
Abstract
Multiple sclerosis (MS) is a chronic autoimmune disease that affects the central nervous system causing neurological deterioration over time. The objective of this study was to examine the predictors associated with MS medication use. The categories that were investigated were various alternative treatments such as complementary/alternative medications (CAMs), rehabilitation therapy and psychotherapy services as well as comorbid health conditions. The Survey on Living with Neurological Conditions in Canada (SLNCC) 2011-2012 was used (N = 73 347) to carry out a logistic regression model. Individuals who did not take CAMs were more (OR = 5.44, 95% CI 1.37-9.29) likely to use medications for MS. Having a mood disorder was associated with greater use of MS medications (OR = 5.39, 95% CI 1.60-18.17) while back problems were associated with lower odds of medication use (OR = 0.38, 95% CI 0.15-0.98). These factors need to be taken into consideration when creating effective medication adherence interventions.
Keywords
Multiple sclerosis (MS) is a demyelinating diseases of the central nervous system and affects individuals between 20 and 45 years of age. 1,2 Although there is no cure for the disease, there are a wide range of disease-modifying treatments (DMTs) that have been effective in shortening the duration and frequency of attacks, providing symptomatic relief and lowering the number of emergency department visits. 3,4 Despite the numerous benefits associated with DMT use, adherence rates among MS patients ranged from 41% to 88%. 5 One of the most common reasons behind low adherence rates among patients is due to the side effects associated with DMT medications such as diarrhea, nausea, flu, sinus infections, rash, and dizziness. 6,7 Other studies indicate that psychiatric disorders such as depression and anxiety are common among individuals with MS and that medication adherence may be hindered due to these illnesses. 8 –10
Currently, effective interventions to improve DMT adherence is lacking. Although there may be many psychosocial factors associated with nonadherence to medications, there have been few studies that examined whether using complementary/alternative medicines (CAMs) affect MS medication adherence. In order to create effective interventions, all factors need to be explored including alternative medication use and the impact on MS medication adherence. The main objective of this study was to examine the predictors associated with MS medication use. Two categories were examined in this study: CAMs and existing comorbid health conditions.
Methods
The Survey on Living with Neurological Conditions (SLNCC) 2011-2012 is a nationally representative cross-sectional survey which collects information on a set of 18 neurological conditions. 11 This survey is linked to the Canadian Community Health Survey (CCHS 2010-2011). The CCHS collects information that is related to the health status, health care utilization and health determinants for the Canadian population. 12 The sample for the SLNCC survey was drawn from the CCHS respondents and household members who were aged 15 years and older who had at least one of the 18 neurological conditions. 12 Data were collected from May 9, 2011 to March 31,2012. 12 Replicate sampling weights and bootstrapped variance estimation were used as recommended by Statistics Canada. 12 A set of (n = 500) replicate weights were used which accounted for nonresponses. For the SLNCC linked data set, the bootstrap replicates are the sub samples that were drawn and used to estimate the variance of the CCHS estimates. 12
Measures
All variables were based on self-reported measurements. The main outcome variable was whether the MS patient used medications. The response for this variable was either “1 = yes” or “0 = no.” Demographic factors such as age, sex, income, and education were assessed. Age was categorized as 22 to 30, 31 to 40, 41 to 50, and >51 years. Income was categorized as 5000 to 39 999, 40 000 to 59 999, 60 000 to 89 999, and ≥90 000 Canadian dollars. Education was categorized as less than secondary school education, secondary school or greater, and some post-secondary school or greater.
The first type of category that was assessed was the type of treatments such as complementary/alternative medical treatments (injections, infusions, or pills), rehabilitation therapy and counseling/psychotherapy services. Mood disorder was examined as the psychological factor in the model. Individuals were asked whether they had mood disorder such as depression, bipolar disorder, mania, or dysthymia and the answers for these were either “yes” or “no.” The second category that was examined were chronic comorbid health conditions such as back problems (excluding scoliosis, fibromyalgia, and arthritis), arthritis, heart disease and blood pressure and the responses were either “yes” or “no.” The age of first diagnosis of MS was also used in the screening process and was categorized as ≤ 30, 31 to 40, 41 to 50, and >51 years.
Analysis
A logistic regression model was used to determine whether each of the predictors were associated with medication use. These predictors were selected based on previous theories on this topic. Unadjusted and adjusted odds ratios (ORs) with 95% CIs with P values were computed. Univariate analysis was conducted using a (P < .20). Manual backward selection was used to build the multivariate model based on (P < .05). A complete case analysis was conducted in which only variables with complete values were used in the model and missing values were removed. Confounders were tested in the final model and were retained if the addition of that variable changed the coefficients of the other variables by more than 20%. Interactions were assessed and added to the model if they were significant at (P < .05). The goodness-of-fit statistics was used to assess model fit. The analysis was performed using STATA IC 15.
Results
The final sample consisted of 73 347 weighted observations. There were 49 770 individuals who used medication to treat MS and 23 577 individuals who did not use medications. The sample consisted of 75% of individuals who were females and 25% who were males. Based on the weighted percentage, 50% of individuals with MS were those who were 51 years of age and older, 33% were those who were 41 to 50 years of age, 12% were those 31 to 40 years of age, and 5% were 22 to 30 years of age. In terms of education majority of respondents had some postsecondary education or greater; however, education was not significant and did not have an impact on whether a person used MS medications. Age and sex were controlled in the final model. Although counseling/psychotherapy services and rehabilitation were not significant in the univariate analysis, they were tested for in the final multivariate analysis based on P < .05.
Based on the univariate analysis (Table 1), income, CAM use, back problems, and mood disorder were significant and were included in the final multivariate model. Table 2 shows the results of the multivariate analysis and Table 3 shows the comparisons of the results for the significant variables. Individuals who did not take CAMs were more likely to take medications for MS as opposed to those who used CAMS (OR = 5.44, 95% CI 1.37-9.29). Individuals with a mood disorder were more likely to take MS medications as opposed to those who did not have a mood disorder (OR = 5.49, 95% CI 1.18-25.7). Individuals with MS who had back problems were less likely to take MS medications than those who did not have back problems (OR = 0.32, 95% CI 0.11-0.95). The goodness-of-fit statistics which showed whether the observed and expected observations for the final model were a good fit was 0.23 indicating a good model fit.
Univariate Analysis for Predictors Associated With Medication Usage.a

a Numbers were rounded either up or down due to weights and bootstrapping procedures.
* Shows significance at P < .20.
Multivariate Analysis of Predictors Associated With Medication Usage.
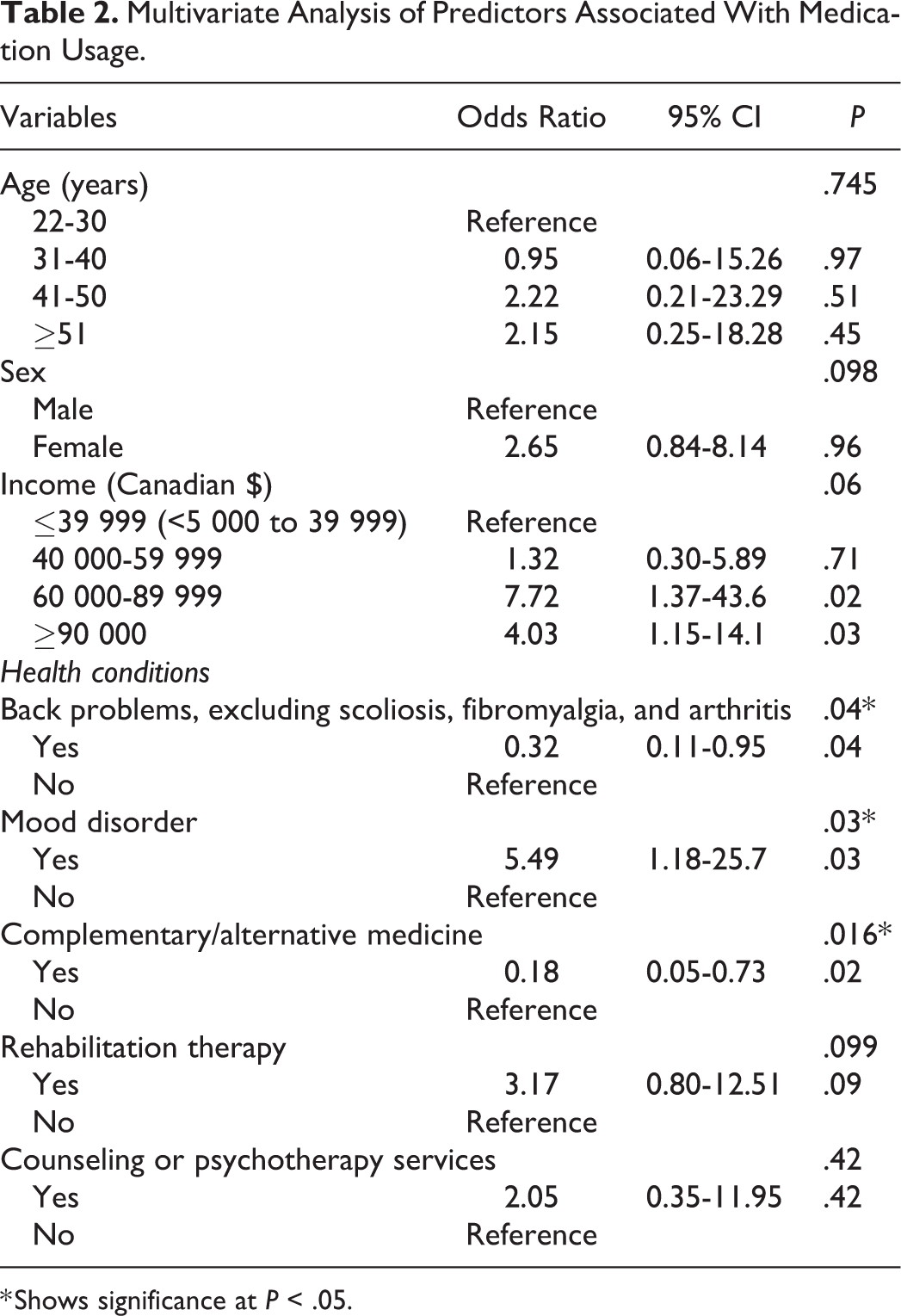
* Shows significance at P < .05.
Comparisons of Odds Ratios Based on Significant Variables From the Multivariate Analysis.

Discussion
This study aimed to show the predictors that were associated with medication use for MS among patients in Canada. Our study indicated that sociodemographic factors were not associated with medication use. These findings are in agreement with a similar study that showed sociodemographic differences as not being a factor in using complementary medication use versus MS medication use among individuals diagnosed with MS. 13 From the analysis it was evident that using CAMs were associated with lower medication use. A study which examined the frequency and characteristics of CAM use among patients with MS found that 67.3% of patients were currently using one or more CAMs. 13 The patients who used complementary treatments were more severely affected by MS than non-users and had a greater duration of the illness. Studies have reported that the most common reason for using CAMs was the desire by MS patients to use holistic health care which treated the mind, body, and spirit. 3 The most frequent CAMs used were herbs followed by massages and acupuncture. 14 Similar studies have reported use of vitamins, essential fatty acids, and minerals. 15 CAMs are used frequently by patients with MS because they experience improvements in their symptoms. 16 Randomized controlled studies indicate that complementary treatments are not very effective in providing symptomatic relief for people living with MS while others indicate positive results. In a study on the effectiveness of American ginseng on fatigue for people living with MS, it was reported that there were no significant difference in fatigue among individuals who were in the experimental group vs the placebo group. 17 In another randomized controlled trial on the effect of ginkgo biloba on functional measures in MS found that individuals in the ginkgo group had shown improvements on measures associated with fatigue, symptom severity, and functionality. 18 Discrepancies in outcomes between various types of complementary treatments could account for why some patients may decide to stop taking medications while others may take supplements along with their MS medications. Our findings were similar to other studies where CAM use was significantly increased when patients did not use MS medications. 19 In some cases, patients decided to use complementary medicine instead of using conventional treatments because of the side effects associated with medications and they believe that more focus should be on getting rid of the stress which will help them feel better over the years. 16 Other reasons for using CAM was the dissatisfaction with medical treatments with regard to lack of support from health care professionals and having less control of medications being prescribed. 20
Our findings also indicated that mood disorders and back problems were associated with whether a person who had MS were likely to take medications. Mood disorders consisted of major depressive disorder, dysthymic disorder, bipolar disorder, panic disorder, and generalized anxiety disorder. 21 The results of our study indicate that individuals with mood disorder were at a greater odds of medication use. This is consistent with the study where researchers examined the effect of comorbidities on DMT use among patients with MS where they found that patients with depression were 13% more likely to initiate DMTs compared to those who did not have depression. 22 One of the reasons for this could be that individuals with depression may have had more active MS as opposed to those who did not have depression and this could be a reason for initiating DMT treatment. 23 Another study also reported that the main reason for alternative treatment use was to gain relief from physical and psychological symptoms. 24
Depression has also been correlated with fatigue caused by MS. 25,26 The lifetime prevalence of depression in MS patients is 50%. 27 Fatigue is a problem that has been overlooked over the years but new studies indicate that 50% to 90% of patients report fatigue as one of the symptoms of MS. 28 Since fatigue is a common problem, physicians prescribe modafinil to patients, which helps with wakefulness and reduces fatigue. 25 This could be one of the reasons for the increase use of MS medications among individuals who have mood disorder since modafinil could be one of the prescribed medications along with first line medications for MS. Patients who have both MS and mood disorder may be more inclined to take their medication in order to reduce their fatigue which they may believe is the cause of their mood disorder. It has also been suggested that psychiatric episodes occur before MS onset, which is a possible explanation for why it may seem that patients who have mood disorder are more likely to use MS medications. 29 Further clinical studies on psychiatric problems among MS patients need to be carried out in order to understand this association.
Back problems are a common problem in patients with MS due to painful spasms. In order to reduce painful spasms caused by MS, patients turn to massage therapy or acupuncture. Our study indicated that those with back problems had a lower adherence to MS medication than those without back pain. One of the reasons for this is that DMTs for MS do not target pain, therefore patients turn to CAM in order to help relieve the symptoms. In a study done on factors associated with CAM use found that CAM helped patients relax, reduce tension and pain in addition to improving overall quality of life. 30 Another study indicated that pain is managed poorly in the treatment course of MS and many patients have turned to opioid medications, benzodiazepines, massage therapy, marijuana and hypnosis treatments because of this problem. 31 Therefore having symptoms that are associated with MS could be the reason why patients turn to CAM use instead of sticking to their daily regimen of medications.
Medication adherence is important and in order to create effective interventions for individuals who have problems with adhering to medications, behavioral modification models could be incorporated as an intervention in patient education programs. There are a vast number of social behavioral models that have been found to be effective in helping patients adhere to medications for many illnesses. 32 For example, the health belief model is commonly used to change one’s behavior with regard to compliance to medications. 33 It is dependent on whether the patient thinks that they are at risk for an illness, whether they think the health condition has consequences, whether there is a course of action for the illness, and whether the benefits of taking action outweigh the costs. 33 One of the problems with adhering to medication is that when many medications are prescribed, the patient may find it difficult to manage. Behavioral models for medication adherence could be effective if the model is modified. The effectives is not based on the model that one chooses, but is based on tailoring the model to suit the individuals needs based on the type of illness they have, operationalize the factors such that the factors that motivate the person are identified and then to use the model based on these changes. 32 In a study done by Klauer et al 34 on compliance, adherence and the treatment of MS, researchers state that a comprehensive model of treatment adherence should integrate patient, therapist, illness, treatments factors as well as the external factors from the social environment. Therefore, interventions need to be tailored to the specific deficits of the patient. The main goal for interventions is to encourage the patient to take responsibility for their treatment. 34 Having good communication between the patient and health care providers is important for better treatment progress.
The limitation of this study is that it is a cross-sectional study, therefore a cause and effect relationship cannot be determined. The disease course and severity of MS was not available in the survey, which would have been beneficial for determining whether medication and CAM use differed based on the stage of illness of the respondent. The specific type or category of medications used as well as frequency of these medications was not available and could have been a potential confounder in this analysis. This information would have helped in understanding why some patients may have stopped taking MS medications and would have allowed for a detailed analysis. Another potential confounder that was not available was the specific type of CAM used, which would have been beneficial in the analysis since it would have provided clues as to why patients were using a particular type of CAM compared with others. The study highlights the importance of good communication between health care providers and patients and the need for better interventions for MS medication uptake.
Conclusions
This is one of the few studies that have examined the association between various alternative treatment options and their impact on mediation use among MS patients. In order to create effective interventions for medication uptake, patient education programs need to cover areas such as importance of taking MS medications, the side effects of using CAMs and incorporate models of behavior change. Future clinical research in mental health and CAM use is needed so that more insight into risk factors for MS medication non-adherence can be understood.
Footnotes
Acknowledgments
The authors acknowledge and thank the Saskatchewan Research Data Centre for providing access to conduct the analysis presented in this research. Opinions expressed in this publication are those of the authors and do not reflect the opinions or views of Statistics Canada.
Author Contributions
KBA was involved in conceiving and designing the study along with analyzing and interpreting the data. CD provided review, feedback, and revisions of the manuscript. Both authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KBA received funding from the Canadian Research Data Centre Network (CRDCN) Emerging Scholars Grant during her PhD studies.