
Abstract
Multiple myeloma (MM), a cancer of the bone marrow, is categorized as the second most common hematological malignancy of adults in the Western world. Despite dramatic improvements in immunotherapies in the field of cancers, MM immunotherapy has not been promising until now. Recent clinical studies of immune checkpoint inhibitor therapy, either alone or in combination with anticancer drugs, showed excessive side effects or low efficacy, particularly in advanced MM patients. In this context, lymphocyte levels of exhaustion markers play a pivotal role in the MM tumor microenvironment (TME). Hence in the present review, the mechanisms relevant to MM of five inhibitory molecules including T-cell immunoreceptor with Ig and ITIM domains (TIGIT), T-cell immunoglobulin, and mucin domain 3 (Tim-3), lymphocyte activation gene-3 (LAG-3), V-domain Ig Suppressor of T-cell activation and killer immunoglobulin-like receptors along with bispecific T-cell antibodies (BsAbs) will be discussed. Further, we summarized the underlying biology of these checkpoints in cancer and their rapidly emerging role in pathways in MM along with presenting recent clinical trials in context.
Introduction
Cancer immunotherapy for the treatment of neoplastic disease has been consistently raising attention over the past century. Multiple myeloma (MM) is a cancer of clonal plasma cells that accounts for approximately 10% of hematological malignancy. 1 In multiple myeloma, the bone marrow (BM) microenvironment, including the immune cell components, is pivotally involved in disease development and pathogenesis. 2 In the BM microenvironment, the extensive interaction among bone marrow stromal cells (BMSCs), BM endothelial cells, and the MM cells may lead to secretion of various cytokines such as hepatocyte growth factor, transforming growth factor-β (TGF-β), vascular endothelial growth factor, and stromal cell-derived factor-1α (SDF-1α) that increase myeloma cells durability. 3 The interaction between myeloma cells and BMSCs releases interleukine-6, which further enhances the durability of the malignant cells and, interestingly, the association between increased levels of IL-6 and IL-17A and survival has been recently reported in patients with newly diagnosed multiple myeloma.4,5 Under optimal physiological circumstances, the immune system actively eliminates neoplastic cells persistently emerging. 6 In this context, the tumorigenic antigens that are recognized by major histocompatibility complexes are introduced to antigen-presenting cells (APCs), including dendritic cells, macrophages, and B cells, that finally differentiate effector T cells to recognize and eliminate cancer cells. 7 This precise cell-mediated immune response is regulated by either costimulatory or co-inhibitory signaling molecules. In addition, the roles of the secretion of various immune mediators that influence cell-mediated immunity should not be neglected. 8 The cytotoxic tumor lymphocyte antigen 4 (CTLA-4) and the programmed cell death-1 (PD-1) are the most studied co-inhibitory molecules that belong to B7-CD28 group of proteins on the surface of T cells, B cells, and natural killer (NK) cells, which favor immune tolerance. The immune response can also be suppressed upon binding of PD-1 on the surface of immune cells with its associated ligand PD-L1, either on APCs or cancer cells. Hence, the cancer cell growth can be due to either suppression of T-cell activation or escaping of cancer cells from immune surveillance.9–11 Further, two ligands, CD80 (B7-1) and CD86 (B7-2), which are approximately 25% identical in gene sequence to cytotoxic tumor lymphocyte antigen-4 or CD28 also restrict the production of antigen-specific T cells. 12 Various studies revealed the elevated expression levels of both CTLA-4 and PD-L1 in BM plasma cells of patients with MM.13,14 The aberrant expression of PD-1 on peripheral blood CD4 T cells in patients diagnosed with MM has been correlated with the compromised functionality of CD4 T cells throughout the progression of the disease. 15 In patients with active myeloma that exhibit increased PD-1 expression in T cells, the PD-1 blockade by anti-PD-1 antibody, improves ex vivo T-cell responses to autologous DC/tumor fusion stimulation. 16 Further to the aforementioned two important inhibitory immune checkpoints, there are other crucial inhibitory molecules that are involved in the immune function of T cells in MM. 17 This review delineates the mechanistic involvement, specifically in MM, of five inhibitory molecules, namely T-cell immunoreceptor with Ig and ITIM domains (TIGIT), T-cell immunoglobulin, and mucin domain 3 (Tim-3), Lymphocyte activation gene-3 (LAG-3), V-domain Ig Suppressor of T-cell Activation (VISTA) and killer immunoglobulin-like receptors (KIRs); alongside with bispecific T-cell antibodies (BsAbs). Further, their underlying biology and their rapidly emerging role in pathways in MM along with the recently conducted clinical trials are presented.
Role of classical co-inhibitory molecules PD-1/PD-L1 in pathogenesis of MM
Over the past decade, the anti-PD-1 (pembrolizumab, nivolumab, and cemiplimab) and anti-PD-L1 (atezolizumab, avelumab, and durvalumab) agents have been used for immune checkpoint blockade (ICB) therapy in various cancers; however, until now they have shown clinical benefits only in a few hematological malignancies.18,19 It has been proposed that the communication between MM cells and BM stromal cells enhances tumor survival by blocking CD4+ T-cell activity via the interaction between PD-L1 and PD-1. 18 Despite the PD1/PD-L1 immunosuppressive mechanism of action in various solid tumors and MM, the accumulating data indicate the lack of adequate responsiveness or even resistance to anti-PD-L/PD-1 therapy. Conversely, in relapsed or refractory MM a combination of pembrolizumab with dexamethasone and lenalidomide in a phase Ib trial has shown a 50% overall response rate while the ORR decreased to 38% in lenalidomide-refractory patients. 20 Notably, a 60% ORR was seen for a combination of pembrolizumab with pomalidomide and low-dose dexamethasone for relapsed/refractory multiple myeloma (RRMM). 21 These studies further highlighted the importance of the anti-PD-1 therapy in combination with various phase III trials, including Checkmate 602 (pomalidomide and dexamethasone ± nivolumab in relapsed myeloma), Keynote-183 (pomalidomide and dexamethasone ± pembrolizumab in relapsed myeloma), and Keynote 185 (lenalidomide and dexamethasone ± pembrolizumab in myeloma. 22 Importantly, all these trials were stopped in September 2017 by the FDA due to increased risk of death due to autoimmune disorders such as myocarditis and pneumonitis, as compared to the control group. There are factors that influence the efficacy of PD1/PD-L1 blockade strategy, including T-cell function, the levels of PD-L1 and PD-1 expression, tumor microenvironment, and its immunogenicity. In this context, there has been an association between resistance to therapeutic PD-1 blockade and upregulation of alternative immune checkpoints. 23 For example, in an experimental study of lung cancer, the analyses of the tumor microenvironment TME have shown that following anti-PD-1 therapy in two fully immunocompetent mouse models of lung adenocarcinoma, an increased regulation of TIM-3 has observed that hampered the treatment. Consistently, another study of nivolumab in a PD-1 blockade phase IB trial in 27 MM patients has also shown little effect due to stimulation of immunosuppressive cells, including Treg or exhausted T cells. 24 Importantly, the PD-1+CD8+ T cells from the BM of MM patients at advanced-stage co-expressed RAG3 and TIGIT and further indicated the blockade of the PD-L1−PD-1 pathway alone could not sufficiently recover T-cell function while TIGIT ICB improved the treatment strategy. 25 Regarding the low efficacy of anti-PD-1 blocking antibody treatment, the properties of exhausted T cells that can limit current immunotherapy approaches also deserve particular attention. 26 Pauken et al. 26 have found that reinvigoration of exhausted CD8 T cells (TEX) in mice by PD-L1 blockade could minimize memory development. The PD-L1/PD-1 blockade might be an effective therapeutic approach particularly when it comes in association with other anti-MM therapeutic strategies. In this context, the potential immunomodulatory effects of immunomodulatory drugs (IMiDs), including suppression of regulatory T cells and myeloid-derived suppressor cells, the stimulation of T and NK cells, and their effects on decreasing PD-1 expression on T cells should not be overlooked. The CD38 as a type II transmembrane glycoprotein is a multifunctional protein and has a double function as receptor and ectoenzyme. 27 Regarding enzymatic function, isatuximab readily inhibits cyclase and hydrolase activity through binding to CD38 ectoenzyme catalytic site without altering its configuration while daratumumab, especially inhibits cyclase activity with enhancing the hydrolase activity via binding to specific epitope outside of the CD38 catalytic site. 28 The increased efficacy of anti-PD-L1 agents through inhibition of extracellular adenosine (ADO) production also deserves attention. The ADO that is produced in tumor microenvironment enhances tumor cell survival through its binding with purinergic receptors. The over-expressed CD38 in all stages of myeloma also can regulate the calcium signaling through catalyzes of extracellular conversion of nicotinamide adenosine dinucleotide (NAD+). The NAD+ also is the main intracellular purine resource in the tumor microenvironment for producing ADO. 29 The ADO binding to adenosine receptors (AdoRs) inhibits tumor adaptive immunity through various mechanisms, including suppressing tumor antigen presentation and downregulation of major histocompatibility complex II (MHC II). Further, the ADO inhibits antitumor cytokine and chemokine secretion with consequent inhibition of T-cell receptor (TCR) binding or disruption T-cell infiltration into the tumor site. 30 These findings suggest that there might be an interaction between CD38-mediated immune response and the PD-L1/PD-1 axis in the MM microenvironment. In this context, unveiling the anti-CD38 antibodies signaling pathways for the treatment of MM patients is of high clinical importance. Consequently, elucidating the signaling pathways activated by anti-CD38 antibodies for the therapeutic management of MM patients holds substantial clinical significance.
V-domain Ig suppressor of T-cell activation
In the B7 family, the VISTA is a type I immunoglobulin membrane protein with 55–65 kDa molecular weight that is also known as differentiation of embryonic stem cells 1, platelet receptor Gi24 precursor, B7-H5, SISP1, DD1α and programmed death protein-1 homolog (PD- 1H). It shares 22% homology with PD-L1 while having large structural differences with CD276, CD80, and CD86 in the same family. 31 The VISTA expression in hematopoietic, myeloid cells, and mature APCs has been identified with its potential action as a T-cell checkpoint inhibitory ligand. The proposed role of VISTA in suppressing T-cell activity is supported by several experimental approaches: (a) an engineered checkpoint receptor agonist (VISTA.COMP) targeting the putative VISTA-receptor inhibits T-cell–mediated immune responses, (b) genetic disruption of VISTA in mice altered immune reaction to neoantigen and enhanced susceptibility to the development of autoimmunity (c) an engineered anti-VISTA antibody (SG7) blocks the VISTA interactions with both PSGL-1 and VSIG-3 proteins and inhibits its activity in humans and mice.32–34 The two specific and potential VISTA ligands including V-Set and Immunoglobulin Domain Containing Protein-3 (VSIG-3) and P-Selectin Glycoprotein Ligand 1 (PSGL1) have recently been seen to be highly expressed on tumor and stromal cells.35,36 In this context, the VISTA can act with both functions either as a T-cell co-inhibitory ligand and a co-inhibitory receptor. 37 Although in MM the VISTA plays an important role in the immune regulation of T cells, the precise mechanisms by which the cancerous plasma cells escape T-cell immunity are yet to be discovered. A recent study conducted by Mutsaers et al. indicates that tumor infiltrating CD11b+ myeloid cells have higher VISTA expression, and interestingly cells that are strongly positive for both VISTA and CD11b in a tumor are significantly associated with poor survival. 38 Further, analyses of the BM tissue compartmentalization of VISTA+, CD11b+ cells, and CD8+ T cells in patients with MM revealed that VISTA+ and CD11b+ cells in the tumor have been associated with low circulation of CD8+ T cells into the same compartment. Consistently, a high VISTA expression on CD11b+ myeloid cells in tumors has been previously discovered in mice. 39 The observed correlation between heightened VISTA and CD11b expression within tumors, coupled with the absence of CD8+ T cells in tumors (but not in stroma), and its concurrent association with diminished survival rates, implies a potential role of increased VISTA expression on CD11b+ cells preventing the infiltration of newly circulating CD8 T cells into tumor sites. The activation of integrin CD11b, which belongs to a family of adhesion receptors promotes pro-inflammatory macrophage polarization through expression of microRNA Let7a, which can lead to antitumor immunity. 40 Hence, to target CD11b for cancer immunotherapy, it should be also of interest to investigate the influence of VISTA expression on the CD11b+ cells toward recruitment of CD8+ T cells into the TME. In this context, the ligation of other ligands such as VSIG3 or PSGL1 with CD11b+ myeloid-derived suppressor cells, should not be further overlooked. Of interest, the concurrent expression of VISTA with other immune checkpoints on T-cell subsets either in peripheral blood or BM of affected patients also deserves attention. Huang et al. reported double-positive expression of VISTA with other checkpoints including VISTA+PD-1+, VISTA+Tim-3+, and VISTA+TIGIT+ CD3+/CD4/CD8+ in peripheral T cells. 41 Further, high expression of VISTA+ T cells and VISTA+PD-1+/Tim-3+/TIGIT+ T cells from peripheral blood was also found. These results strongly indicate that the increased VISTA expression on peripheral T cells compared with BM T cells should be investigated precisely. Additionally, it emphasized that the elevated expression of VISTA in Tregs in MM should be associated with Tregs activation and upregulation. In this context, determining the levels of VISTA expression either alone or in combination with PD-1, Tim-3, and TIGIT on various T-cell subsets, including CD3+, CD4+, Treg, and CD8+ is urgently suggested. To summarize: Blocking of VISTA can potentially prevent T-cell depletion while it improves T-cell function in patients with MM. Consistently, transcriptomic analysis conducted independently on 718 patients with MM enrolled in trials alongside analysis of 1654 samples of BM from various clinical trials revealed that the VISTA+, CD11b+, and CD8+ cell combined scores can potentially be associated with immunotherapy prognosis. 17
Killer immunoglobulin-like receptors
Cytotoxic lymphocytes including NK cells along with subsets of activated CD8+ T cells express important surface inhibitory receptors known as KIRs that specifically bind to MHC class-I which is also called human leukocyte antigen (HLA) class-I. 42 The KIRs have both stimulatory and inhibitory activity through KIRxDS and KIRxDL, respectively. The inhibitory activities of KIRs are transmitted with a long cytoplasmic tail (L), while those with short cytoplasmic tails (S) transmit stimulatory signals, however, the HLA class-I ligands interact with both of them. 43 Several KIRs that bind with HLA molecules as their ligands include (a) KIR2DL1 and 2DS1, (b) KIR2DL2, 2DL3, and 2DS2, (c) KIR3DL1, and (d) KIR3DL2 that recognize the HLA-C2 group, HLA-C1 group, HLA-Bw4 with HLA-A3 and finally A11, respectively. 44 The distinct interactions between these receptors and their associated ligands mediate the effects of KIRs on host immune response. The main inhibitory receptors of NK cells that recognize HLA class-I ligands and are known as conventional inhibitory receptors are KIR, CD94 associated with NKG2A, and LILRB1. 45 In a MM mouse model study, the anti-myeloma NK-cell activity increased when the anti-inhibitory KIR antibody 1-7F9 (also called IPH2101, which cross-reacts with KIR2DL1, -2, and -3 receptors), and lenalidomide both were used. 46 In another study, the NK-cell-mediated lysis of HLA-C–expressing tumor cells was increased by 1-7F9 monoclonal antibody (mAb) which indicates an enhancement of NK-cell cytotoxicity. 47 In contrast to this finding, a study revealed that the infusion of IPH2101 monoclonal antibodies (mAbs) in patients with myeloma, resulted in a rapid decrease in both NK-cell reactions and KIR2D expression on the NK-cell surface. 48 In this study, the reduction of NK-cell functionality that was associated with the loss of free KIR2D surface protein could be due to trogocytosis, a process that either result in cell death or acquisition of altered functions in recipient cells via antibody-dependent cytotoxicity mechanisms or intercellular protein transfer, respectively. 49 In this context, other factors such as the heterogeneity of KIR expression that influences KIRs mAbs targeting should not be neglected. Targeting potential therapeutic candidates like HLA-E binding peptides that are expressed on the MM plasma cells further deserves attention. 50 Clinical trials examining the NK anti-KIRs monoclonal antibody 1-7F9 (IPH2101) are presented in Table 1. Last but not least, the association of the expression levels of KIR and its ligands with the response to treatment in MM has been recently identified. In this context, Thai patients with MM, have shown lower frequencies of KIR3DL1 and 2DS4 compared to controls (p = 0.02). Interestingly, after treatment with bortezomib, patients who achieved more than a very good partial response (VGPR) showed higher frequencies of KIR3DL1, 2DS4, 2DL1 with C2, and 3DL1 with Bw4 compared with those patients with a VGPR or worse response. 44
Conducted clinical trials evaluating NK anti-KIRs monoclonal antibody for multiple myeloma immunotherapy.

NK, Natural killer; KIR, killer immunoglobulin-like receptors.
Lymphocyte activation gene-3 (LAG-3)
Numerous immune cells such as T cells, regulatory T cells (Tregs), natural killer cells (NK cells), natural killer T cells (NKT cells), activated B cells, plasma cells, and plasmacytoid dendritic cells (pDCs) express a transmembrane molecule closely related to CD4, that is named lymphocyte activation gene-3 (LAG-3).51,52 Galectin-3 a 31-kDa lectin, liver sinusoidal endothelial cell lectin (LSECtin), MHC II, and fibrinogen-like-protein 1 (FGL1) are four ligands for LAG-3 with inhibitory activities on antitumor T-cell dependent responses.53,54 LAG-3 exerts inhibitory effects on T-cell activation by either competing with CD4 for binding with human leukocyte antigen class II (HLA-II) or binding with fibrinogen-like protein 1 FGL-1. Preclinical investigations have demonstrated that mAbs targeting LAG3-FGL-1 axis enhanced antitumor T-cell activity.55,56 LAG-3 is expressed in various tumor types and alters the tumor microenvironment via immunosuppressive activities. 57 In the tumor microenvironment of MM patients, effector T-cell responses were enhanced by blocking immune checkpoints PD1 and LAG3 either alone or in combination. 53 In MM patients, increased LAG-3 expression along with increased surface and intracellular expression of galectin-3 were observed in proliferating CD3+ T cells and CD138+ cells, respectively. In these patients, blocking LAG3/GAL-3 improved the proliferation of T cells and their functional activities against MM via XBP1/CD138/CS1-targeting memory CD8+ T cells. 53 The pathological shift including increased expression of T-cell inhibitory molecules LAG-3 during smoldering MM evolution, also highlights its potential as an immunotherapy target. 58 Importantly, a recent study further confirmed that type 1 interferons (IFN-I) can regulate co-inhibitory receptor expression, including PD-1, TIM-3, and LAG-3 on human T cells. 59 In this context, the investigation of potential transcription factors that differently regulate co-inhibitory receptor expression under IFN-I secretion may provide a rationale for further investigation of immunotherapy in human cancer. On iTreg cells, the expression of LAG-3 can induce secretion of transforming growth factor beta (TGF-β1) and IL-10 that results in inhibition of Tregs and subsequently tumor immune escape. Interestingly, the study performed by Wang et al. indicates interleukin-10 plays a pivotal role in immune suppressive microenvironment in MM. 60 In this study an elevated serum IL-10 was associated with various clinical factors with prognostic significance like increased lactate dehydrogenase (LDH) levels, high international staging system (ISS stage), and poor performance status. These findings may indicate the level of serum IL-10 as a prognostic factor in MM that should be more investigated. In this context, the LAG-3+ T cells that represent a new Tregs subset that can induce interleukin-10 secretion with its potential role as biomarkers for a treatment approach in autoimmune disorders have been discussed elsewhere. 61 Even though important progress has been made in hematological cancer immunotherapy, the mechanisms in which LAG-3 governs its functional properties, including its expression in correlation with overall prognosis, need to be entirely evaluated. A phase I/II randomized trial of anti-LAG-3 and anti-TIGIT agents either alone or combined with pomalidomide and dexamethasone for evaluation of their safety and immune efficacy in patients with relapsed refractory MM is ongoing. Targeting compounds and conducted clinical trials examining potential anti-LAG-3 in hematological malignancy are presented in Table 2.
Conducted clinical trial evaluating anti-LAG-3 antibody for multiple myeloma immunotherapy.

LAG-3, lymphocyte activation gene-3.
T-cell immunoreceptor with Ig and ITIM domains
The activated T cells and NK cells express other important inhibitory immune checkpoints that are named T-cell immunoreceptors with Ig and ITIM domains. Multiple ligands bind to TIGIT among which is the poliovirus receptor (PVR) characterized by a singular extracellular immunoglobulin variable domain and a short intracellular domain. The type I extracellular transmembrane domain shares sequence homology with DNAM-1, CD96, CD155, CD111, CD112, CD 113, and PVRL4. 62 The short intracellular domain includes one ITIM and one immunoglobulin tyrosine tail (ITT)-like motif while the ITIM has an identical sequence in mice and humans.62,63 These ligands, prominently expressed on cancerous cells, elicit inhibitory responses that impede the antitumor capabilities of both T and NK cells. 64 Recently, an IgG4-type monoclonal antibody against human TIGIT known as MG1131 has been developed that interacts with TIGIT more firmly than the PVR receptor. In patients with MM, MG1131 improved NK-cell-mediated tumor-killing properties along with inhibitory activity on Tregs-mediated immune suppression. Moreover, MG1131 improved Interferon-gamma (IFN-gamma) secretion from peripheral blood mononuclear cells and it has been proven that IFN-gamma can act as an inhibiting factor on myeloma cell proliferation.64,65 By observing these results, authors concluded that MG1131 improves the effector functions of T cells and NK cells while influencing negatively Treg cell activity. Consistent with this finding, the overexpression of TIGIT in NK and T cells has been found to be associated with tumor immune escape with decreased secretion of activating immune mediators including interferon-γ (IFN-γ) and tumor necrosis factor-alpha (TNF-α) in patients with myelodysplastic syndromes. 66 Another signaling pathway that induces NK-cell exhaustion is the interaction between CD155 and the TIGIT in the regulation of BMSC. 67 In newly diagnosed MM patients (NDMM), CD155 is highly expressed on bone marrow stromal cells (BMSCs) while its expression is very low on myeloma cells. The TIGIT immunoglobulin domain is able to bind with their ligands CD155, CD226, CD112, and CD113 with high affinity for CD155. Importantly, the CD155/TIGIT signaling can stimulate BMSC-induced NK-cell exhaustion and in vitro co-culture showed that TIGIT blockade may rebuild NK-cell exhaustion by BMSCs and subsequently impede myeloma progression. In light of the restricted efficacy observed in impeding inhibitory immune checkpoints among MM patients, there is a need to discern alternative immune inhibitory ligands. 68 Within this framework, investigating the inhibitory interactions of newly identified ligands like PVRIG that induce inhibitory signals to T and NK cells is suggested. Further, analyzing the expression of novel ligands including PVRL2 and PVR in the content of DNAM1 axis also deserves attention. The conducted clinical trials examining potential anti-TIGIT in MM are presented in Table 3.
Conducted clinical trial evaluating anti-TIGIT antibody for MM immunotherapy.
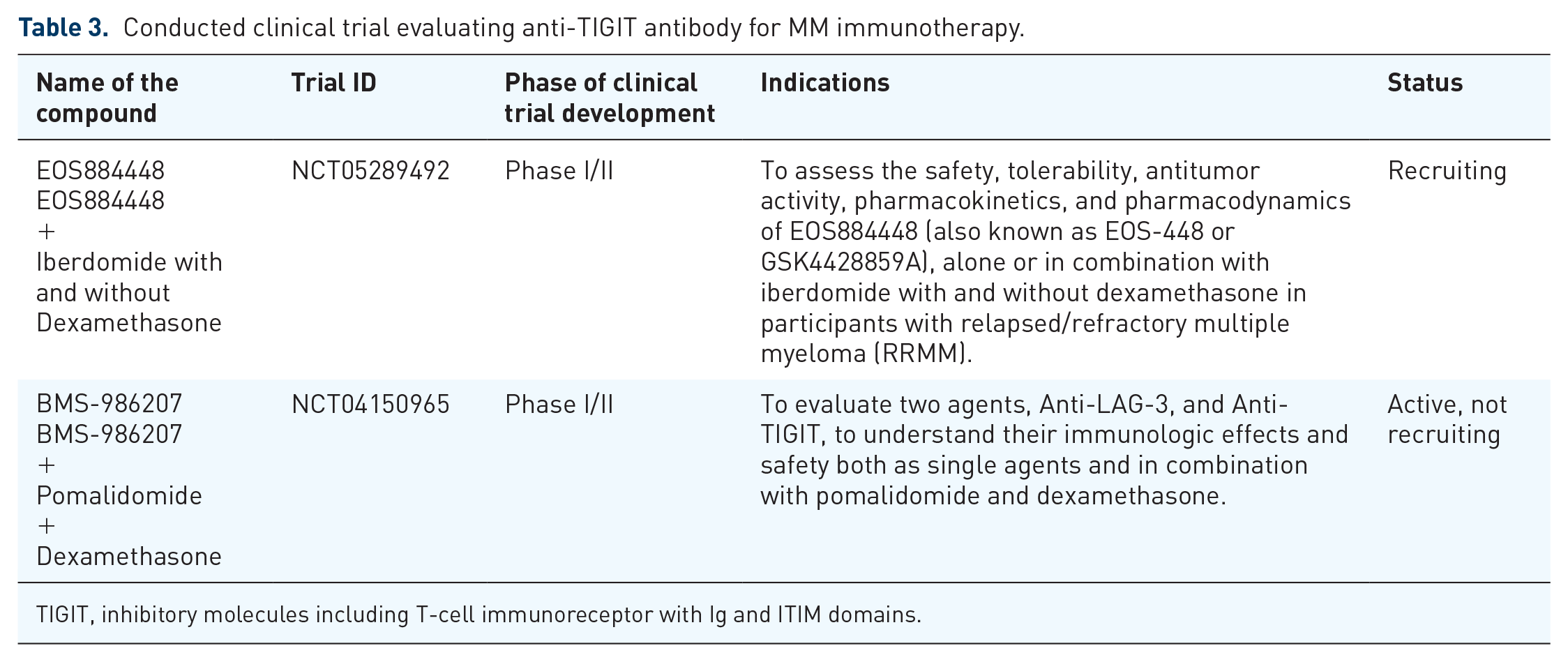
TIGIT, inhibitory molecules including T-cell immunoreceptor with Ig and ITIM domains.
T-cell immunoglobulin and mucin domain 3 (Tim-3)
Tim-3 that belongs to the immunoglobulin superfamily is mostly expressed at higher levels either by CD8+ TILs and CD4+ regulatory T cells (Treg) with four associated ligands such as galectin-9, phosphatidylserine (PtdSer), high mobility group protein B1 (HMGB1), and carcinoembryonic antigen-related cell adhesion molecule-1 (CEACAM-1). As an inhibitory regulating molecule, the interaction of Tim-3 with its associated ligands like galectin-9 (Gal-9) enhances lymphocyte apoptosis while its blockade exacerbates autoimmunity and tumor immune escape. 69 The expression of Tim-3 is not limited to immune cells and its expression on tumor cells also deserves attention. Tim-3 is expressed on a variety of solid tumors including prostate cancer cells, non-small cell lung cancer, gastric cancer, and hepatocellular carcinoma (HCC).70–73 Among blood cancer types, a high expression of Tim-3 has been reported in leukemic stem cells in acute myeloid leukemia (AML), hematopoietic stem cells in myelodysplastic syndrome (MDS), and lymphocytes in MM.41,74–76 Among immune cells NK cells are known for their effective antitumor activity while Tim-3 negatively regulates them in malignancies. Importantly, elevated levels of Tim-3 expression have been reported on NK cells of BM and peripheral blood of MM patients. 77 Increased cytolytic activity of NK cells was observed in both human MM cell lines and primary MM cells subsequent to Tim-3 blockade, facilitated through diverse mechanisms such as the upregulation of perforin, granzyme B, TNF-α, and IFN-γ. 77 Consistently elevated Tim-3 expression, especially at the tumor site has been associated with tumor invasion, and upregulation of TNF-α molecules in human esophageal cancer. 78 In the BM, high expression of Tim-3 on myeloma cells has been positively correlated with β2 microglobulin, creatinine, and plasma cells while negatively associated with hemoglobin and red blood cells. 79 Notably, the treatment of MM cell lines either RPMI-8226 or U266 with Tim3 knock-down agents has shown to inhibit cell proliferation along with induction of cell apoptosis. 79 In a completed phase Ib, multi-arm, open-label study in patients with AML or intermediate or high-risk myelodysplastic syndrome (MDS) with trial ID (NCT03066648), 51 vHR/HR-MDS (very high risk/high risk), and 40 ND-AML patients that treated with spartalizumab (a humanized monoclonal antibody targeting PD-1) or sabatolimab (a high-affinity, humanized, IgG4 antibody targeting TIM-3), either alone or in combination have shown a higher overall response rate (ORR) and 1-year progression-free survival (PFS). 80 In another clinical trial (NCT03946670), which was a double-blind, placebo-controlled phase II study that enrolled 127 patients with intermediate-risk, high-risk, and very high-risk MDS, treatment with either sabatolimab plus hypomethylating agent (HMA) or placebo plus HMA has shown a primary complete remission (CR) rate of 21.5% and 17.7%, respectively. These studies further indicate that Tim3 might be a pivotal inhibiting checkpoint molecule in the treatment of MM.
Other potential MM antigens and immunotherapy strategies
Bispecific T-cell antibodies (BsAbs) are recombinant molecules with two binding sites, one is involved with binding to the tumor cells epitopes that is currently associated with B-cell maturation antigen (BCMA), CD19, CD38, FC receptor-like5 (FCRL5) or G protein-coupled receptor class C group 5 member D (GPRC5D) while with the other site binds to T and NK immune effector cells through CD3 and CD16, respectively. 81 Bispecific T-cell engagers (BiTEs) are other structurally and functionally similar molecules to BsAbs with two linked single-chain variable fragments (scFvs). These molecules activate polyclonal T-cell reactions independent of MHC and TCR and the simultaneous interactions of two binding sites activate T cells and subsequently lead to tumor killing. 82 Besides binding to CD3, these antibodies bind to specific tumor antigens and co-localize T cells with tumor cells to enhance T-cell’s activities. Compared to the bispecific antibodies (BsAbs), the BiTEs have lower molecular weight and shorter half-life and consequently, they have shorter intervals of injection for immunotherapy. 83 Summaries of recently conducted clinical trials examining the potential BsAbs in combination with PD-1 inhibitors in MM are presented in Table 4. In addition to MM immune checkpoint inhibitors (ICI) therapy, recent therapeutic approaches like chimeric antigen receptor-T (CAR-T) cell therapies also deserve attention. In MM, there are various antigens for the CAR-T cell treatment strategy, including CD19, CD138, light chains, NKG2D, and B-cell maturation antigens. 84 In 16 patients with R/R myeloma that received 9 × 106 CAR-BCMA T cells/kg against CD28 costimulatory domain, an overall response rate (ORR) of 81% was observed. 85 Despite the high OR in this study, the elevated toxicity level for 94% of patients who developed cytokine release syndrome (CRS) should not be neglected. Interestingly, recently, in treatment of French patients with relapsed/refractory myeloma that was treated with Ide-cel at expansion of circulating CAR-T cells to more than 180 mm3 after infusion, prolonged PFS was seen while 92% of patients have shown grade 1–2 CRS and only one patient has shown grade 3 or more. 86 In this context, the combined use of CAR-T cell therapies with ICI for the treatment of hematological malignancies also deserves attention. In patients with refractory/relapsed B-cell non-Hodgkin lymphoma (B-NHL), the combined treatment of nivolumab with anti-CD19 CAR (CD19 CAR)-T cells mediated potent anti-lymphoma activity. 87 Regarding the adverse effects, 25% (3/11) showed grade 1 CRS while 50% (6/11) of them showed grade 2. In this study, the good objective and complete response rate at 81.81% and 45.45%, respectively, highlighted the need for further investigation in clinical trials. Car-T cell therapies either combined or in sequential treatment with ICI applied in hematological malignancies have been reviewed systematically elsewhere. 88 In summary, heterogeneous efficacy outcomes have been seen for combined or sequential treatment of ICI (particularly PD1/PDL1 inhibitors) and CAR-T therapies for hematological malignancies. Based on the results obtained so far, the combination strategy has not been proven to be superior as compared to CAR-T cell monotherapy. The combination has shown manageable toxicities with a toxicity profile comparable to CAR-T cell monotherapy. Last but not least, the new studies regarding vaccine therapy for the treatment of MM should not be neglected. In this context, a phase I PD-L1 peptide vaccination with IO103 and adjuvant Montanide should be addressed. In this study, ten patients with MM who had been previously treated with high-dose chemotherapy were examined. All patients have shown peptide-specific immune responses measured either by IFNγ enzyme-linked immunospot assay or intracellular cytokine staining from blood and skin infiltrating lymphocytes. Average responses to PD-L1immunization were seen with moderate adverse reactions mostly at injection site. 89 Three out of ten patients had an enhanced response to treatment with peptide vaccinations. Based on myeloma anticancer vaccinations, several clinical trials in combination with other peptides like IDO, PD-L2, and arginase have been under study (NCT03381768, NCT03939234, and NCT04051307).
A summary of the recently conducted clinical trials examining the potential BsAbs in combination with checkpoint inhibitors therapy in MM.

Concluding remarks
In recent years, the therapeutic potential of checkpoint inhibitors are being studied either alone or in combination for hematological malignancies. Despite significant advancement in understanding the functions of ICI for unveiling the pathways by which the cancerous cells escape the immune system, so far none of the examined inhibitory molecules have shown promising therapeutic potential in MM. Mechanisms that mediate resistance to MM immunotherapy vary and include induction of IL-10 as an immunosuppressive immune mediator, molecular cascading of MM cells to protect them from lysis, Treg cell suppression, and finally T-cell exhaustion. Other immune factors like APCs and effector T cells function or tumor mutation properties have been found to be associated with autoimmune disorders and infectious complications. Additionally, other new approaches including combined PD-1 inhibitors with radiation therapy also deserve attention. It presumed that combined and multiple immune checkpoint markers have a significant potential for escaping MM cells from the host immune system. Despite the potential of PD/PD-L1 blockage by pembrolizumab immunotherapy in MM, compelling clinical trials so far have shown disappointing results. The combination of checkpoint-inhibitor (CPI) with immunomodulatory agents like IMIDs have shown promising results. Significant gene expression alterations in MM tumor microenvironment along with elevated number of monocytes, NK cells, and monocytes were observed in combined treatment of durvalumab (a human immunoglobulin G1 kappa monoclonal antibody) and pomalidomide in patients with relapsed/refractory MM. 90 However, pembrolizumab in combination with IMiDs, lenalidomide or pomalidomide has shown immune system-related toxicities (such as infection, neutropenia, and pneumonia), particularly in RRMM patients. Hence due to the reduced survival and increased adverse effects in these patients, the clinical trials of IMiD agents in combination with CPIs were postponed. It should be mentioned that monotherapy with nivolumab has shown an equal safety profile in RRMM patients. From these points of view, the potential targets of checkpoint inhibitors for immunotherapy would be those with increased and uniform expression on the cancerous cells. However, in the pursuit of optimal treatment, it is imperative to explore the prospective roles of newly identified immune checkpoints highlighted in this review, namely VISTA, KIRs, lymphocyte activation gene-3 (LAG-3), T-cell immunoreceptor with Ig and ITIM domains (TIGIT) and T-cell immunoglobulin and mucin domain 3 (Tim-3), whether employed individually or in combination, to ascertain their efficacy in MM immunotherapy. In this context, unveiling the precise molecular interactions regulated by BiAb/BiTE whether in the treatment of RRMM patients or the earlier lines of treatment remains a critical area of investigation.