
Abstract
Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA) are rare primary headaches that can sometimes present with a status like pattern which can be highly disabling. Intravenous (IV) lidocaine has been reported to be useful in status like SUNCT but its use in status like SUNA remains unexplored. We report a patient of episodic SUNA who despite on multiple conventional drugs had status like presentation. He had an excellent sustained response to IV lidocaine. Relevant literature on treatment of status like SUNCT/SUNA is briefly reviewed. IV lidocaine can be a very useful treatment for status like SUNA.
Keywords
Introduction
Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA) are characterized by sudden brief attacks of severe unilateral head pain in orbital, periorbital, or temporal regions, accompanied by ipsilateral cranial autonomic symptoms. The frequency of attacks is highly variable and may be as low as one attack every other day to multiple attacks per day. A status like presentation in SUNCT is known to occur rarely in which attacks are so frequent (>30/h) that the pain persists for the better part of day and can be extremely disabling. 1 However, status like presentation in SUNA has not been described so far to the best of our knowledge. Because of the ultra-short duration of the pain, acute treatment has largely been unsatisfactory, and the only promising drug is sodium channel blocker lidocaine given as an intravenous (IV) infusion. Although use of lidocaine in status like SUNCT and in some patients of frequent SUNA is documented, its use in status like SUNA is unknown. We describe a patient with status like SUNA who had almost continuous painful paroxysms throughout the day which were completely relieved by IV lidocaine.
Case report
A 48-year-old right-handed male presented to us in March 2017, with history of recurrent episodes of headache of 3 years duration. A typical attack was characterized by severe right hemicranial pain, localized to the orbital, periorbital, and frontal regions that lasted for 3–5 min. Each attack consisted of a group of stabs, which were moderately severe and characterized by the patient as moderately severe (6 on visual analog scale of 1–10), making the patient restless and irritable during the attack. The attacks were associated with ipsilateral lacrimation and rhinorrhea but no congestion of the eyes. There were no other cranial autonomic symptoms or signs. There was associated ipsilateral photophobia, nausea, occasional vomiting, and tinnitus but he denied any phonophobia. Initially, the headaches occurred infrequently (2–3 episodes/day) with remissions lasting for a variable period of 2–4 months but subsequently, they become more frequent with 8–10 episodes/day. The attacks were evenly distributed throughout the day, occurring even during sleep (albeit with a lower frequency), causing poor sleep. He reported that attacks were often triggered by chewing, washing his face, flow of air around the face, without any refractory period, and attacks could occur repetitively in the presence of a repetitive stimulus. In between the attacks he was pain free. There were no other comorbidities. A detailed neurological examination was unremarkable. His routine investigations were normal except for a mild microcytic hypochromic anemia (hemoglobin = 11.0 g/dl). A gadolinium-enhanced magnetic resonance imaging with special emphasis on sellar, cavernous, and trigeminal root entry zone areas did not reveal any abnormality and there was no neurovascular contact. A diagnosis of primary episodic SUNA was made and he was started on lamotrigine (50 mg/day gradually increased to 150 mg/day) and pregabalin (150 mg/day). Initially, he reported a significant improvement in his symptoms, with a marked decrease in headache frequency, most attacks occurring only during chewing food. After 3 months in June 2017, he reported back with increase in frequency of attacks, with up to 20–30 attacks/h, each lasting 2–3 min. He was admitted for evaluation, lamotrigine was increased to 200 mg/day and oxcarbazepine was added and up-titrated to 900 mg/day. This resulted in a decrease in attacks over the next week to 1–2 every alternate day. However, in November 2017, he came back with multiple episodes of headache which would occur repeatedly throughout the day almost continuously each with duration of 1–2 min with very little pain-free intervals for past 1 week. In view of the high frequency of attacks (50–60 attacks/h) causing severe disabling pain for better part of the day, a diagnosis of status like SUNA was made (Online Supplemental Video 1). After a 12-lead electrocardiogram, patient was started on IV lidocaine with continuous cardiac monitoring at a dose of 0.5 mg/kg/h that resulted in a significant decrease in the attack frequency to 4 episodes/h. The dose was gradually increased to 1.5 mg/kg/h over the next 24 h and at this dose there was complete abolition of pain. The infusion was continued for 5 days and stopped after the patient was pain free for 3 consecutive days. He was subsequently discharged on pregabalin (300 mg/day), lamotrigine (200 mg/day), and oxcarbazepine (900 mg/day). On subsequent follow ups up to 6 months, patient continued to be pain free (Online Supplemental Video 2).
Discussion
SUNCT and SUNA are two subtypes of short-lasting unilateral neuralgiform headache attacks. While in SUNCT, the ipsilateral autonomic symptoms at a minimum consist of both conjunctival injection and lacrimation, in SUNA either of these two autonomic symptoms is present. 2 It is suggested that SUNCT may be part of SUNA and the later may be under-diagnosed. Although the International classification of Headache Disorders (ICHD)-3 beta criteria require an attack frequency of at least one a day for more than half of the time when the disorder is active, there is a great variability in the frequency of attacks both among individuals and in the same patient. The number of paroxysms may range from a few attacks per day to nearly continuous attacks. Status like SUNCT has been variably defined as a condition with an attack frequency of more than 30/h or nearly continuous attacks that cause pain for better part of the day resulting in an unbearable condition due to the intensity and frequency of the attacks lasting for 1–3 days. 3,4 Our patient met the ICHD-3 beta criteria for episodic SUNA and presented twice with a marked increase in frequency of attacks which occurred almost continuously throughout the day with minimal pain free interval, thus manifesting as status like presentation of SUNA. To the best of our knowledge, status like presentation of SUNA has not been described previously. Status like presentation of SUNCT/SUNA can be extremely disabling as patients may not be able to eat or drink because of frequent, easily triggered, high-intensity pain attacks as was evident in our case also. On one occasion, increase in medication and addition of oxcarbazepine resulted in a significant decrease in frequency of paroxysms, but the second episode was much more disabling that required IV lidocaine. There was a dramatic response to lidocaine and attacks completely abated at a dose of 1.5 mg/kg/h. The response was sustained as he remained completely pain free for 6 months after the infusion. The reason for the increase in the frequency of attacks is not clear, but it has been observed that status like presentation of SUNCT/SUNA does not have an adverse prognostic value and often does not indicate a secondary cause of SUNCT/SUNA. 1 Since SUNCT and SUNA are ultra-short-lasting headaches, acute treatment options for pain are limited. IV lidocaine has been used with variable success in patients with SUNCT status (Table 1). 4 –9 Literature regarding use of lidocaine in patients with SUNA is limited. Cohen reported successful treatment of four SUNA patients with lidocaine but individual details were not provided, although mean duration of attacks was 174 min/day (range 4–1000) and 67 attacks per day (i.e. 3–4 attacks/h). All four patients had remissions lasting for 2 days to 12 weeks. 6 Similarly, Williams and Broadley used subcutaneous lidocaine in two of five SUNA patients with excellent results (>90% reduction in headache frequency and/or severity). 7 However, these patients did not have a status like presentation of SUNA, and to the best of our knowledge, this is the first case report of successful use of IV lidocaine in a patient who had status like presentation of SUNA. Montes et al. tried an IV bolus of corticosteroids (with oral carbamazepine) in one patient with status like SUNCT with encouraging results and this seems to be another treatment option in status like presentations of SUNCT/SUNA. 4
Review of studies using lidocaine in SUNCT/SUNA.
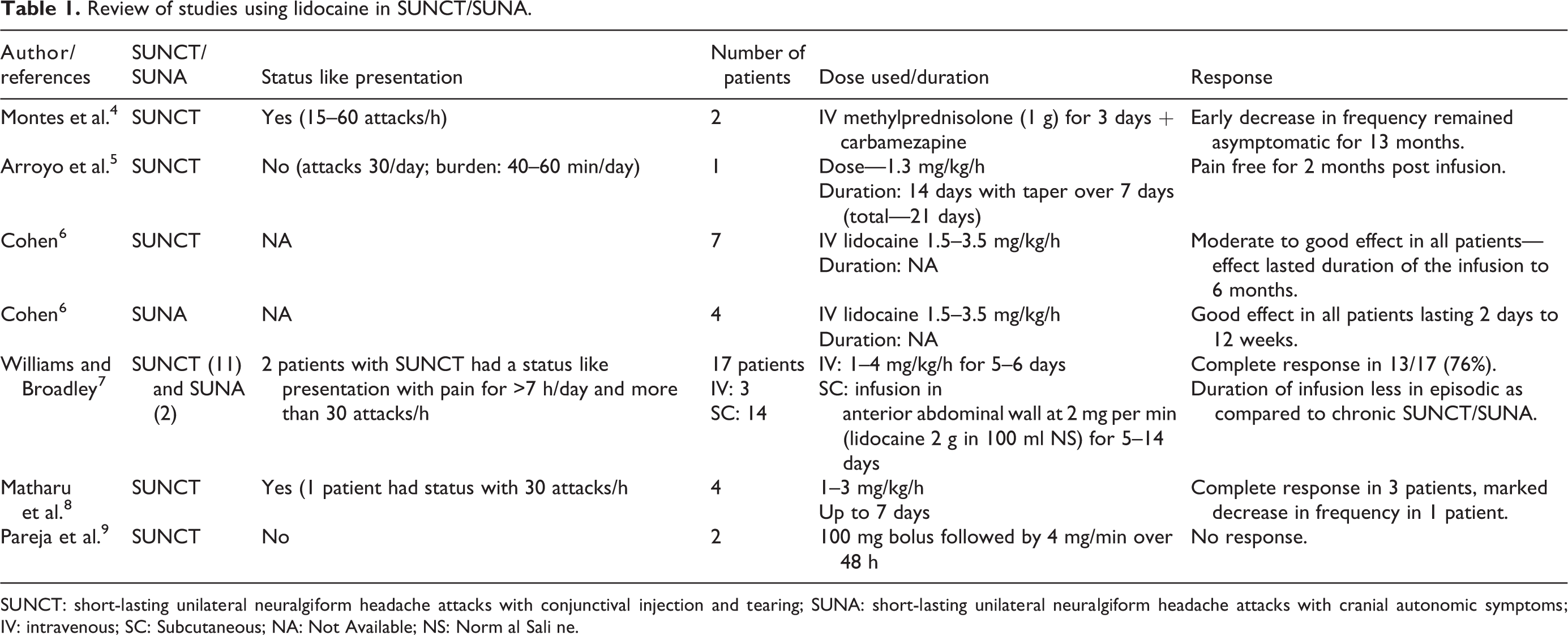
SUNCT: short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA: short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms; IV: intravenous; SC: Subcutaneous; NA: Not Available; NS: Norm al Sali ne.
The main therapeutic use of lidocaine in SUNCT/SUNA is in patients with very frequent, easily triggered, high-intensity painful paroxysms. Additionally, it can also be used as a bridge during titration and optimization of preventive medications such as lamotrigine which need to be introduced in a gradual manner and thus may take time in providing pain relief. 4 However, IV lidocaine administration carries risks and requires careful monitoring, particularly of Electrocardiogram (ECG) and blood pressure, making its regular use difficult. Another problem with IV lidocaine infusion is frequent neuropsychiatric symptoms such as acute depression or paranoia that is usually reversible after discontinuation of lidocaine. Most of the side effects are dose related and frequency is generally low (<1%) except hypotension which can be seen in 15–20% of patients receiving IV lidocaine. 10 Infusion of lidocaine should be used with an aim to suppress or markedly decrease the attacks of SUNCT, because fixed duration infusions of 48 h have not been found to be effective. 9 The total duration of IV lidocaine administration remains unresolved and probably differs from one patient to another but in general infusion should not be given for more than 7 days though rarely some patients may require lidocaine for 14 days. Some authors found that response to IV lidocaine in SUNCT is so convincing that it can be used as a diagnostic test for SUNCT akin to indo test for hemicrania continua and paroxysmal hemicrania. 8
In conclusion, SUNA can present with variable frequency of attacks and a status like presentation may be seen occasionally that can be extremely disabling. IV lidocaine given with proper precautions can be a very useful therapy in patients with status like presentation of SUNA.
Clinical implications
SUNA, a rare type of trigeminal autonomic cephalalgia can occasionally present with very frequent attacks resulting in status like condition. Status like presentation of SUNA is a highly disabling condition. IV lidocaine can provide efficient and long-lasting benefit.
Footnotes
Author contributions
The authors Dr Debashish Chowdhury, Dr Ashish Duggal, Dr Arun Koul and Dr Ankur Gupta have contributed equally in the management of the reported patient and preparation of the manuscript.
Informed consent
Informed consent was obtained from the patient reported in this case report. Informed consent was also taken for the use of video for educational purposes.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.