
Abstract
Nummular headache (NH) is an unusual disorder attributed to a dysfunction of the epicranial nerves. We report a new series of cases, highlighting some clinical features, the association with other headaches, and the therapeutic response. Data of patients with NH, fulfilling ICHD-3 criteria, observed in a Headache Outpatient clinic during 5 years, were retrieved from records. Response to onabotulinumtoxinA was recorded prospectively and evaluated with a Headache Impact Test (HIT). Twenty-four patients, aged 53.8 (±14.6) years at diagnosis, 13 women, had definitive (N = 21) or probable (N = 3) NH for an average of 2.4 years. Headache was consistently localized, more frequently extratrigeminal (N = 15) and parietal, and confined to the scalp. Pain was unremitting since onset in 58.3% of mild-to-moderate severity often with superimposed paroxysms (66.7%) and local allodynia (70.8%). In five cases, there was a possible precipitant. Thirteen patients reported other headaches, preceding NH by 8.2 years. In eight persistent cases, there was a significant improvement on HIT, after onabotulinumtoxinA. Despite its persistence, NH may go unrecognized for years. It often follows other headache types and has some tropism for hair-covered regions of the scalp. OnabotulinumtoxinA seems effective in persistent cases.
Introduction
Nummular headache (NH) is an intriguing primary headache disorder that develops and persists without evident cause in a very circumscribed region of the scalp. 1 The size and shape of the painful region prompted the term nummular on its first description by Pareja in 2002, 2 because it reminds the configuration of a large coin.
The pathogenesis of NH is not known, but its quality suggests a neuropathic origin, 3 since it is often described as a superficial burning pain with local hyperesthesia/allodynia, hypoesthesia, dysesthesia, and superimposed paroxysms, which is typical of lesions of the small peripheral nerve fibers in any part of the body. 4 However, some evidence questions this neuropathic hypothesis. Firstly, because it can be associated with intracranial lesions 5 –7 and can be aggravated by Valsalva maneuvers, sexual activity, or the menstrual cycle, triggers that involve intracranial mechanisms. 8,9 Secondly, because the pain does not follow the typical topography of a peripheral nerve territory nor does it respond to local nerve blocks. It has a round or elliptical shape with sharp contours that suggest a circumscribed local process (akin to the one observed in nummular eczema and other skin disorders). Furthermore, it seems to have some tropism for the extratrigeminal territory. In fact, to the best of our knowledge, there are almost no reports of NH in the forehead or face, which is different from nerve injury caused by infection (herpetic neuralgia), trauma, entrapment, or vascular contacts. Although there are reports of secondary forms of NH 8 or its association with autoimmune biomarkers, 10 it usually develops in the absence of any local pathology and reported local biopsies have been negative. 11
So far there is little evidence for the treatment of this disorder. 12 While most publications mention therapeutic response to neuromodulators, 8,12 –15 there are also reports of improvement with onabotulinumtoxinA. 16 –19
We describe a new series of patients with NH highlighting three features: (1) its frequent association with other headaches, often preceding NH for several years and sometimes affecting the same anatomical region; (2) its preferred localization to regions of the scalp with hair, which seems to be the large majority in published cases, and (3) its response to onabotulinumtoxinA.
Methods
Cases with the clinical diagnosis of NH, observed in the last 5 years in the headache outpatient clinic of a University Hospital by one of the authors, were retrieved from the records. Clinical data were reviewed and checked for the diagnostic criteria of International Classification of Headache Disorders (ICHD-3) for NH. 1 Patients fulfilling the diagnosis of probable or definite NH were included and analyzed regarding demographic features (age at consultation, gender, and age at pain onset), headache characteristics (lateralization, localization, size, pain character, superimposed paroxysms, and response to treatment), associated disorders (namely other types of headache or other neurological disorders), and findings on physical examination and imaging studies. Whenever an underlying disorder was found in close temporal or possible causal association with the onset of headache, we classified NH as triggered (temporal association) or secondary (if there was a temporal and causal relation between the two). Patients who had not been observed in the last 6 months were contacted by telephone and invited for a follow-up visit, after informed consent.
Treatments directed at NH were recorded and therapeutic response was classified in three categories, according to the clinical notes: 1—no response, 2—partial improvement and 3—excellent response, patient reports feeling much improved or without pain. Patients with persistent pain who failed or presented adverse events with oral therapies or were unwilling to maintain oral treatment were referred for onabotulinumtoxinA according to a “follow the pain” protocol consisting of five to seven points of five units (total 25–35 units) on the site of pain (one in the center and four to six equidistant points, at the periphery of the site of pain), after written informed consent. Patients receiving toxin were studied prospectively and recorded the impact of headache, before and at least 1 month after the treatment using the Headache Impact Test (HIT). 20 Session repetition was performed on demand every 3 months.
The study protocol was approved by the joint Hospital and Faculty Ethics Committee of the Institution.
Results
Clinical data
Twenty-eight cases were retrieved from a sample of about 2500 patients with headache, and 24 fulfilled the ICHD-3 diagnostic criteria. Three subjects with localized pain were excluded because they did not conform to current diagnostic criteria and another case because of an associated basalioma of the scalp. At first visit patients’ age was, on average, 53.8 (±14.6) years, ranging between 31 years and 79 years, and there were 13 females. The first symptoms began by the age of 50.3 years (±15.2, range 23–75), resulting in an average duration of symptoms of 2.4 years (29.3 ± 26.2 months). No patient had been previously diagnosed as NH. The majority (n = 21) fulfilled the ICHD-3 criteria for definite NH, and the remaining for probable NH mostly due to missing data on records (Table 1).
Patients’ data and headache features.

NR: not recorded; post: posterior; sup: superior; ant: anterior; NH: nummular headache.
Pain was lateralized in all cases, 12 on each side of the head, and the painful area crossed the midline, by less than 1 cm, in 3 subjects. Headache was located outside the cutaneous territory of the trigeminal nerve in two-thirds of patients (N = 15). The pain was more frequently felt in the parietal region (N = 15), exclusively or in part, followed by the temporal (N = 4), the occipital/retroauricular (N = 3) or the frontal (N = 2) regions. In all cases, the affected area was restricted to the scalp, entirely (23) or partially (1) in hair-covered regions, although one patient was partially bald.
The affected area was round in 14 and elliptical in 9 cases. The larger diameter ranged between 1 cm and 6 cm, with an average of 3.2 cm. The pain was persistent and continuously felt in 14 and intermittent and relapsing in 9 patients. The latter did not describe any type of periodicity, reporting phases of hours or days with pain alternating with pain free periods of days or weeks. In no case was the background pain described as recurrent short-lasting attacks. Most patients (n = 16) described superimposed paroxysms of pain ranging from one episode every other day to 15 a day. The majority (N = 17) had hyperesthesia/allodynia in the affected region, where light touch was felt as painful. Rarely (n = 2) there was a decrease of sensation on the affected area. Pain intensity was variable. Most patients considered the baseline pain of mild intensity, but paroxysms were considered severe (Table 1). Neuroimaging (10 computed tomography (CT) and 5 brain MRI) was reviewed in all but four patients and was considered normal.
In five cases, NH was related with a possible trigger. Three patients reported minor local trauma, without loss of consciousness, that were somehow temporally coincident with the onset of pain (in one case 3 months later), the localization of trauma was believed to be coincident with the painful region but was not recorded. One patient had suffered an accident with an extensive trauma to the scalp in childhood and NH developed some 40 years later. Finally, a female patient had an osteolytic tumor of the skull (eosinophilic granuloma) that was surgically removed. She had a localized pain over the granuloma region but later developed an identical pain, with features of NH, on the contralateral symmetrical point of the scalp, not corresponding to any skull lesion.
Other headaches
Thirteen (54.1%) patients, seven women, had other types of headache (Table 2). In most cases, these began several years before the onset of NH, on average 8.2 (±12.1) years before, and were easily distinguish from NH. Seven cases initially requested the consultation because of other headache types, and NH was found in the anamnesis or in the follow-up. The type of headache was not uniform. Five subjects (three women) had episodic migraine, one with aura. One man had suffered from typical episodic cluster headache since the age of 34 years but had been in remission for 10 years by the time he developed NH at 54 years of age. Interestingly, NH developed exactly in the same location as previous cluster attacks. Three patients had tension type headache, one chronic and more marked on the side of NH. One woman had occasional attacks of trigeminal neuralgia involving the second territory of the trigeminal nerve, ipsilateral to extratrigeminal NH. One man had a burning mouth syndrome that was much more incapacitating than NH. A young athlete had a unilateral primary exertional headache that had been investigated 1 year before and was ipsilateral to newly developing NH. An elderly patient had occasional paroxysms of ear pain, with red ear, that occurred independently of the continuous mastoid burning pain with hyperesthesia/dysesthesias of NH.
Previous headaches.

NH: nummular headache.
Therapeutic response
Patients received different therapies, before or during their observation in the Headache Clinic (Table 3). Neuromodulators were the most commonly prescribed drugs and were selected according to patients’ age, associated disorders, and profile of drug adverse events. A few patients did not try any specific treatment for this headache because it was mild or intermittent or because they were reluctant to maintain a permanent medication for a localized pain.
Therapeutic response.a

AT: amytriptiline; Botox: onabotulinumtoxinA; BZD: benzodiazepines; CBZ: carbamazepine; GBP: gabapentine; NSAID: nonsteroidal anti-inflammatory drugs; PGB: pregabaline; Venlaf: venlafaxine.
a Therapeutic response is coded as: 1—no response, 2—partial improvement, and 3—excellent response, patient reports feeling much improved or without pain.
Regarding neuromodulatory therapies, 16 patients underwent treatment with gabapentin. Partial therapeutic response was observed in nine patients and very good in one with no effect in the remaining. Among four patients taking carbamazepine, three reported either a partial (N = 2) or an excellent (N = 1) response. Pregabalin was given to six patients, of whom only one had partial therapeutic responses. Valproate, lamotrigine, and flunarizine were prescribed to one patient each, without pain control. Eleven patients were prescribed amitriptyline and four reported benefit.
Eight cases (4 females, 56 years of age, ranging between 34 and 79 years), with persisting pain, and not responding to oral medication were treated with onambotulinumtoxinA on the affected region. There were no adverse events, except for pain during the injection, particularly in patients with local hyperesthesia. Therapeutic response was monitored through the headache impact scale (HIT-6) at baseline (before the first session), in two follow-up times after the first session, and at each subsequent treatment sessions (eight patients received one treatment session, six received two sessions, four had three, and two patients had four sessions). HIT-6 scores are summarized in Table 4, showing data from baseline, 3 months (on average) after first treatment and at the second, third, and last sessions (independently of the number). Since this treatment was repeated initially on demand, some patients received the second treatment more than 3 months after the first one. There was a significant decrease of HIT-6 scores comparing baseline with first follow-up 1 (p = 0.008) and baseline with last session (p = 0.027; Wilcoxon, paired samples test). Only one patient did not show significant improvement (patient 8).
HIT scores in patients treated with onabotulinumtoxinA.

NR: not recorded; SD: standard deviation; HIT: Headache Impact Test.
Discussion
Multicentric data are essential to gather information about new clinical entities, in particular when they are uncommon. In this report, we describe a new series of 24 patients with NH observed in a tertiary Headache Center. They correspond to a small percentage of cases observed in the Headache clinic (about 0.96%), and none had a previous diagnosis of NH, despite a persisting pain for several months duration, showing that this entity is probably unknown to primary care or other physicians.
Clinical features were identical to those described by Pareja in 2002 2 and in other series. 21 –23 Pain was strictly localized and the painful site was very consistent between observations. It was more often described as burning or “wound-like” superficial pain in the scalp, of mild or moderate severity with fluctuating intensity, and with superimposed paroxysms of severe stabbing/sharp pain. It was continuous and unremitting in most cases, or episodic and recurrent in the same location, in others. The affected region did not show cutaneous abnormalities but was very tender to light touch, to pressure and to painful stimuli, with allodynia only in the affected region. Two patients presented a localized loss of cutaneous sensation, suggesting an involvement of the sensory nerve terminals. All these features support the hypothesis of an epicranial or strictly scalp cause.
Of interest is the fact that in all cases the pain was felt in areas of hair implantation. Although in most published series the exact location of pain is not shown, the most frequent localization is extratrigeminal, parietal or temporo-occipital, and the least common is frontal. In publications with drawings or photographs of patients it is always depicted in areas with hair, and to the best of our knowledge, there have been few reports of NH in the forehead 24 or the anterior temporal region 25 but never in the face. This raises the hypothesis of the involvement of hair follicles nerve plexus (rich in sensory afferents and sympathetic fibers) or other follicular structures in the origin of pain. Interestingly, there is a report of a patient with a hair heterochromia and another with alopecia areata in the affected region. 26 –29 These may correspond to trophic changes associated with the pain. The patient with a documented co-localized alopecia areata improved with botulinum toxin and later recovered from alopecia. 29 A recent study found a high prevalence of autoimmune disorders in these patients, disorders that often affect the skin. 10 Although hair follicles are widespread in human skin, there are differences between vellus hair that covers most of the body and scalp hair. 30 Scalp follicles have a higher density, extend into the hypodermis (as opposed to the dermis), have a longer cycle, and have larger neurovascular bundles than in other skin regions, which may make them more vulnerable to specific disorders.
In the present series, the majority of cases of NH were considered primary. Although some patients attributed the pain to a local trauma the relation between the traumatic episode, and the onset of pain was not clearly documented. In fact, patients often did not recall well the site of trauma making the relation difficult to establish. It is possible that some of these cases are primary and should not be classified as post-traumatic types of headache. One patient had an eosinophil granuloma surgically removed from the skull, but the initial pain, felt in the region overlying the granuloma, disappeared and NH developed in the other side of the scalp. Both eosinophilic granulomas and multifocal pain have been described in other cases of NH. 27,28,31 In the present series, there were no cases with intracranial lesions.
Thirteen patients had other headaches of different types, mostly primary or neuralgic. There were also rare disorders associated with peripheral nerve dysfunction such as the burning mouth syndrome. Of particular interest is the case with a long-standing history of typical cluster headache that developed NH in exactly the same site of usual cluster episodes, deep in the left temple. The association between NH and other headache disorders has been described in other series, with a percentage ranging between 17.4% and 56% of cases (see Table 5 for a revision of series with 10 or more cases 2,10,21,32 –35 ).
Review of associated headaches.a
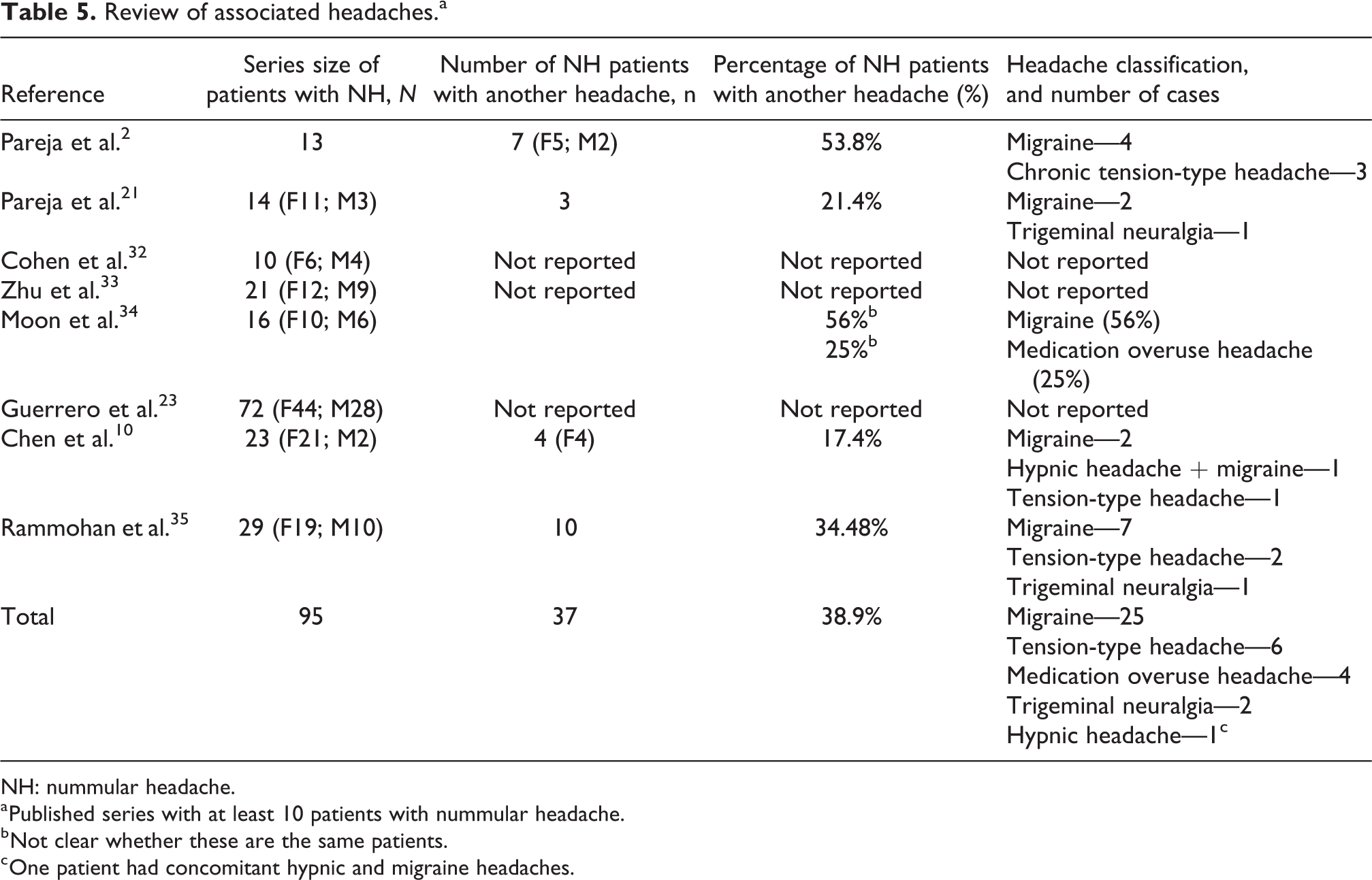
NH: nummular headache.
a Published series with at least 10 patients with nummular headache.
b Not clear whether these are the same patients.
c One patient had concomitant hypnic and migraine headaches.
The type of associated headache has not been uniform. The majority are primary headaches that begin before the development of NH. This may have different explanations. It may indicate either that a primary headache can be causally associated or facilitate the development of NH, through recurrent allodynia or other peripheral mechanisms. Alternatively it may correspond to a referral bias. In fact, seven patients were referred because of other headaches and the diagnosis of NH was made in addition to it.
Therapeutic response to antiepileptics and tricyclic antidepressants was instantiated on the basis of the neuropathic theory of NH. However, the results were not satisfactory in many patients. OnabotulinumtoxinA was tried, because of previous evidence suggesting its efficacy 12 and also its safety and local action on sensory nerve terminals. There was a significant improvement in HIT-6 scores after the first procedure and 6 patients were willing to repeat the treatment. This contrasts with reports showing that local anesthesia is ineffective in NH. 12
We acknowledge limitations to this report namely the retrospective collection of data and the limited number of patients, especially those referred for toxin. Besides, we did not collect data regarding pain intensity in a visual analog scale (VAS) scale or the percentage of reduction of pain with treatments.
Conclusion
NH is a rather uncommon and undiagnosed primary headache. While most of its features favor an epicranial neuropathic mechanism, its preference for the hair-covered scalp regions may suggest the participation of hair nerve terminals. Other types of chronic headaches are frequent in these patients. While we cannot discard a referral bias, this association needs further study since it raises the possibility of a central facilitation for a peripheral pain. Persistent cases may respond to onabotulinumtoxinA treatment.
Clinical implications
Nummular headache is an unusual and unrecognized disorder that must be considered in patients with localized headaches.
Chronic cases may improve with local injections of botulinum toxin.
Footnotes
Acknowledgements
The authors thank Professor Luis Soares de Almeida for providing critical information regarding skin pathology.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Isabel Pavão Martins has participated in Allergan and Novartis Advisory Boards and has received travel support from Allegan. Luis Abreu reports no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.