
Abstract
Individuals with rheumatoid arthritis (RA) continually fall short of treatment targets using standard drug therapies alone. There is growing evidence that emphasizing physical and mental wellness is equally crucial for improving functioning among people with RA. The purpose of this formative study is to examine the feasibility of offering the wellness-based intervention (“KickStart30”) in patients with RA. Thirteen individuals with RA on targeted immune modulators (a biologic or JAK inhibitor) enrolled in the KickStart30 program. Participants completed self-report measures of RA-specific disability (eg, pain) and other functional areas (eg, mood) in a pre- versus post- intervention design. Paired samples t-tests (and Related-Samples Wilcoxon Signed Rank Tests for non-normal distributions) detected statistically significant results for 10 of 12 measures, including reductions in pain (M = 4.54 to M = 3.54; p = .025; BPI), functional disability (M = 0.94 to M = 0.73, p = .032; HAQ-II), cognitive and physical dysfunction (M = 25.46 to M = 13.54, p < .001; CPFQ), depressive symptoms (M = 9.31 to M = 5.54, p = .003; PHQ-9), anxiety (M = 5.69 to M = 3.23, p = .005; GAD-7), insomnia (M = 11.62 to M = 17.32, p = .007; Note: higher scores on the SCI indicate less insomnia), stress-related eating (M = 75.46 to M = 84.54, p = .021; Note: higher scores on the EADES indicate less stress-related eating), along with significant increases in mindfulness (M = 62.54 to M = 67.85, p = .040; MAAS), mental wellness (M = 4.46 to M = 5.69; HERO), and well-being (Md = 8.00 to Md = 5.00, p = .004; WHO-5). All significant measures had medium to large effect sizes (Cohen's d). The study gives preliminary support for the possibility that the adjunct intervention may have an effect.
Introduction
Rheumatoid arthritis (RA) affects more than 1.3 million Americans, the majority (75%) of whom are women. 1 Whereas the exact etiology remains unknown, RA is an immune-mediated inflammatory disease that likely stems from a combination of genetic predisposition and environmental/lifestyle factors.2,3 RA may result in progressive joint damage with loss of function, in addition to extra-articular comorbidities such as anemia, cardiovascular disease, and osteoporosis. 4 Other significant impairments include fatigue, anxiety, depression, cognitive dysfunction, and reduced quality of life.1,5,6
The development of targeted immune modulators (TIMs) has resulted in significant improvement of RA, with decreasing numbers of patients requiring joint replacement surgery. 7 Clinical trials have shown statistically significant improvement in patient reported outcomes (PROs), such as fatigue and quality of life. 8 Consequently, traditional treatment has focused on the diagnosis and treatment of illness, rather than on incorporating wellness as an essential element of treatment.9,10
The “treat to target” (T2T) paradigm has guided the management of patients with RA over the past 10 years. 11 In RA, T2T goals are usually remission or low disease activity (LDA). T2T requires the selection of measures to assess patient disease activity at regular intervals. Patient and clinician global assessments are usually included (eg, Clinical Disease Activity Index (CDAI), Disease Activity Score (DAS28), Simplified Disease Activity Index (SDAI), and Routine Assessment of Patient Index Data 3 (RAPID3). 12 These measures provide metrics for RA improvement and help clinicians adjust medication therapy (e.g., dose increases, initiation of alternate treatment, etc.).
Discordance between patient and clinician global assessments of disease activity may hinder target fulfillment, leading to frustration among rheumatologists,13,14 and may also involve patients’ tendency to rate their disease progress in light of their own wellness behaviors. Indeed, in a systematic review of patient goals, “wellness” (defined as multidimensional, holistic, and requiring active self-directed engagement) 15 was identified as a major theme among patients with RA. 9 Assessment of wellness factors in measuring RA improvement is thus clearly indicated.
Exercise helps alleviate physical consequences of RA, such as reduced cardiorespiratory fitness, decreased muscle strength, increased weight, and increased pain sensitivity.16,18 Research has shown that mindfulness interventions are effective at reducing stress and markers of inflammation and may even be an effective modifier of inflammation. Numerous studies have shown that healthy sleep is associated with improved health outcomes. Yet, sleep disturbances are common among those with RA, and likely contribute to the commonly reported symptom of fatigue. 19 Social connectedness has been found to be an essential factor in improving adherence to self-management programs for people with RA, as well as improving depression and well-being.20,22 Each of these wellness elements have been studied alone as adjuncts to treating chronic illness such as RA and for patient self-management.
Some clinicians have begun incorporating elements of wellness promotion into treatment with favorable results.9,23 Meanwhile, researchers and clinicians have indicated the need for low-cost, low-maintenance adjunctive approaches to managing RA symptoms.24,25 Perhaps in directly targeting patient wellness, rheumatologists may be more successful in achieving RA therapy targets. The 90-day WILD 5 (Wellness Interventions for Life's Demands) Program and the briefer, 30-day version called “KickStart30” studied in the present investigation, identifies five wellness and anti-inflammatory strategies - exercise, mindfulness, sleep, social connectedness, and nutrition. The full 90-day WILD 5 Wellness Program has shown change in improving psychiatric symptoms in other populations.26,27 The purpose of this formative study was to assess the impacts of an evidence-based, 30-day self-directed, prescriptive wellness intervention (KickStart30) as an adjunct to drug therapy in improving health and wellness among patients with RA.
Methods
Design
The Kickstart30 intervention was evaluated using a single cohort, nonrandomized, pre- versus post- intervention preliminary study design. Program improvements were based on statistically significant improvements on various gold-standard clinical outcome measures related to wellness and functioning from baseline (day 1) to follow-up (day 30), assessed by paired sample t-tests. As this was a formative study, the planned study size was set at approximately 12. We concluded the study with 13 completers. The study was approved by the University of Texas at Austin Institutional Review Board (IRB; Protocol #2018-10-0095), and given its status as an intervention study, was appropriately posted in a clinical trial registry (clinicaltrials.gov) accessible by the public where detailed information regarding the intervention protocol can be found (ID NCT03993548).
Procedures
Participants were recruited between June 2019 and March 2020 using convenience and snowball sampling. Study fliers were posted around a large public university and private clinics across a moderately-sized metropolitan area in central Texas. Electronic fliers were posted on clinicaltrials.gov, RA-focused Facebook groups, subreddits, and blog websites (all with moderator permission). Recruitment was limited to the United States because of prohibitive international shipping costs for the study workbooks. Those interested in participation watched a brief video for an overview of the intervention, then called a dedicated phone number for a screening interview.
Inclusion criteria included a diagnosis of RA from a rheumatologist and current treatment with a TIM (full list of acceptable medications on study flier and full protocol) to ensure participants had at least moderate RA, per immune modulator FDA indications. Additional inclusion criteria were interest in enhancing wellness, fluency in speaking and reading English, age 18 years old or more, having internet access and basic computer skills. Exclusion included individuals who were acutely suicidal or psychotic and/or pregnant or planning on getting pregnant or lactating within the 30-day intervention period. Nineteen individuals were screened for participation: two dropped out after agreeing to participate and four declined.
Participants were assigned a secure ID for online access where they completed online registration and consent and submitted program forms with personal information relevant to create a baseline. The forms and information were securely stored in Qualtrics. After phone screening, participants were mailed a KickStart30 workbook and tracked adherence in Qualtrics. Automated reminders via MailChimp were sent to promote adherence and fidelity to the intevention protocol. Full participation entalied completing HERO exercises and practicing each of the five wellness components every day (for 30 days) as outlined in the workbook (described below).
Exercise
Using the “FID” principles, participants were directed to exercise seven days a week (“Frequency”), at moderate intensity (“Intensity”), for 30 min (“Duration”), and to increase exercise intensity and duration as tolerated. The workbook provided instructions on how to achieve moderate intensity exercise using target heart rate and maximum heart rate calculations. Importantly, a designation in the workbook states that those with physical limitations or a chronic pain condition will have met this requirement if participants exercised “to the best of [their] capabilities,” even if that entailed no exercise on some days. Additionally, participants were encouraged to exercise in line with their health providers’ directives.
Mindfulness
Participants were encouraged to practice mindfulness meditation for at least 10 min daily. Mindfulness meditation, as defined by Jon Kabat-Zinn is “paying attention in a particular way: on purpose, in the present moment, and nonjudgmentally.” 28 To standardize this component, participants were directed to a website (www.wild5meditations.com) where they selected from nine guided meditation recordings (created for this intervention by a researcher – 1) Five-Minute Breathing Space (6:45); 2) Mindful Breathing (15:00); 3) Body Scan (15:00); 4) A Moment of Gratitude (9:58); 5) Happiness Meditation (11:37); 6) Pain Meditation (13:00); 7) Introduction to Mindful Meal Meditation (5:19); 8) Mindful Meal Meditation (23:31); 9) Mindful Moment with a Raisin (9:57)) and downloaded favorites to their preferred device. 26 Participants could use any combination of these recordings throughout the intervention.
Sleep
Participants were asked to implement four or more of six listed sleep hygiene practices each day of the intervention, which included avoiding: electronics at least 90 minutes before bed, daytime naps, ambient light (clocks, windows), caffeine 10 hours before bed; and incorporating relaxing bath or shower before bed, and regular bedtime including on weekends.
Social connectedness
Participants met or called a minimum of two friends or family members daily. The workbook provided education on macro- versus micro-socializations (e.g., having dinner with family or friends vs saying good morning to a passerby) to elucidate different types of social interactions. Participants were encouraged to optimize both levels of socialization and to examine their own social tendencies as they found comfortable and sustainable ways to connect with others. Texting did not meet adherence to this criterion.
Nutrition
To meet the “nutrition” requirement, participants logged their daily intake (meals, snacks, beverages, alcohol) during the intervention, with the expressed goal of enhancing mindful consumption. Although no form of dieting was required, the workbook provided guidelines on how to follow the research-based MIND diet, a diet rich in plant-based foods and limited in animal proteins, which has been shown to have many physical and mental health benefits.
HERO exercises
Participants spent five minutes per day completing brief written exercises meant to enhance four positive psychology wellness traits - Happiness, Enthusiasm, Resilience, and Optimism (HERO). Each daily HERO exercise included two questions related to two wellness traits. For instance, to enhance happiness and enthusiasm, one HERO worksheet included participants writing down two positive things they would like to experience that day (happiness) and two projects they find inspiring (enthusiasm). The objectives of the daily intervention sessions are illustrated in Table 1.
Objectives of Daily Interventions.

Measures
Wolfe and colleagues developed the 10-item
The
The
The
The 5-item
The 15-item
The
The
The
The
The
Data Analysis
Standard descriptive statistics were calculated for demographic and baseline clinical data, and for pre/post intervention scores for all 12 outcome measures. Paired t-tests were used to test differences between means of pretest and posttest measures, and Cohen's d was reported as an effect size. Cohen 42 classifies d effect sizes .20-.49 as small effects; .50-.79 as medium effects; and .80 or higher as large effect sizes. Assumption of distribution normality was assessed with the Shapiro-Wilk Test. With a statistically significant Shapiro-Wilk result, mean differences were tested with Related-Samples Wilcoxon Signed Rank Tests and a matched rank biserial correlation was reported for effect size. All tests were two-sided, with p < .05 significance. Given the formative nature of the study, no adjustments for testing of multiple outcomes were made increasing the likelihood of type 1 error. Descriptive statistics were performed in Microsoft Excel (version 16.39 for Mac), and inferential statistics were performed in JASP version 0.12.2.
Results
Statistical analyses demonstrated significant changes across nearly all outcome measures. Descriptive statistics and test results are displayed in Table 2. Fifteen participants enrolled in the study (completed all pre-program forms), and of those that enrolled, 13 completed the study (completed all post-program forms), resulting in an 87% completion rate.
Pre- and Post-Test Descriptive Statistics and Test Results for Outcome Measures.
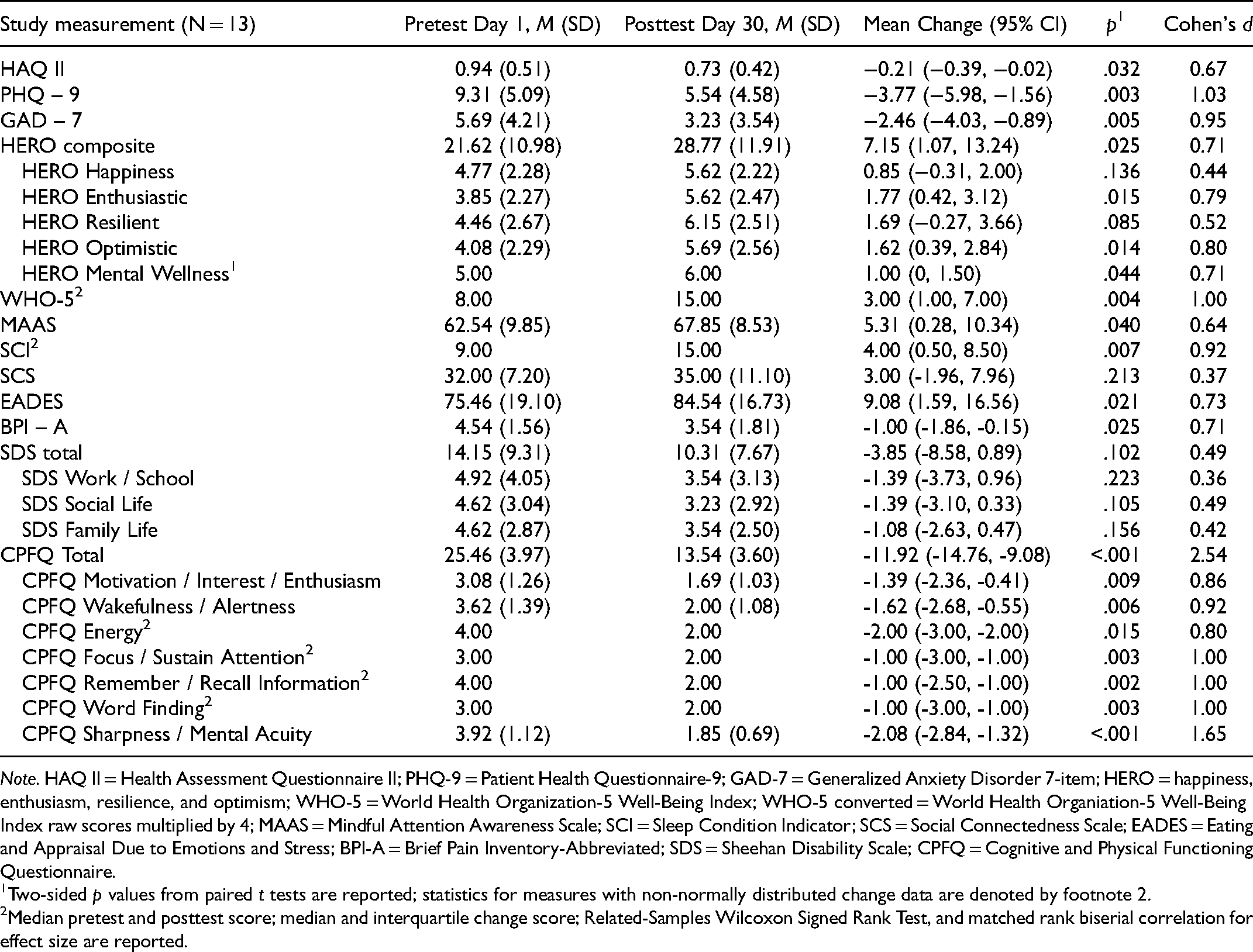
Note. HAQ II = Health Assessment Questionnaire II; PHQ-9 = Patient Health Questionnaire-9; GAD-7 = Generalized Anxiety Disorder 7-item; HERO = happiness, enthusiasm, resilience, and optimism; WHO-5 = World Health Organization-5 Well-Being Index; WHO-5 converted = World Health Organiation-5 Well-Being Index raw scores multiplied by 4; MAAS = Mindful Attention Awareness Scale; SCI = Sleep Condition Indicator; SCS = Social Connectedness Scale; EADES = Eating and Appraisal Due to Emotions and Stress; BPI-A = Brief Pain Inventory-Abbreviated; SDS = Sheehan Disability Scale; CPFQ = Cognitive and Physical Functioning Questionnaire.
Two-sided p values from paired t tests are reported; statistics for measures with non-normally distributed change data are denoted by footnote 2.
Median pretest and posttest score; median and interquartile change score; Related-Samples Wilcoxon Signed Rank Test, and matched rank biserial correlation for effect size are reported.
Mean PHQ-9 scores decreased by 3.77 points, indicating an overall improvement from nearly qualifying as moderate depression, (M = 9.31) to nearly qualifying as minimal depression (M = 5.54). For the PHQ-9, a score of 5—9 indicates mild depression. While both the pre-test and 30-day mean scores indicated mild depression and were not clinically significant, they were statistically significant (p = .003, d = 1.03).
Mean GAD-7 scores decreased by 2.46 points. A score of 5 on the GAD-7 is the threshold for detecting anxiety, thus the mean pre-test score (M = 5.69) improved from mild anxiety to clinically non-meaningful anxiety symptoms at 30 days (M = 3.23) and was statistically significant (p = .005, d = .95).
Mean composite HERO Wellness scores increased by 7.15 points, and the difference was statistically significant (p = .025). Mean scores of each domain also demonstrated improvement, however, only enthusiasm (p = .015), optimism (p = .014), and mental wellness (p = .044) were statistically significant. WHO-5 Well-Being Index 30-day scores were statistically significantly higher than pre-test scores (W = 0.00, p = .004, d = 1.00). Using transformed scores, of the 13 participants, 7 (54%) increased by more than 10 points. Applying the suggested cutoff of less than or equal to 50 for reduced well-being, 10 of 13 (77%) were below the cutoff at baseline. Following treatment, those below the cutoff decreased to 6 (46%), which indicates an overall improvement in emotional and mental well-being.
Mean MAAS scores increased by 5.31 points, indicating that participants experienced increased levels of mindfulness. This finding was statistically significant (p = .040, d = .64) and indicated a moderate effect.
SCI, a measure of insomnia, had one of the largest score increases. A Wilcoxon Test indicated that 30-day scores were statistically significantly higher than pre-test scores, p = .007. This improvement was also clinically significant as the 30-day mean score (M = 17.62) no longer met the insomnia threshold.
Mean SCS scores increased by 3 points, indicating that social connectedness increased in the expected direction, but this change was not statistically significant (p = .213). Mean EADES scores showed improvement in stress-related eating, which is common in people with rheumatological illnesses, and this finding was statistically significant (p = .021, d = .73). Mean BPI-A scores decreased 1 point and were statistically significant (p = .025, d = .71).
Mean total SDS scores decreased by 3.85 points, indicating a reduction in overall functional impairment, but was not statistically significant (p = .102). The three components of the scale, work/school, social life, and family life, all improved after 30-days, but were also not statistically significant.
Mean total CPFQ scores improved 11.92 points at 30-days and was statistically significant (p < .001, d = 2.54). The seven components of the CPFQ demonstrated statistically significant improvement as well. On average, HAQ II scores, another measure of functional status, improved by 0.21 points, and was statistically significant (p = .032, d = .67). Overall, these results demonstrate a highly significant 30-day improvement in cognitive and physical functioning which coincides with the reduction in functional impairment demonstrated with the SDS.
The Post-Program Participant Questionnaire demonstrated a mean 43.85% improvement in overall wellness (range 10% to 100%).
Discussion
RA is a challenging, chronic disease with significant impact on physical and emotional well-being.1,4,6 Although there have been significant advances in this field with the introduction of biologics and JAK inhibitors, some individuals with RA continue to suffer. Better interventions are needed to address both the physical disability, and common mental health disabilities that often accompany this inflammatory disorder. Indeed, the present investigation reveals that participation in a 30-day, self-directed program aimed at enhancing wellness (KickStart30), as an adjunct to pharmacologic therapy, may lead to further improvements in RA specific disability, mood, anxiety, sleep, and cognitive and self-reported physical functioning
The aim of this formative study was to test KickStart30 in its ability to address issues of disability, suffering, and impairment by adding it to current treatment regimens. Treatment of RA has traditionally targeted joint pain and inflammation. Almost all metrics of disease activity include a patient global assessment, which contributes to frustrating discordance between clinician and patient views of improvement and meeting of treatment targets.13,14
It may be possible to strengthen the agreement in the ratings between patient and clinician of disease activity and remission, by enhancing wellness factors directly. Patients with RA often include individual reports of wellness behaviors in self-assessments and enhancing these wellness factors may have a favorable impact on global assessments. 9
To the best of our knowledge, this is the first study of a multipronged wellness intervention in patients with RA. Our findings support those of the individual health promotion interventions utilizing sleep, 43 exercise, 17 nutrition,16,44 social connection,21,22 and mindfulness.45,46 Additionally, our findings validate the positive impact of these measures in a combined self-management intervention. The positive results are encouraging, particularly in light of the robust improvements that were realized in a short period of time (30 days) with minimal hands-on management by the clinical team. These are important considerations given rheumatology is a highly specialized field with a limited number of providers who are often overstretched in their provision of high-quality care. We hope that this research inspires investigators from different global institutions to consider similar interventions for their RA patients. Clearly, improving the lives of people with RA from a holistic, mind-body perspective is an urgent clinical need. While this formative study did produce positive results, the final determination of the value of wellness interventions in improving the lives of patients with RA will only be answered by more definitive RCT studies.
There are a number of limitations to this study and so generalizability of the present findings should be considered with caution. First, this is an open label, small pilot study (N = 13) that did not include a control group. We find it encouraging that the predominantly female sample represents RA population prevalence statistics, although a lack of control group is inherently problematic with respect to inferring causality. Second, sample self-selection bias and the intervention's requirement for English literacy and internet/computer access among participants should be considered. Third, RA diagnoses were self-reported and not confirmed by a rheumatologist. However, the inclusion criterion requiring that participants were already taking a RA-specific prescription helped to ensure that all participants had true moderate to severe diagnoses, since such medications are not indicated for milder forms of RA. Fourth, all measurements were prone to self-report biases, although we justified their use in order to expand our small pool of eligible participants by not requiring expensive and clinician-obtained objective measures of RA disease activity (eg, RAPID3, CDAI, or DAS28) and laboratory measures of inflammation (e.g., ESR or CRP). Moreover, to reduce social desirability bias inherent in self-report methods, participants were not given access to their measurements or scores after submission. Also, our modified use of the BPI indicates that overall scale reliability and validity may not apply to our use of a smaller subset of items. Lastly, given the formative nature of the study, no adjustments for testing of multiple outcomes were made increasing the likelihood of type 1 error.
Conclusion
The purpose of this study was to evaluate a holistic self-management wellness intervention in a population with limited research in this area. Given numerous scales were used to measure disability, mental health, and wellness—and that the vast majority indicated statistically significant improvements in the expected direction—supporting the progression to larger trials using the addition of a wellness intervention, such as KickStart30, could have an important role in improving disability and mental wellness, and reducing mental health suffering. From the perspective of busy clinicians with limited time to coach patients in wellness, KickStart30 may be a particularly attractive intervention given positive results were realized in a brief time frame with minimal clinical oversight. In sum, The WILD 5 Wellness Kickstart30 program is an intervention that is easily implemented, inexpensive, and demonstrated significant effects in 13 participants with moderate to severe RA. We encourage larger and better controlled studies of wellness interventions, as reducing human suffering and enhancing wellness and self-empowerment are worthy goals of every clinician. 45–47
Footnotes
Author Contributions
Tara Hutson and Nicole Murman wrote the initial draft of the manuscript with support from Donna Rolin, Saundra Jain, and Andrew Laster. Tara Hutson performed the initial data analyses and compiled the tables. Nicole Murman created the histograms. Steve Cole reviewed and revised the statistical analyses, tables, and histograms. Rakesh and Saundra Jain developed the research project and collected the data. All authors revised the manuscript for final submission.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Rakesh Jain - Co-creator of WILD5 Wellness Program – All profits are donated to mental health charitiesAndrew J. Laster - Consultants: Eli Lilly; Amgen; Myriad; Speaker bureau: Amgen; Eli Lilly; Pfizer; Novartis; Genentech; Exagen; MyriadSaundra Jain - Co-creator of WILD5 Wellness Program – All profits are donated to mental health charities; has served as a consultant, member of advisory boards, and/or speaker bureaus for Eli Lilly, Otsuka, Pamlab and Sunovion
Ethical Approval
Approval from IRB.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sigma Theta Tau International Epsilon Theta Chapter, research grant received by Dr. Donna Rolin.