
Abstract
The authors investigated the prevalence of complementary and alternative medicine usage among medical students and assessed their knowledge and attitude. A survey was conducted, and the following results were obtained: the response rate was 91% (408/450), 61% were female and 67% were 22 years old or younger, 66% had used complementary and alternative medicine, and 17% were using complementary and alternative medicine currently. Most commonly mentioned complementary and alternative medicine include echinacea, cod liver oil, and aloevera. More than half were not sure about complementary and alternative medicine’s efficacy and safety, but 88% would recommend it to others. Only 16% had informed their general practitioner about complementary and alternative medicine use. With respect to formal teaching on complementary and alternative medicine, 56% of the students had not received any and 28% expressed an interest in receiving some. complementary and alternative medicine use among medical students is common despite most being unaware of potential side effects and drug–herb interactions. Such information is vital in enabling them to counsel future patients. Education on complementary and alternative medicine should be standardized and compulsory in all UK medical schools.
Introduction
Complementary and alternative medicine is becoming increasingly popular in the United Kingdom and Europe. In the United States, studies have shown that approximately 38% of adults and approximately 12% of children are using some form of complementary and alternative medicine. 1 It is estimated that in the United Kingdom an estimated £1.6 billion is spent annually on complementary and alternative medicine, 2 but it remains difficult to say precisely how many people use it regularly, due in part to its broad definition that encompasses an array of remedies, most of which are unregulated and readily available over the counter. It can be defined as a health-related therapy or discipline that is considered to be part of mainstream medical care, and as its use continues to grow, it now represents a significant sector within the health care industry, mainly due to an increase in patient demand and in the number and diversity of providers that now exists. 3
In 1999, there were approximately 50 000 complementary and alternative medicine practitioners registered in the United Kingdom, 10 000 of whom are registered health care professionals. 4 It is therefore vital that further knowledge is obtained if primary adverse effects related to complementary and alternative medicine and secondary adverse effects related to interactions with conventional medicines and surgery are to be avoided. 4,5 Oftentimes, health providers are unaware of such interactions or indeed that patients are taking herbal medicines when administering conventional drugs. 6 The British Medical Association note the need for educating health care professionals on the effects and associated risks of herbal medicines, as a result of its growing interest and demand among the public. 7 Arguably, this education should begin at medical and nursing school. 8 However, recent research has shown that views on this can vary from enthusiasm to skepticism among students of medicine and the allied health sciences. 9 –16
Traditionally, complementary and alternative medicine has not been part of the curriculum at most medical universities in the United Kingdom, but this is changing. 17,18 However, there remains no systematic study of the provision of complementary and alternative medicine education in all UK-based medical schools. It was with this in mind that we decided to observe the use of complementary and alternative medicine in medical students, to assess their knowledge base about it and to identify their attitudes toward the complementary and alternative medicine education and training currently in their curriculum. In doing so, we would attempt to make a case for making complementary and alternative medicine education in medical school both standardized and compulsory among all medical schools in the United Kingdom.
Methods
Setting
This study was carried out among medical students at the University of Aberdeen. In common with other UK medical schools, the medical school has a quota for both home and international students (an annual intake of 162 and 13, respectively). 19 The duration of the course is 5 years: the first 3 years are preclinical and the last 2 years are clinical. During the clinical years, the medical students spend most of the time in the hospital with direct exposure to the patients on the wards, theatres, and in the clinics. There is currently formal teaching on complementary and alternative medicine on the curriculum that involves 1 clinical pharmacology lecture during the third preclinical year. However, this lecture is 30 minutes in duration, briefly summarizes the topic, and raises the awareness that complementary and alternative medicine exists and that the future doctors should know about it without specifically arguing a case for or against its usage.
Design
This was a questionnaire-based survey study and was conducted over a 4-week period between June and July 2010. The questionnaire was developed by the team based on previously published literature and was piloted before use in the current study. It included a brief definition of complementary and alternative medicine and highlighted therapies that come under this umbrella term (see the appendix). Questionnaires were distributed to medical students at the medical school and hospital. One of the researchers was always available to distribute and collect the questionnaire face to face to allow any queries to be answered if needed. A total of 450 questionnaires were distributed. Each responder completed the questionnaire only once.
Data Collection and Statistical Analysis
The data were collected and analyzed using IBM SPSS (SPSS, Inc, Chicago, IL) for Windows version 18. Descriptive statistics were calculated for the cumulative data on the whole sample for quantitative variables and frequencies. Chi-square testing was used to find the relationship between categorical variables. One-way analysis of variance and t tests were performed for comparison of the categorical and quantitative groups. Least significant difference testing at the 5% level of significance was used for determining significance difference. The results were considered significant at the 5% level of significance. The criterion for significance was a P value being less than .05.
Results
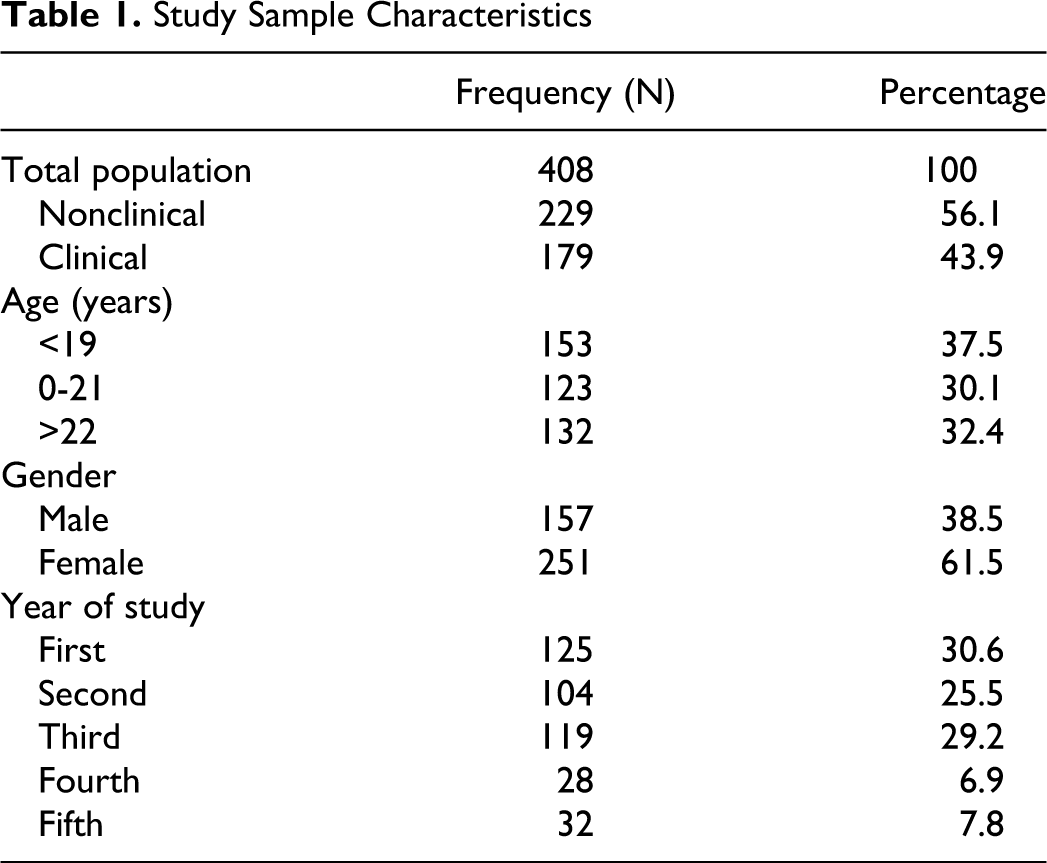
The response rate was 91% (408/450); 61% were female and 67% were 22 years old or younger (Table 1). Of the total responders, 66% (271/408) had used some form of complementary and alternative medicine. Of these, 21% were using complementary and alternative medicine currently, 21% used complementary and alternative medicine within the last 12 months, and 24% had used complementary and alternative medicine more than a year ago. The most commonly mentioned complementary and alternative medicine were aloevera, cod liver oil, and echinacea, used for immunity, concentration, and skin conditions, respectively (Table 2).
Study Sample Characteristics
Reasons for Using Complementary and Alternative Medicine

Friends and family were the most common source of information on complementary and alternative medicine (Figure 1). Of the 408, 99 (24%) students were on prescribed medications but only 16% (65/408) of responders had informed their general practitioner about complementary and alternative medicine use.
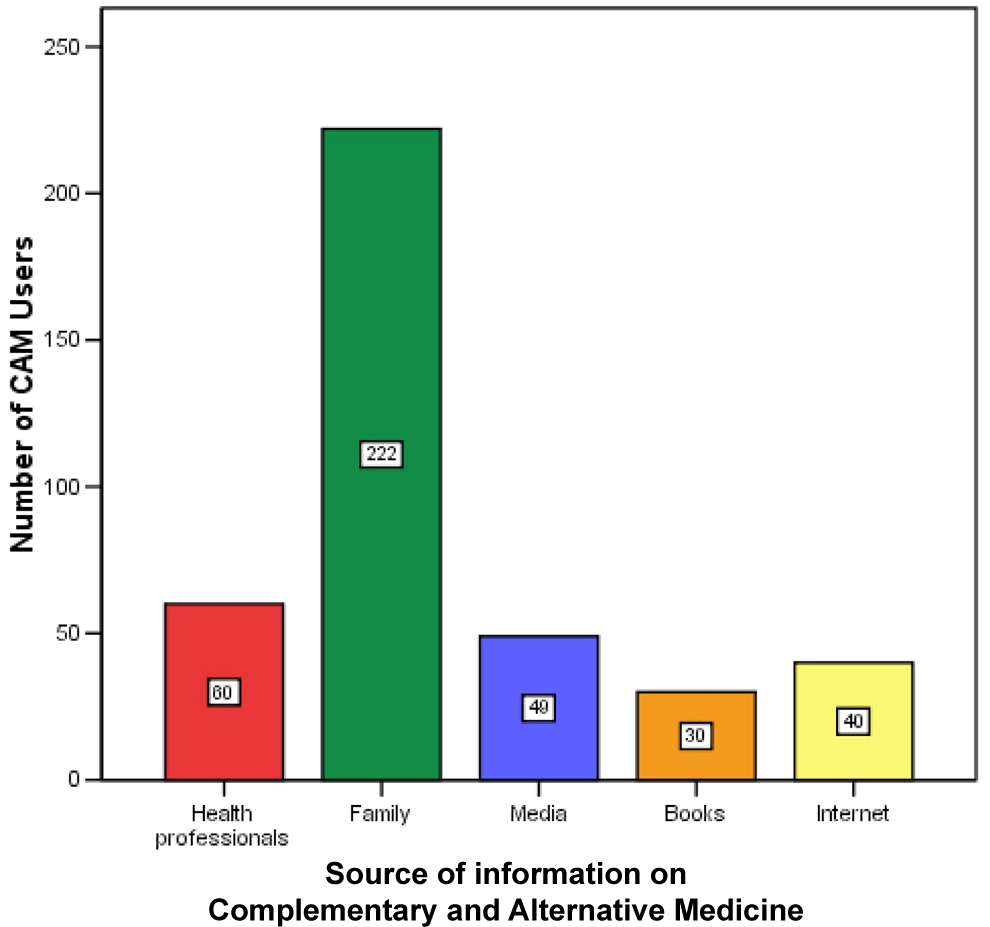
Sources of information on Complementary and Alternative Medicine
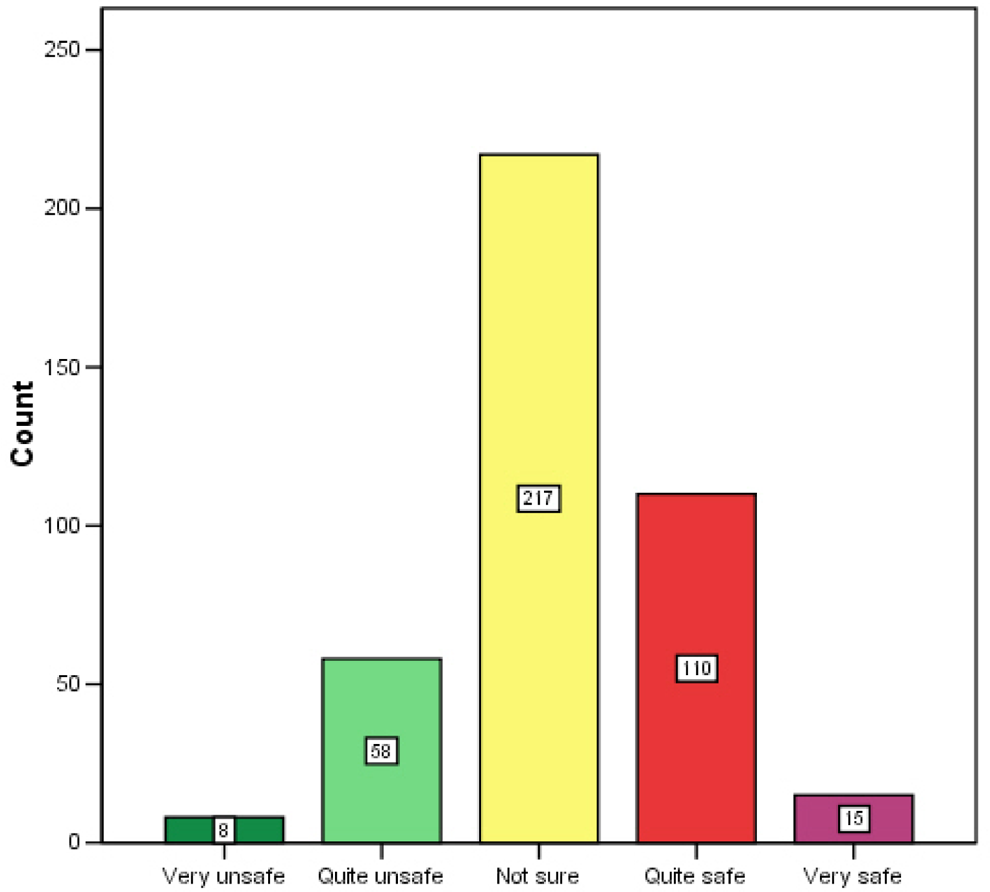
Over half of the students were not sure about the efficacy and safety of complementary and alternative medicine (Figures 2 and 3). However, only 22% (n = 88) would not recommend their use to others. The majority were equivocal (n = 233, 52%).
Effectiveness of Complementary and Alternative Medicine
Safety of Complementary and Alternative Medicine
Despite complementary and alternative medicine currently being on the curriculum, 56% (n = 253) of the students had received no formal teaching on complementary and alternative medicine; 28% (n = 127) thought that they would definitely like formal complementary and alternative medicine teaching, whereas an additional 42% (n = 187) would consider it (Figures 4 and 5).
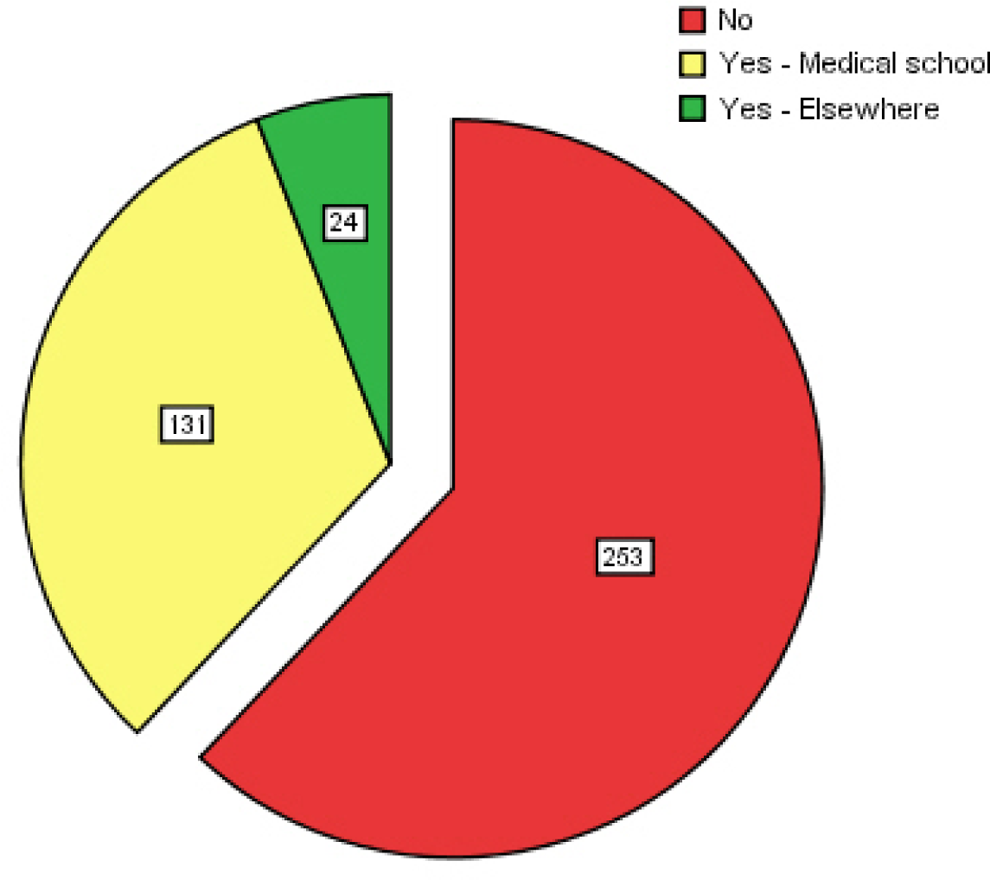
Previous teaching and training of Complementary and Alternative Medicine
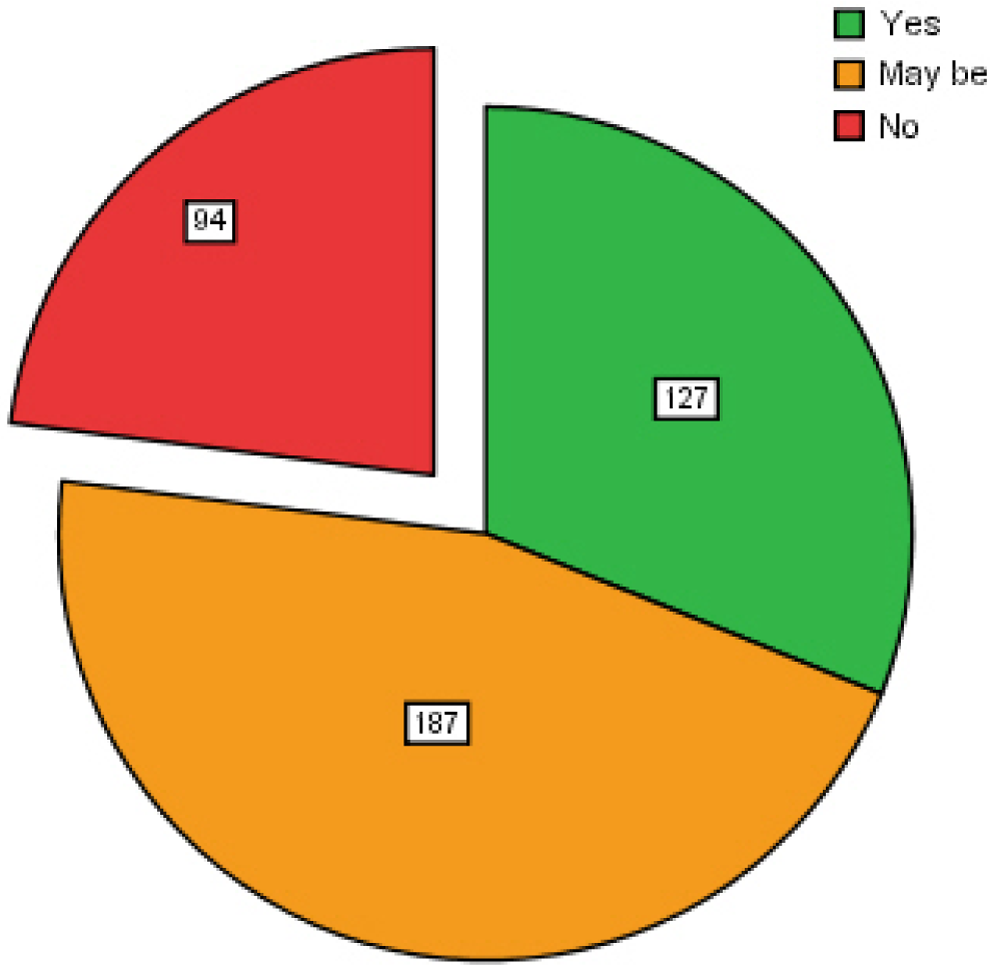
Inclusion of Complementary and Alternative Medicine teaching and training in undergraduate curriculam
There are not many differences when preclinical and clinical students were compared (Table 3). However, statistically there were significant differences in 3 parameters with respect to clinical students: they are less likely to inform their family physician regarding complementary and alternative medicine use, they have had some complementary and alternative medicine education, and they are keener to have formal education on complementary and alternative medicine as part of undergraduate teaching curriculum.
Comparison of Preclinical and Clinical Groups

Abbreviation: GP, general practitioner.
Discussion
People’s attitude toward their health seems to be changing. In Australia, 2 in 3 people use complementary and alternative medicine each year. 20 One of the reasons that explains a change from the use of conventional medicine can be the result of people adopting new and alternative lifestyles. Adopting healthy living regimes can also influence people’s choice of therapies. They feel that complementary and alternative medicine therapies offer a more natural option as opposed to the often pharmaceutical choices of conventional treatments and this can better fit in with their way of life. Another theory of consumer behavior regarding complementary and alternative medicine has shown that many people turn to using alternative therapies once they have already tried conventional medical therapy. Factors influencing their choices included severity of symptoms, consumer age, and dissatisfaction with conventional care. 21 Today’s doctors must thus have an understanding of these trends and be willing to compromise with patients by making allowances for complementary and alternative medicine use when recommending conventional therapies. Indeed, it was the academic psychiatrist George Engel who, in 1977, demonstrated that it is within the capacity of modern medicine to recognize the benefits of a holistic—in the accurate sense of the term—approach to medical care. 22 But to do so, a sound knowledge of complementary and alternative medicine is crucial if side effects and adverse drug–herb interactions are to be avoided. In 2003, Featherstone et al found in a survey of the prescribing practices of 323 Scottish general practitioner (GP) offices over a 1-year period that 60% of the practices were in fact prescribing herbal medicines and 4% of patients had been administered herbal medicines known to interact with the patients’ current prescribed conventional drugs. 23 The problem thus becomes apparent.
With respect to education on complementary and alternative medicine, 56% of the students commented that they had received no formal teaching of complementary and alternative medicine during their medical training, whereas 29% stated they had despite there being formal complementary and alternative medicine teaching on the curriculum. This can be partly due to poor attendance by the student who may already have a negative attitude toward complementary and alternative medicine or who is skeptical about its benefits and sees it as unscientific. Conversely, it can reflect the way that complementary and alternative medicine is presented to the student, who then views it as unimportant and forgettable. This skepticism coupled with unstructured teaching can result in a lack of vital knowledge concerning herbal side effects and herb–drug interactions and an unwillingness to grasp the importance of these. We found that while students were significantly more likely to have received complementary and alternative medicine education of some form by the time they were in their clinical years, they were still significantly less likely than preclinical students to report personal use of it to their general practitioner. This finding seems to illustrate the point: a general lack of structured education about complementary and alternative medicine and mounting skepticism toward it, and as students’ clinical experience grows, this lack of knowledge may consequently skew their perception of it when they enter clinical practice and possibly negatively affect future doctor–patient relationships.
In 2001, Berman stated that most medical schools have a packed curriculum, so complementary and alternative therapy options tend to be electives with only a smattering of core curriculum lectures. 24 However, this was a comment on the situation in United States-based medical schools and in response to an earlier article by Owen et al, who describe the provision of a Complementary and Alternative Medicine module in a United Kingdom undergraduate medical school. 18 Although the latter study suggests that there is a trend toward more robust teaching of complementary and alternative medicine to UK-based medical students, it would seem that Berman’s view is still the case in the school we studied. Formal complementary and alternative medicine education as part of the core curriculum still does not seem to be standard across the country.
Our study has shown that complementary and alternative medicine use among future doctors is high (66%) and more commonly used by female students that males, which may reflect usage among medical schools throughout the country. This seems at odds with the fact that only 16% claim to actually find it effective. Given that echinacea was one of the more popular complementary and alternative medicine therapies used and concentration was cited as the most common reason for its use, one reason for this apparent dichotomy may be that the academic demands of medical school and stress of examinations has driven its high usage in students willing to try a wide variety of interventions to help their success regardless of how unconventional or how little they actually believe in its effectiveness. In many cases, the advice of family and friends seems to be instrumental. Yet when comparing them with a patient population previously studied, 6 we find that medical students are still less likely to find complementary and alternative medicine effective (16% vs 54%) and also less likely overall to recommend CAM use to others (22% vs 57%). This finding adds to the hypothesis that physicians and the public differ in their views and usage of complementary and alternative medicine, and reasons may be due to subjective reasons and temperaments rather than a view of complementary and alternative medicine’s actual effectiveness.
Conclusion
This study suggests that the use of complementary and alternative medicine is common among our local medical students. It usually follows the advice of friends and family and often the general practitioner is not informed. Many students remain unaware of the potential side effects and drug–herb interactions, and such information is vital to enable them to counsel their future patients confidently about such potential risks. Education on complementary and alternative medicine use should be a standardized and compulsory part of the curriculum in all United Kingdom medical schools. Skepticism is high among many medical students with respect to complementary and alternative medicine use, and how it is taught must be considered carefully when curricula are being devised if its importance is to be accepted.
Footnotes
Appendix
Acknowledgments
We are grateful to all the medical students who participated in the survey.
Author Contributions
Ahsan Rao: Data collection and analysis and writing and finalizing the article. Muhammad Shakeel: Study concept, data collection and analysis, and writing and finalizing the article. Aaron Trinidade: Data analysis, writing and finalizing the article, and submission of the article. Ghaus Rao: Data collection and analysis and writing and finalizing the article. Amy Pearce: Data collection and analysis and writing and finalizing the article. Kim-Wong Ah-See: Study concept, data analysis, and writing and finalizing the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The institutional department of clinical effectiveness was contacted, but as it was an anonymous survey and was regarded as an audit, no formal ethical approval was required at the time of the survey. The medical students participated on voluntary basis after verbal consent.