
Abstract
In the United States, approximately 21% of the adults suffer from arthritis. Yoga offers one possible way of managing arthritis. The purpose of this study was to look at studies from 2010 to June 2013 and examine whether yoga can be an efficacious approach for managing arthritis. A systematic search from Medline, Cumulative Index to Nursing and Allied Health, and Alt HealthWatch databases was conducted for quantitative articles involving all schools of yoga. A total of 9 articles met the inclusion criteria. Five of these were from the United States and 4 from India. Of the 9 studies, 6 demonstrated positive changes in psychological or physiological outcomes related to arthritis. Despite the limitations not all studies using randomized controlled design, having smaller sample sizes, having different outcomes, having nonstandardized yoga intervention, not using behavioral theory, and having varying lengths, yoga appears to be a promising modality for arthritis.
Introduction
In the United States, more than 21% of the adults or approximately 46.4 million people have self-reported doctor-diagnosed arthritis. 1 According to the National Arthritis Data Workgroup, of those suffering from arthritis, approximately 27 million have clinical osteoarthritis, 2 4 to 10 million have carpal tunnel syndrome, 2 5 million have fibromyalgia, 2 3 million have gout, 2 1.3 million have rheumatoid arthritis, 1 0.6 to 2.4 million have spondylarthritides, 1 0.4 to 3.1 million have primary Sjögren’s syndrome, 1 294 000 children have juvenile arthritis, 1 161 000 to 322 000 have systemic lupus erythematosus, 1 and 49 000 have systemic sclerosis. 1 In addition to these types of arthritis, 59 million reported low back pain in the past 3 months, and 30.1 million reported neck pain in the past 3 months. 2 It is projected that 67 million (25%) adults aged 18 years or older will have doctor-diagnosed arthritis by the year 2030. Of those with arthritis an estimated 25 million (37%) will have arthritis-attributable activity limitations. 3 Furthermore, the total costs attributable to arthritis and rheumatic conditions in the United States based on a study in 2003 was approximately $128 billion, which equaled 1.2% of the US gross domestic product at that time. 4 Based on these data it can be easily said that arthritis is a common and significant public health problem.
The Centers for Disease Control and Prevention has recommended 3 major modalities for management of arthritis patients: (a) medication; (b) nonpharmacological approaches such as self-management, physical or occupational therapy, weight loss, joint assistive aids; and (c) surgery. 5 The role of self-management and increasing physical activity is of paramount importance in management of arthritis. It is in this context that yoga has been applied and tested for arthritis. By stretching of the muscles yoga can provide physical relief of symptoms around the affected joints. Yoga reduces stress, which is known to exacerbate arthritis. Yoga can improve coping and by altering perspective toward life and provide spiritual solace.
The word “yoga” is derived from the Sanskrit word meaning “union.” It is an ancient system of physical and psychic practice that originated during the Indus Valley civilization in South Asia. The first written records of this methodology appeared around 200
The traditional practice of yoga was quite rigorous, arduous, and entailed lifelong devoted practice and adherence to strict austerities. Today, many schools of yoga have simplified the techniques making these more suitable for users in different walks of life. The 8 conventional steps of Asthangayoga consist of Yama (rules for living in society), Niyama (self-restraining rules), Asana (low physical impact postures), Pranayama (breathing techniques), Pratihara (detachment of the mind from senses), Dharana (concentration), Dhyana (meditation), and Samadhi (complete union with super consciousness). 9 Today, various schools of yoga use one or more of these techniques.
A literature review was published in 2011 that looked at all the clinical trials from 1980 to 2010 that had studied the effects of yoga on arthritis. 10 The study summarized the results from 11 such trials and found that sample sizes were small and not all studies used control groups. The results showed reduced disease symptoms (tender/swollen joints, pain), decreased disability, improved self-efficacy and better mental health. Since 2010, several additional studies have been published in this area. Hence, the purpose of this review was to look at these additional studies and examine whether yoga can be an alternative and complementary approach for arthritis.
Questions being addressed in this review include the following: Has yoga been found to be efficacious in alleviating symptoms of arthritis since the 2011 review? Are there sufficient data available to draw conclusions regarding the efficacy of yoga in arthritis? What are the methodological limitations of present research studies and how can these be addressed in future research? What are the common outcome measures measured by studies and which ones are more important for future studies?
Methods
A systematic review of studies involving yoga interventions for arthritis was the method used in this study. To be included in this study the article must meet the following criteria: (a) be published in the English language; (b) be included in the Medline, Cumulative Index to Nursing and Allied Health, or Alt HealthWatch database; (c) conducted between the years January 2010 and June 2013; (d) include any form or school of yoga as an intervention; (e) use any quantitative study design for evaluation; and (f) measure at least one of the following psychological or physiological outcomes—pain, disability, swelling, morning stiffness, physical function, depression, anxiety, quality of life, sleep, C-reactive protein, and hand grip strength. Articles were excluded from this review if they did not satisfy the following criteria: (a) studies that did not evaluate the intervention or implemented a qualitative design; (b) did not include selected outcome measures; and (c) did not index in Medline, Cumulative Index to Nursing and Allied Health, or Alt HealthWatch database.
Three phases of data review were conducted for this study (Figure 1). To identify studies meeting these criteria Medline, Alt HealthWatch, and Cumulative Index to Nursing and Allied Health database searches were performed for phase I. Boolean terms used to identify studies meeting the criteria included, “Yoga AND Arthritis” for the time period January 2010 to June 2013.

Flowchart depicting the 3-step data extraction process.
Using the above terms/phrases, 47 articles were returned—from Medline (n = 23), Alt HealthWatch (n = 8), and Cumulative Index to Nursing and Allied Health (n = 16). Phase II included preliminary distillation of the articles by eliminating duplicates (n = 4), review/discussion/other articles (n = 29), and studies not incorporating quantitative designs (n = 2). In Phase III, comprising of manuscript review of the remaining articles (n = 12), 2 studies did not have results and 1 study did not incorporate at least one of the selected outcome measures and had cost as outcome variable, which was not selected. Hence, the remaining articles (n = 9) satisfied the eligibility criteria.
Results
As a result of the data extraction process, 9 articles were found to satisfy the eligibility criteria. Table 1 summarizes the studies, including the year of publication, authors/country where the study was performed, study design and sample size, age of participants, intervention modality, intervention dosage, outcome measures, and the salient findings. The studies are arranged by year of publication in the ascending order starting from 2010. Within a given year, studies are arranged alphabetically by the last name of the first author.
Summary of Yoga Interventions for Arthritis Done Between 2010 and June 2013 (n = 9).
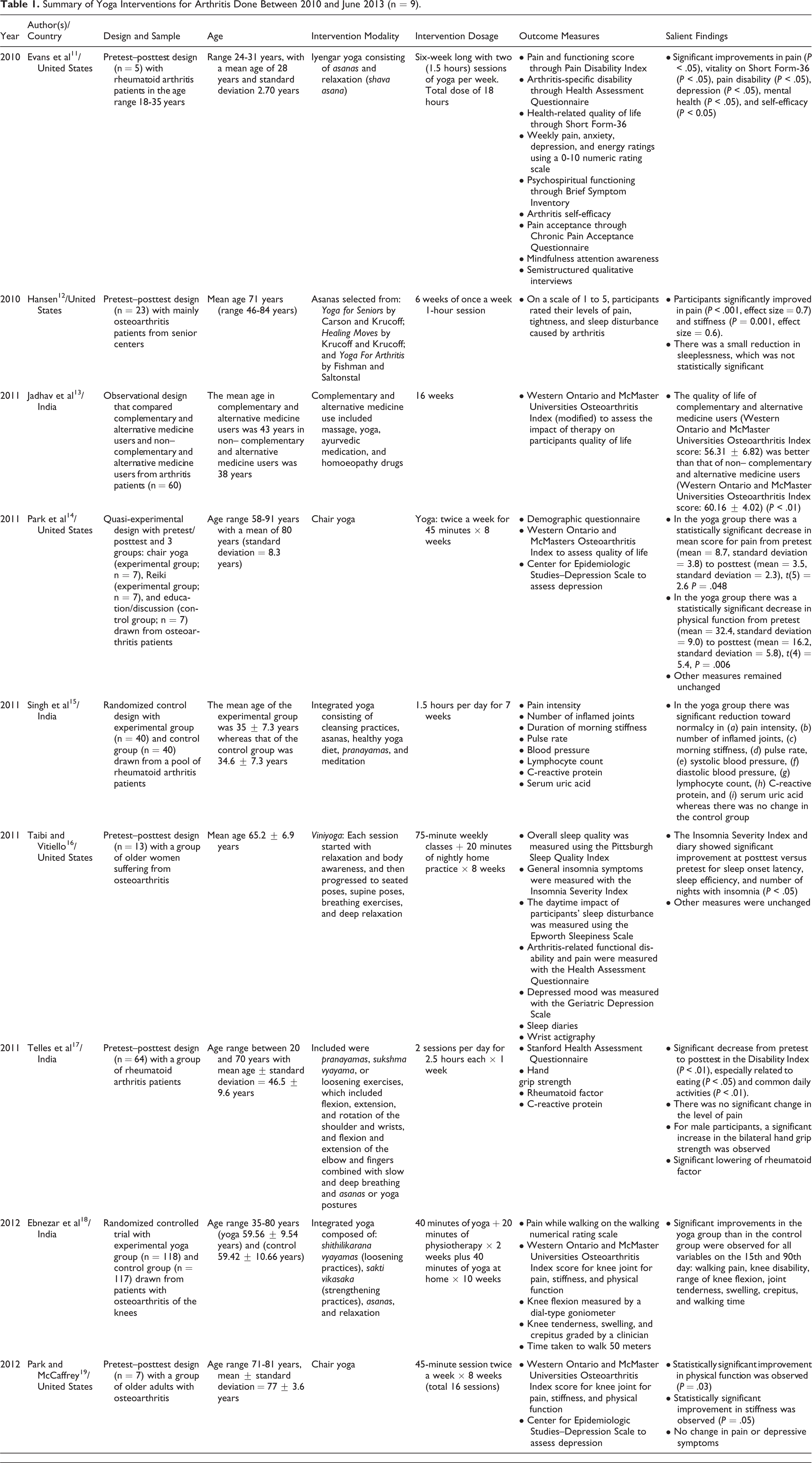
Of the 9 interventions 5 were done in the United States 11,12,14,16,19 and 4 in India. 13,15,17,18 Of the 9 interventions, 2 used randomized controlled designs, 15,18 1 used quasi-experi-mental design, 14 5 used pretest–posttest designs, 11,12,16,17,19 and 1 was an observational study between complementary and alternative medicine users and non–complementary and alternative medicine users for arthritis. 13 The mean sample size calculated for all 17 studies in this review was 56.44 with a standard deviation of 72.33 and range of 5 to 235. Total sample sizes (n) were typically less than 30 with 5 studies 11,12,14,16,19 falling in this group and only 1 study had the sample size more than 100. 18 The sites of the yoga intervention for arthritis were in colleges/universities (n = 3), 14,16,19 hospitals/outpatient clinics (n = 3), 13,15,18 community settings (n = 2), 11,12 and at a residential yoga camp. 17 The school of yoga was not identified by 2 studies. 12,13 It was identified as chair yoga by 2 studies, 14,19 integrated yoga by 2 studies, 15,18 Iyengar yoga by 1 study, 11 viniyoga by one study, 16 and hatha yoga by 1 study. 17
The duration of yoga interventions varied from 6 hours 12 to 46 hours. 18 The mode of duration was 12 hours (n = 3) 14,16,19 and mean was 18.6 hours (standard deviation = 13.14 hours). The most common outcome measure was the score on Western Ontario and McMaster Universities Osteoarthritis Index for pain, stiffness, and physical function, which was used by 4 studies. 13,14,18,19 Several other studies had also measured pain and functioning using other scales. 11,12,15,16,17 Two studies 15,17 used a physiological measure of C-reactive protein. Two studies 12,16 focused on sleep aspects of arthritis and 3 studies 14,16,19 focused on depression associated with arthritis.
Discussion
The aim of this review was to examine studies published from 2010 to June 2013 and examine whether yoga can be an alternative and complementary therapeutic approach for managing arthritis. A total of 9 studies met the inclusion criteria. The first question that this review addressed was—“Has yoga been found to be efficacious in alleviating symptoms of arthritis since the 2011 review?” From the 9 studies, a majority (n = 6) 11–15,18 demonstrated positive changes in psychological or physiological outcome measures related to arthritis. The other 3 remaining studies 16,17,19 had mixed results where some of the indicators showed improvement whereas the other measures did not change. These findings are in consonance with the previous review published in 2011 that found majority of studies having positive results on symptoms of disease (pain, tenderness, stiffness) and disability. 10 Of the 6 studies that showed positive results, only 2 had used randomized controlled designs. 15,18 This type of design is considered the most rigorous as it enlists pretests and posttests, randomizes the participants or their group into a control and an experimental group, and minimizes threats to internal and external validity. In this design, changes in pretest and posttest scores can be contrasted by levels of intervention. This can be seen in the randomized control trial from India 15 that had 2 groups: (a) an experimental yoga group that received 1.5-hour sessions per day for 7 weeks and (b) a control group. The findings showed in the yoga group there was significant reduction toward normalcy in (a) pain intensity, (b) number of inflamed joints, (c) morning stiffness, (d) pulse rate, (e) systolic blood pressure, (f) diastolic blood pressure, (g) lymphocyte count, (h) C-reactive protein, and (i) serum uric acid, whereas there was no change in the control group. Likewise in the other randomized controlled trial from India, 18 significant improvements in the yoga group compared with the control group were observed for all variables on the 15th and 90th day, namely walking pain, knee disability, range of knee flexion, joint tenderness, swelling, crepitus, and walking time.
The other design is the pretest–posttest design. Pretest–posttest design is the least costly and simplest but is unable to minimize threats to internal validity such as maturation and history without a control group for comparison. In this review, majority of the studies used this design and found positive changes in arthritis-related outcomes. But without having a control group, the findings can only be interpreted with caution. With regard to design, future studies should use the robust randomized control design or if that is not feasible, the group randomized control design must be used.
The second and third questions that this review examined were as follows: “Are there sufficient data available to draw conclusions regarding the efficacy of yoga in arthritis?” “What are the methodological limitations of present research studies and how can these be addressed in future research?” The review looked at 9 studies, of which only 2 were randomized controlled designs. Based on these studies, some conclusions can be drawn but one would need to consider the limitations. Besides the design, the other shortcomings that need to be kept in mind while interpreting the efficacy of yoga in arthritis are the small sample sizes used in the studies, the lack of standardization of the yoga interventions, and varying dosages of the interventions. The sample sizes have generally been small with only 1 study having sample size more than 100. Two studies used very small sample sizes, for example, five 11 and seven 19 and were excluded. Power calculations and sample size justifications are generally missing from most of the reviewed studies. There have been no multicentric studies or large-scale studies that have been done with this research problem. Future research should look at the possibility of conducting large-scale studies. The yoga interventions have been from a variety of schools of yoga and substantial number do not even identify any particular school. It is essential to identify at least a few asanas, a few breathing techniques, relaxation pose (shava asana), and meditation that are common to all yoga interventions. Although most interventions did mention use of these techniques, it will be important for future research to develop a checklist of essential techniques that can be replicated. There has been a wide variability of intervention time that has ranged from 6 to 46 hours. The mode has been 12 hours with a mean of 18.6 hours. Twelve- to 18-hour interventions seem to be ideal in view of both feasibility and practicality. These interventions are able to make changes in the short term. Long-term sustainability of effect is questionable in this short approach. One intervention 18 taught yoga for 2 weeks and then required participants to practice daily for 10 weeks. This intervention also resulted in significant improvements. Such an approach can be quite promising and needs further replication. Future research should aim at developing interventions that are long range and require home practice by participants.
Another aspect pertaining to methodology of yoga interventions is that none of the interventions used any behavioral theory in the design and conduct of the intervention. Use of behavioral theory such as social cognitive theory or theory of planned behavior helps in discerning measurable program outcomes. This method specifically helps in identifying the timing of the intervention, helps in choosing the right mix of strategies, improves replication, and fosters program efficiency and effectiveness. 20
The final question that this review aimed at answering was—“What are the common outcome measures measured by studies and which ones are more important for future studies?” Both psychological and physiological measures were used by the studies. Both self-report and objective assessments were used by the studies. The most common outcome measure was score on Western Ontario and McMaster Universities Osteoarthritis Index for pain, stiffness, and physical function. Several other studies have also measured pain and functioning using other scales. The symptoms of arthritis, namely pain, stiffness, movement, and functionality around the joint are important markers that must be monitored by all research studies in this area. Some physiological measures that can be used by future studies are C-reactive protein, rheumatoid factor (in seropositive rheumatoid arthritis cases), lymphocyte count, and serum uric acid (in gout). Sleep and depression scales can also be used in conjunction with arthritis measures.
Conclusion
Arthritis is a major public health problem and one of the approaches to address this problem is through yoga. A total of 9 interventions from 2000 to June 2013 examined yoga and its efficacy in alleviating symptoms of arthritis. Of these 9 interventions, 6 were able to demonstrate positive effects in psychological or physiological outcome measures related to arthritis. Despite the limitations of not all studies using randomized controlled design, having smaller sample sizes, having different outcome measures, having nonstandardized yoga intervention, not using behavioral theory, and having varying lengths of intervention, yoga is a promising modality for arthritis. Future researchers must conduct large-scale and long-term yoga interventions to study the effects of yoga on arthritis.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, or publication of this article.
Ethical Approval
This study did not warrant institutional review board review as no human subjects were involved.