
Abstract
Since antiquity, the interaction of brain and heart has inspired physicians and philosophers. Today, our knowledge has vastly improved, but the exact way of their interaction still holds many secrets to reveal. The interaction between brain and heart merits particular attention in the aftermath of a sudden injury to the brain-like acute ischemic stroke (AIS). This narrative review gives an overview of current knowledge on frequency, prognosis, and potential pathophysiological mechanisms of myocardial injury following AIS.
Keywords
Preface
“Tell me where is fancy bred, or in the heart or in the head”
The Merchant of Venice, Act III, Scene 2, William Shakespeare
Introduction
Diseases of the heart and the brain are closely entangled. Vascular diseases of both organs share the same risk factors. Pathophysiology of atherosclerotic vascular heart and brain diseases overlap and many therapeutic strategies are similar. Moreover, at least one in five ischemic strokes originates from the heart. 1,2 These so-called cardioembolic strokes may be caused by a variety of heart conditions including but not limited to atrial fibrillation, intracardiac thrombus, prosthetic cardiac valve, recent (<4 weeks) myocardial infarction, reduced ejections fraction, or endocarditis. 3 Cardiac work-up constitutes a cornerstone for tailoring the optimal secondary stroke prevention strategy. 2,4 In many circumstances, ischemic stroke can be considered the complication of cardiac disease.
On the other hand, it is less widespread knowledge that stroke may harm the heart. Following stroke, one may observe myocardial injury, acute coronary events, left ventricular dysfunction, and arrhythmias. These cardiac complications following acute ischemic stroke (AIS) have been termed “stroke–heart syndrome.” The stroke–heart syndrome has recently attracted much attention and put a spotlight back on a long-lasting history of mutual involvement of heart and brain. 5,6 This narrative review gives an overview on myocardial injury after AIS.
History
The interaction between heart and brain looks back on a history of millenniums. About 300 B.C., the antique Greek philosopher Aristotle and his followers had propagated a powerful cardiocentric theory: This teaching was based on the assumption that the origins of consciousness, motion, and sensation were located in the heart. In opposition to this, Galen, a Greek physician practicing during the second century of our era in Rome, suggested a brain-centered understanding of neuropsychiatric symptoms. The dispute was negotiated throughout the middle ages. Scholastic physicians and philosophers tried to solve this brain–heart dispute. They tried to reconcile two great minds with each other. The conclusion was that stroke would begin in the brain but would terminate in the heart. 7,8
The perception of acute stroke beginning in the brain and terminating in the heart seems strikingly modern, if we have a look at recent research. Growing evidence supports the notion that stroke can cause damage to the heart. 5,6,9
Myocardial injury after AIS
In the diagnostic work-up of ischemic stroke, cardiac diagnostic forms a cornerstone. 1,2 Cardiac diagnostic is essential to clarify stroke etiology and the optimal prevention strategy of stroke recurrence. In addition to prevention of recurrence, therapy strives to prevent other complications like myocardial infarction and deaths. One in five deaths in stroke patients has a cardiovascular cause. Cardiovascular deaths are only the tip of the iceberg, as stroke is related to an increased risk of nonfatal cardiac complications including acute coronary syndrome (ACS), arrhythmias, and ventricular dysfunction (takotsubo syndrome is an example). 5,6,10 The most serious complications after AIS occur in the acute phase. 11,12 The risk to experience severe cardiac complications like takotsubo syndrome is proportional to the severity of the neurological deficit. 5,13
Cardiac troponin
An easy way to assess and quantify myocardial injury is the measurement of cardiac troponin (cTn). cTn may indicate cardiac complications at an early stage. cTn is highly specific to cardiomyocytes injury and allows to quantify myocardial injury. 14,15 Measuring cTn also conforms to the current guidelines on early management of patients with AIS. The guidelines advocate cTn assessment with a class one level of recommendation that is based on sound meta-analyses of observational data showing its predictive power. 16 The recommendation is also strong, because timely identification of cardiac disease may prompt additional diagnostic tests and this, in turn, may lead to adjusted therapy and finally improves outcomes. 6 The proportion of AIS patients exhibiting cTn elevation will depend on the assay applied. If up-to-date, high-sensitivity assays are in use, elevated cTn will be detectable in about 30–60% of stroke patients. 17,18 Elevated cTn in AIS is more common in older patients. However, the prevalence of 30–60% is much higher than would be expected from populations of elderly individuals without acute stroke. 6,19 Besides, cTn elevation in AIS goes along with higher stroke severity, known coronary heart disease, and impaired kidney function indicating comorbidities and worse premorbid status. In the vast majority of patients with cerebrovascular events, cTn elevation occurs in the absence of typical clinical coronary symptoms (e.g. chest pain and dyspnea). 20 In contrast to the very frequent finding of cTn elevation in AIS, only 10% of AIS patients will exhibit left ventricular dysfunction. If left ventricular dysfunction is present, they are strongly associated with elevated cTn. 21 In contrast, up to 70–90% show pathological electrocardiogram (ECG) findings. 22,23 The most frequent ECG findings are repolarization changes and most of these ECG alterations are transient and peak early after stroke. 24 Importantly, although transient, ECG alterations identify individuals at risk for clinically relevant arrhythmias 25 and have—in part—been linked to cTn elevation. 26,27
Prognosis
Cardiac cTn elevation indicates worse prognosis in AIS at several aspects. First, elevated cardiac cTn is associated with worse prognosis including higher inhospital mortality. The association between elevated cTn and higher mortality in stroke patients remains robust after 3, 12, and even up to 24 months after the event. 18,28 With respect to prognosis, adding high-sensitivity cTn (hs-cTn) to established scores improved the precision of prediction. 29 Further, in patients with embolic stroke of undetermined source, elevated cTn was associated with an increased risk for cardiovascular events. 30 Moreover, elevated hs-cTn was linked with more severe matter lesions of the brain, suggesting silent brain infarction as one possible link. 31 This silent brain damage of the white matter may well go along with dementia. This notion is supported by an analysis of the Prospective Cohort With Incident Stroke cohort that found higher hs-cTn levels to be associated with higher prevalence of cognitive impairment at the time of a first-ever ischemic stroke and indicated lower cognitive status during 3-year follow-up. 32
Potential mechanisms
In the acute phase, physicians may be wary not to miss acute myocardial infarction (AMI). The higher the levels of cTn and their dynamic rise or fall pattern, the greater the odds that the cause is an AMI. 6,33 AMI would typically be accompanied by a dynamic change of cTn of greater than 20%, new ischemic ECG changes, imaging evidence of new loss of viable myocardium or new regional wall motion abnormalities, and identification of a coronary lesion. 33 A case illustration is given in Figure 1.

Illustrating case.
However, in two-thirds of AIS patients with elevated cTn, serial measurements showed no relevant temporal change in cTn levels. 34 Although myocardial injury is a prerequisite for the diagnosis of myocardial infarction, it is also an entity of itself. Elevated cTn without dynamic change may indicate myocardial injury due to cardiac conditions on the one hand (including myocarditis, heart failure, ventricular tachyarrhythmia, or cardiac procedures like coronary revascularization, ablation, and defibrillation) but may be associated with noncardiac conditions such as renal failure, severe anemia, or respiratory failure, on the other. 33 An overview of potential reasons for elevated cTn is given in Table 1.
Reasons for elevated cTn indicating myocardial injury. 33
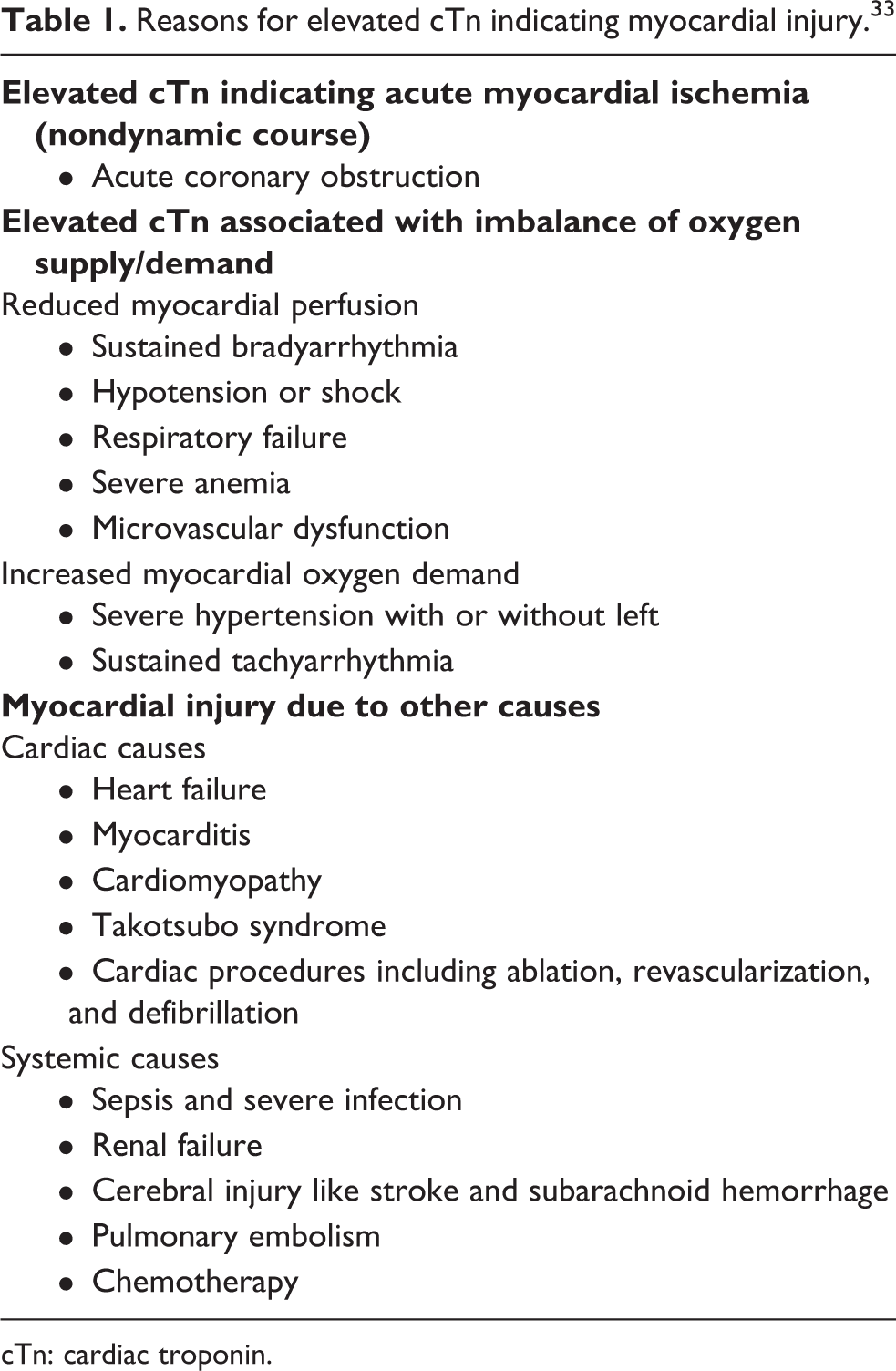
cTn: cardiac troponin.
Echocardiographic findings like akinetic left ventricular wall were not present in the majority of AIS patients. 35 Proof of severe coronary lesions (namely “culprit lesions”) was not found in about three of four AIS patients with elevated cTn. 36 Therefore, AMI will be the explanation in a minority of AIS patients with cTn elevation only, and more research is warranted to identify those AIS patients in need of immediate coronary imaging as well as to understand alternative explanations of myocardial injury in AIS. Ongoing research will help to identify those patients in need of extended and possibly invasive diagnostics. 37
The alternative underlying mechanisms of cTn elevation in the context of AIS are still poorly understood. In a first step, stroke-associated myocardial injury may be differentiated between those AIS patients with and without underlying heart disease. 5,6,18 Both ischemic (i.e. ACS) and nonischemic cardiac damage may lead to myocardial injury in stroke patients.
One main nonischemic mediator (no coronary artery obstruction) would be autonomic dysregulation as the heart receives input from the central autonomic system that will change heart rate and contractibility. 5,6,38
The role of central autonomic dysregulation is supported by imaging studies. By using voxel-based lesion-symptom mapping, Krause et al. demonstrated that (1) the relative changes of elevated hs-cTn are significantly associated with AIS lesions in the right-sided cerebral insular cortex and (2) in contrast, the absolute (or baseline) hs-cTn values acquired on admission did not show any relation to stroke lesion location within the anterior circulation. 39 The insular cortex is regarded as an essential part of autonomic regulation, particularly with respect to cardiac control. 40,41 It has also been proposed that insular damage might contribute to sudden cardiac death after stroke. 42 Insular strokes were linked to decreased heart rate variability 43 and arrhythmias like incident atrial fibrillation. 27,44 In a selective insular AIS rat model, the most prominent myocardial changes were found in the region of the atrial myocardium with the highest density of sympathetic nerve endings. 45 These observations argue in favor of dysregulated autonomic cardiac control.
Mediation is not restricted to nervous autonomic control. The neuroendocrine hypothalamic–pituitary–adrenal Axis (HPA) employing humoral pathways is involved. In addition to elevated cTn levels, a release of serum catecholamines has been observed in stroke patients. These elevated stress hormone levels have been correlated with stroke severity and extent of insular damage. Both elevated serum catecholamine and serum cortisol levels express involvement of the HPA. 46 Indeed, stimulation of the hypothalamus activates sympathetic output and may induce electrocardiographic abnormalities, arrhythmias, and even myocardial necrosis. 47 Experimental animal studies have demonstrated an increase in serum catecholamine levels after ischemic stroke that was directly proportional to the incidence of cardiac damage. 48 Systematic release of catecholamines from the adrenal glands is promoted via direct autonomic sympathetic stimulation and via the humoral hormones inherit to the HPA axis. This constitutes the basis for the catecholamine surge hypothesis. 49
The cardiac injury may be exacerbated by local and systemic inflammatory responses due to stroke. Cytokines are released acutely after stroke within the brain. Bone marrow and spleen inflammatory coupling lead to systemic inflammation. Release of interleukin-1, monocytes, and neutrophils and activation of caspase-1 complex as well as systemic release of catecholamines from the adrenal glands all contribute to myocardial injury. 49 Increased sympathetic tone enhances the splenic inflammatory response further. The mechanisms enhance one another. 6 Figure 2 displays mechanisms of stroke-induced myocardial injury.

Myocardial injury may be mediated via three major entities.
Diagnostic implications
While cTn measurement is advised by guidelines to prompt further cardiac investigations, these guidelines remain vague with respect to diagnostic and therapeutic consequences in patients. Identifying AIS patients at high risk for coronary events may be a prerequisite for better prevention strategies in the future. 37,50 Elevated baseline cardiac cTn is associated with higher stroke severity, higher creatinine, ST-segment depression, and inverted T waves, but none of the factors was helpful to differentiate myocardial infarction from autonomic cardiac dysregulation. 51 Ancillary investigations may be needed to solve the differential diagnosis. Coronary angiography remains the gold standard to diagnose extend and severity of coronary artery disease. Besides, coronary angiography offers the opportunity for invasive treatment. However, the 2020 European Society of Cardiology guidelines for the management of ACS consider coronary computed tomography angiography an alternative to invasive angiography to exclude ACS when there is a low-to-intermediate likelihood of coronary artery disease and when cardiac cTn elevation and/or dynamic are inconclusive. 52 A detailed recommendation on how to apply and interpret cTn elevation in the context of AIS and when to use ECG, echocardiogram and coronary angiography have been published recently. 6,18,53 A possible workflow is displayed in Figure 3.

Proposed workflow in patients with ischemic stroke and elevated cardiac troponin.
Apart from long-established diagnostics like ECG and echocardiogram, noninvasive cardiac magnetic resonance imaging (MRI) may provide helpful information to identify stroke patients with or without ACS. Cardiovascular MRI (CMR) was proven feasible in stroke patients and allowed identification of systolic and diastolic dysfunction. 54 Including contrast agent-based sequences, CMR enables to detect late gadolinium enhancement (LGE). CMR allows excellent tissue characterization and may identify and differentiate vital myocardium, scaring (LGE), nonischemic diffuse fibrosis (via T1 mapping), and edema (T2 mapping)/extracellular volume fraction (%). 55 Therefore, one can distinguish lesions consistent with myocardial infarction from nonischemic lesions. 55,56 CMR was also used in a subgroup of patients within the TRELAS study which had quantified frequency of severe coronary lesions (so-called culprit lesions) on coronary angiogram in AIS patients with troponin elevation by assessors blinded to clinical information. 36 In this subgroup, patients who showed transmural LGE on CMR all had corresponding culprit lesions diagnosed on their coronary angiograms while no patient without transmural LGE had. 57 Absence of MRI-detected LGE may well indicate the absence of culprit lesions or significant coronary artery disease by coronary angiography. Of note, CMR may add important information on stroke mechanisms including embolic heart infarcts and amyloidosis. 55,58
Both CMR and coronary computed tomography angiography will help to differentiate between ischemic and nonischemic myocardial injury in the future. Further data are needed to establish the optimal diagnostic algorithm. The PRediction of Acute Coronary Syndrome in Acute Ischemic StrokE Study has just managed to recruit the preplanned sample size of patients and results may be expected with excitement. 37 In addition, the ongoing Cardiomyocyte Injury Following Acute Ischemic Stroke (CORONA-IS; clinicaltrials.gov NCT03892226) 59 and “Bern Heart and Brain Interaction Study” (clinicaltrials.gov NCT03720522) will produce valuable data on the diagnostic capacity of CMR.
New data will improve knowledge on the long-lasting interaction between heart and brain. Myocardial injury after acute ischemic stroke and stroke–heart syndrome are now a thriving research topic. The causative mechanisms of stroke-related dysfunction may become attractive new targets for future therapeutic strategies.
Footnotes
Author contributions
CHN drafted the manuscript. ME and JFS made substantial intellectual contributions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.