
Abstract
Keywords
Introduction
Diffuse large B-cell lymphoma (DLBCL NOS) is presented with large, transformed B cells with a high proliferation fraction and a diffuse growth pattern. DLBCL NOS is responsible for 40% of all non-Hodgkin lymphoma (NHL) cases. 1 It has a moderate male predominance, with a 65-year-old average age at presentation. 2 About 33% of the patients with DLBCL NOS present with stage “I “or “II” disease, 3 with bulky disease (tumor size > 7.5 cm) in about one-third of these patients. 4 DLBCL NOS has numerous subtypes, and most DLBCL NOS cases are still considered not otherwise specified (NOS). 5 One or more B-cell markers, such as (CD19, CD20 and CD79a) and surface immunoglobulin, can be expressed in 50% to 75% of DLBCL NOS cases. 6
Many factors, including age, performance status (PS), constitutional symptoms, serum 2-microglobulin, lactate dehydrogenase (LDH), and albumin levels, significantly impact DLBCL NOS patients’ survival. The size of the tumor, Ann Arbor stage, and extranodal and BM involvement are all factors to consider.7,8 The International NHL Prognostic Factors Project created the international prognostic index (IPI), assigning one point to each of the following negative prognostic factors: older than 60 years, Ann Arbor stage III to IV, two or more extranodal site involvement, PS 2 or higher, and serum LDH level above the normal high level. The newly designed therapies resulted in the emergence of the less complex revised IPI (R-IPI) with a more remarkable ability to detect patients’ long-term outcomes. The National Comprehensive Cancer Network (NCCN) database was used to create the latest and most detailed NCCN-IPI scoring system.9,10
Epithelial markers are being studied extensively in NHL to investigate significant relationships to prognosis and to aid in tumor-tailored targeted therapies. One of these markers is carbohydrate antigen 125 (CA-125), produced by serous membranes mesothelial cells, colonic and gastric mucosa and cells originating from the female genital tract celomic epithelium. 11 This serum marker is expressed in various gynecologic malignancies and is used to track the progression in ovarian cancer patients.12,13 Furthermore, studies showed elevated serum CA-125 levels in NHL patients; specifically, DLBCL NOS, had a significant adverse prognostic factor and poorer survival, implying that CA-125 could indicate the prognosis of NHLs. 14 CA 19-9, another member of carbohydrate antigens, is useful mainly as a marker for digestive system malignancy with remarkable sensitivity and specificity in diagnosing pancreatic cancer. 15
This study tries to determine the possible expression of CA-125 and CA 19-9 in nodal DLBCL NOS tissues using immunohistochemistry (IHC) and the possible relation of such expressions to clinicopathological features and patient survival.
Materials and Methods
Samples
Patients' files, as well as H&E and IHC slides of all diagnosed cases of DLBCL NOS between 2018 to 2022, were reviewed at the surgical pathology lab of the Oncology Center at Mansoura, Egypt, and consent is not applicable. Cases with insufficient clinical information and those diagnosed solely based on Tru cut or Fine Needle Aspiration Cytology (FNAC) were excluded. Sixty-five cases met the selection criteria. The patients received no neoadjuvant therapy.
Clinical Parameters and Histopathological Evaluation
All cases` clinicopathological data were re-examined, including H&E and IHC slides. Age, gender, histological type and stage, location, extranodal involvement of the spleen and BM, presence of bulky disease, anemia, serum LDH level (n ≤ 450 U/L) and response to therapy are among the information provided. Furthermore, the performance status was assessed using the Eastern Cooperative Oncology Group (ECOG) scoring system 16 in conjunction with the international prognostic index (IPI) scoring, with scores of 1&2 considered low and 3&4 considered high. 17 All patients were followed up for 60 months following the surgery to evaluate the prognostic value of CA-125 and CA 19-9 expression. The overall patients’ survival (OS) was calculated from the time of disease diagnosis till the time of disease-specific death or the last follow-up. Disease-free survival (DFS) was defined as the period from the primary surgery to the documented relapse, recurrence or distant metastasis.
Tissue Micro-Array (TMA)
Manual TMA blocks were made using the modified mechanical pencil tip method described previously. 18 Multiple 0.8 mm diameter cores were punched out from each case paraffin block and inserted into the newly formed TMA blocks. Multiple standard tissue cores were also inserted as positive and negative internal controls. TMA block sections (4 µm thickness) were prepared for routine hematoxylin and eosin (H&E) staining. Other sections were prepared for IHC on charged slides.
Immunohistochemistry (IHC)
Deparaffinized 4 µm thick sections were incubated in 0.3% H2O2 in methanol for half an hour before being microwave-heated for another half an hour in an EDTA buffer solution (pH 8.0). The indirect immunoperoxidase technique was applied by using monoclonal mouse anti-human CA 19-9 Ab (Clone 121SLE, Cat. #760-2609, predilute ready-to-use for IHC, Ventana) and monoclonal mouse anti-human CA-125 Ab (Clone OC125, Cat.# 760-2610, predilute ready-to-use for IHC, Ventana). Each primary antibody was allowed to react at room temperature for 30 min. Then, the immunoperoxidase method was performed using Immuno Pure Ultra-Sensitive ABC Peroxidase, and diaminobenzidine was used as the chromogen.
Evaluation of IHC
CA 19-9 and CA-125 expressions were evaluated semi-quantitatively in each case. Cases were excluded from the analysis if the tissue core contained no recognizable tumor or if the tissue core was lost during processing. Two authors scored all TMAs independently, and any discrepant readings were re-scored to arrive at a consensus score for each core. Because the expression of both markers is abnormal in DLBCL NOS, cases were classified as negative or positive for data analysis. According to Gui et al, The case was considered positive if positive cells were more than 10%. 19
Statistical Analysis
SPSS version 24.0 for Windows (SPSS Inc, IBM, Chicago, Illinois) was used to analyze the collected data. The Chi-square (χ2) test was used to examine the relationship between each marker's expression and clinicopathological and histological parameters. The Kaplan-Meier test was used to analyze survival data, and the log-rank test was used to compare survival curves. A 2-tailed P ≤ .05 was considered significant in all tests.
Results
Sixty-five cases of DLBCL NOS were obtained from the surgical pathology lab between 2018 to 2022. These cases’ clinicopathological and histological features are listed in Table (1). There were 37 samples from male patients (57%) and 28 from female patients (43%). By DLBCL NOS presentation, the patient's age range was 22 to 83 years (mean, 53.82, SD ± 13.6 years). There was no difference in the mean age of males and females at the presentation. At the time of lymphoma presentation, 83% of the patients (54) were 40 years or older.
Thirty-one patients (48%) had spleen involvement, while only 6 (9%) had BM involvement. On the other hand, 19 patients (29%) had extranodal involvement, and 12 (19%) had a mass measuring 10 cm or more. Fever, night sweats, and weight loss were all reported in 17 patients (26%). Our result noted that 22 patients (34%) were anemic at the time of presentation. The LDH level was elevated in 61 patients (94%). According to PS, 51 of the patients were classified as being in PS 1 (79%), ie, they were nearly fully ambulatory but still had symptoms. Following this group were 13 patients in PS 2 (20%) and just one in PS 3 (1.5%). 40 patients (62% of them) also had low IPI.
Moreover, according to staging, seven patients were in stages I and II (11%), 31 of the patients were in stage III (48%), and 20 were in stage IV (31%). However, in response to the therapy, the disease regressed in 34 patients (52%), remained stationary in 16 patients (25%), and the disease progressed continuously in 15 patients (23%).
Table 1 and Figure 1 show abnormally-expressed CA 19-9 in 8 (12%) of the cases, whereas CA-125 was not expressed. A significant association between anemia and PS 1 was found in 75% of the cases with CA 19-9 positive results (P = .009 and P = .024, respectively). Although 75% of the cases with CA 19-9 positive results were in female patients, this method couldn't reach statistical significance (P = .052).

(a) Aberrant CA 19-9 cytoplasmic staining in a case of DLBCL NOS (b) Negative CA-125 expression in a case of DLBCL NOS (x200).
Clinicopathological and Histological Features of 65 Cases of DLBCL NOS.

Results are presented as numbers and percentages from the total (in brackets).
Aberrant positive.
Table 2 showed no statistically significant relationship between CA-19-9 expression and other clinicopathological factors.
Relation of CA 19-9 Expression to Clinicopathological and Histological Features of DLBCL NOS Cases.
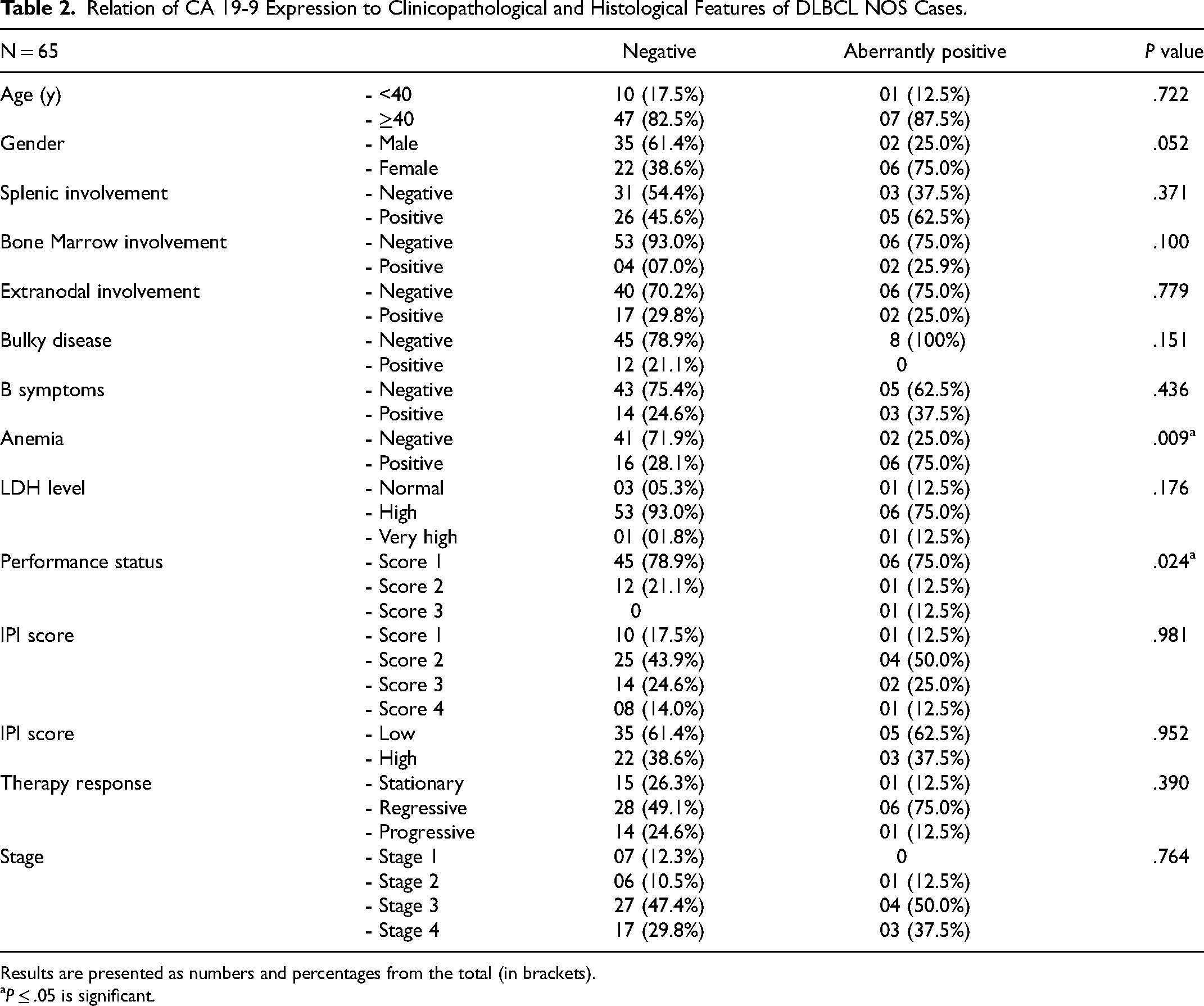
Results are presented as numbers and percentages from the total (in brackets).
P ≤ .05 is significant.
In cases with aberrant CA 19-9 positivity, the overall survival median was 18 months as opposed to 43 months in cases with negative CA 19-9 positivity (P = .879) (Figure 2). Therefore, CA 19-9 expression is not a reliable predictor of prognosis in DLBCL NOS patients.

Relation of CA 19-9 expression to overall survival in DLBCL NOS cases.
Discussion
DLBCL NOS is the most prevalent type of adult NHL worldwide, accounting for about one-third of all NHLs. 20 Patients with DLBCL NOS typically have an average age of 65, and the disease has a very low prevalence in men. 21 In most instances, DLBCL NOS can express one or more B-cell CD markers. 22 Furthermore, it was frequently discovered that specific epithelial markers, like CA-125, were elevated. A reliable marker for staging, determining the disease activity, and tracking the patient's response to therapy, serum CA-125 has been found in prior studies to be elevated in about 45% of DLBCL NOS patients.11,23 Other research found a link between elevated serum CA-125 levels and treatment failure and relapse, reduced complete remission, aggressive behavior, advanced disease stage, aggressive histology, mediastinal and abdominal involvement, extranodal extension, and presence of effusion.24,25 However, in all previous studies, CA-125 serum levels were examined rather than IHC expression in general NHL and DLBCL NOS. It is necessary to re-evaluate serum CA-125 levels in DLBCL NOS cases; as in the current study, we did not detect any expression of CA-125 in DLBCL NOS tissues, indicating that serum levels are not always related to protein expression.
Cancer antigen 19-9 (CA 19-9, sialylated Lewis antigen) is a tumor marker suggested to be utilized during the investigation of pancreatic cancer patients. Reports showed 80% and 90% sensitivity and specificity of CA 19-9 for those patients. 26 The major limitation of using CA 19-9 in this setting is that it may be markedly raised in numerous other forms of gastrointestinal cancer, such as colorectal, esophageal and hepatocellular carcinoma. CA 19-9 can also be detected in other cancerous organs, such as the liver, lung, breast, and others.27,28
Although there have been several reports of unusual gastrointestinal DLBCL NOS presentations, obstructive jaundice, and high CA 19-9 levels have never before been documented. 29 Abdominal pain, weight loss, and obstructive jaundice are frequently accompanied by elevated CA 19-9 levels in cases of advanced pancreatic carcinoma but not in cases of DLBCL NOS. 30 There was only one unusual case of advanced gastrointestinal DLBCL NOS, which had symptoms of obstructive jaundice and mimicked pancreatic adenocarcinoma by expressing extremely high levels of CA 19-9. 29 However, all prior research on gastrointestinal NHLs focused on serum levels of CA 19-9 rather than IHC expression made it necessary to investigate the actual rates of CA 19-9 protein expression in these tumors to understand the expected clinicopathological relationships. To our knowledge, neither the serum nor IHC expression levels of CA 19-9 in cases of nodal DLBCL NOS have been examined.
According to one study, CA 19-9 and other serum markers like CRP, LDH, and bilirubin are prognostically significant pathological features in cases with advanced pancreatic cancer. 31 In contrast to pancreatic adenocarcinoma, which has high CA 19-9 levels in nearly 80% of cases, another study found elevated LDH levels in patients with primary pancreatic lymphoma (PPL) but not in those with high serum CA 19-9 levels. 30 Another study found that some biomarkers, such as albumin, CA19-9, CRP, and LDH, are predictive of poor survival but not chemotherapy response. 32 As with CA-125, all previous works focused on serum levels rather than IHC expression of CA 19-9 in extranodal NHL. However, CA 19-9 expression was detected in 12% of nodal DLBCL NOS cases.
According to our findings, 75% of cases had a positive correlation between CA 19-9 and anemia and PS 1. Anemia is frequently presented in NHL patients, particularly in DLBCL NOS. 33 Tisi and colleagues 34 investigated the relationship between anemia and erythropoiesis regulators in DLBCL NOS patients. They discovered that the patient's Hb concentration ranged between 7.3 and 15 g/dL (average of 11.5 g/dL). Data also revealed that 64% of patients were anemic. As predicted, this low average Hb concentration finding was conveyed in both cases of B-symptoms and cases with age-adjusted IPI scores 1. However, BM infiltration did not play a role due to the absence of significant differences in Hb content between patients with BM infiltration and those that did not.
In contrast, Hong and colleagues 35 investigated the prognostic value of anemia in DLBCL NOS treated with R-CHOP immunochemotherapy and concluded that baseline anemia does not appear to be a consequence manifested by malnutrition and/or impaired PS. It appears to be a biomarker indicating the risk of early death caused by treatment toxicity and rapid deterioration due to disease worsening or later relapse. Some may argue that anemia is an unintended consequence of BM involvement, a significant prognostic factor in DLBCL NOS.36,37 Our findings agree with the first opinion. However, CA 19-9 expression in DLBCL NOS cases was associated with anemia and PS but not with BM or extranodal involvement.
A previous study found a link between serum CA 19-9 level and PS score 1 in patients with unresectable pancreatic cancer, which is similar to our findings. 38 Moreover, other studies reported that patients with higher preoperative CA 19-9 levels had a lower chance of survival, whereas patients with lower post-operative CA 19-9 levels had a higher chance of survival. As a result, they concluded that PS, response rate, and decreased CA 19-9 serum levels were significant prognostic factors.39,40 Other studies have found a significantly improved survival in patients with advanced pancreatic tumor who have lower serum CA 19-9 levels, consistent with these findings.41,42 In contrast, in another study, the tissue over-expression of CA 19-9 in DLBCL NOS was not associated with therapy response or patient survival. 43
Limitations of the Study
As DLBCL cases are so heterogeneous, a larger number of cases is required for more confirmation and validation of our results that are of diagnostic significance in cases of undifferentiated tumors or metastasis of unknown origin.
Conclusion
Because CA-125 was not expressed in nodal DLBCL NOS tissues, studies of serum CA-125 levels in DLBCL NOS patients rather than all NHL patients are required. CA 19-9, on the other hand, was found to be abnormally expressed in 12% of nodal DLBCL NOS cases and to have a significant relationship with anemia and PS-1 but not with survival. CA 19-9 expression in DLBCL NOS patients is not a prognostic factor. As a result, more research is required to determine the possible relationship between serum and tissue CA 19-9 levels and other clinicopathological features of DLBCL NOS patients with nodal and extranodal involvement.
Footnotes
Acknowledgements
The authors would like to express gratitude to all the staff who provided administrative and technical support, particularly Dr Sahira Jilan Al-Nahari at King Faisal Specialist Hospital & Research Center and Dr Shahad Daifalla Al-Sulaimani at King Fahad General Hospital, Jeddah, for their extraordinary efforts.
Authors’ Contribution
All authors read and approved the manuscript. Research conception and design: AAMF, KAAE and ETE; experiments: AAMF, KAAE and ETE; statistical analysis of the data: AAMF and HIS; interpretation of the data: AAMF, TA, HIS, WMA and ETE; writing of the manuscript: AAMF, KAAE and HIS; work revision and final approval: AAMF, TA, WMA and HIS.
Availability of Data and Material
The dataset generated in the current study is available from the corresponding author on demand.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the members of the Medical Research Ethics Committee, Institutional Review Board (IRB), Faculty of Medicine, Mansura University, Mansura, Egypt, with Code No.: R.22.12.1969.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.