
Abstract
Dilated Virchow–Robin spaces (VRSs) are expansions of the normal perivascular spaces with a short axis greater than 2 mm or, according to some authors, greater than 3 mm. They are usually documented at the basal ganglia, at the convexity white matter (WM) and centrum semiovale, and at the mesencephalon. The anterior temporal WM is a recently described preferential location for large (≥5 mm) VRSs. The aim of our study was to evaluate the magnetic resonance imaging (MRI) features and their modifications during a long-term follow-up period (≥24 months) of the anterior temporal VRSs with a retrospective analysis among all brain MRI studies performed at our institution between January 2010 and January 2017. In our study, the presence and the stability of characteristic MRI features certainly increased our diagnostic confidence allowing us to continue conservative approach while the surrounding signal change, as reported in the literature, should not in itself prompt alternative diagnoses to be entertained.
Introduction
Dilated Virchow–Robin spaces (VRSs) are expansions of the normal perivascular spaces having short axis greater than 2 mm or, according to some authors, greater than 3 mm. 1 –5 Normal VRSs are pial-lined spaces surrounding penetrating cerebral vessels as they course from the subarachnoid compartment into the brain parenchyma and represent physiological findings that can be identified on high-resolution magnetic resonance imaging (MRI) studies in healthy patients of all ages theoretically present in 100% of subjects. 1,2,6 –8 VRSs may have very large size (>1.5 cm) with mass effect and consequent changes in cerebrospinal fluid (CSF) dynamics and pose an important diagnostic challenge in the differentiation with cystic benign or malignant lesions of the brain parenchyma. 9,10
Previous literature described three preferential different locations for dilated VRSs: most frequently at the basal ganglia along the pathway of the lenticulostriate vessels that enter via the anterior perforated substance, at the convexity white matter (WM) and centrum semiovale along the pathway of the perforating medullary vessels, and at the mesencephalon along the pathway of the perforating collicular vessels. 2,3,6,11 –13 However, while small VRSs are not uncommonly noted in the subcortical WM of the anterior temporal lobe, the anterior temporal WM is a recently described preferential location for large (≥5 mm) VRSs with 59 cases published in the literature up today, all of them showing similar imaging features. 6,10,14,15
The aim of this retrospective study was to evaluate the evolution of MRI features described in the recent literature of large VRSs located in the subcortical WM of the anterior temporal lobe during a long-term (≥24 months) follow-up.
Materials and methods
Case selection
Given its retrospective design, this study did not require a formal institutional research ethics board approval. All patients were informed that images of their MRI studies could have been used for clinical research and they gave written consent to imaging examination.
Among all brain MRI studies performed at our institution between January 2010 and January 2017 were retrospectively researched patients showing large VRSs (smallest internal diameter ≥5 mm) within the anterior temporal WM having at least two MRI examinations distant ≥24 months.
The patient clinical and imaging records were retrospectively reviewed to obtain patient demographic data, clinical symptoms prompting initial imaging, diagnosis stated on the original radiologist’s report and any further imaging evaluation and subsequent development of neurologic symptoms were also noted.
Imaging acquisition and analysis
MR examinations were performed on a 1.5 T system (Avanto, Siemens Healthcare Sector, Erlangen, Germany) and/or on a 3 T system (Sygna, General Electric HDXT, Milwaukee, Wisconsin, USA). Following performed sequences were reviewed if available: T1-weighted (w), T2-w, fluid-attenuated inversion recovery (FLAIR), diffusion-weighted imaging (DWI), gradient-recalled echo (GRE), variable flip-angle 3-D TSE T2-w, time of flight (TOF) angio-MR, high-resolution 3-D T1-w fast-field-echo and gadolinium-enhanced imaging.
MR images were analyzed in double-blind fashion by two-expert neuroradiologists and any discrepancies were resolved in consensus. The following imaging features of VRS were evaluated: shape, minimum and maximum diameter on T2-w sequences, signal characteristics on T1-w, T2-w, FLAIR-w, DWI-w, GRE-T2*-w sequences, contrast enhancement (CE) after intravenous paramagnetic contrast medium administration, middle cerebral artery (MCA) branches vascular contact, morph-dimensional modifications of adjacent cortical contour, WM signal perilesional changes, presence of close both liquor intensity tract or smaller VRS. 6,10 According to Lim et al., WM signal perilesional change was classified as mild, moderate, or extensive: mild, if there was only a thin rim, moderate for a larger focal area incompletely surrounding the lesion, and extensive if there was a diffuse abnormality surrounding the lesion. 6
Any morphological, signal, or dimensional modifications on MRI studies during follow-up period were recorded.
Results
Among about 2940 MRI brain examinations, six large VRSs of the anterior temporal WM in five patients were retrospectively identified (four females and one male; mean age 55 years, range 37–63 years), which were followed-up for ≥24 months after the initial finding (Table 1). In most (4/5) patients, there were no clinical symptoms that could be directly referable to the lesion: one patient complained progressive concentration and memory deficit (patient A in Table 1), one patient was affected by multiple sclerosis and suffered from upper limb paresthesia (patient B in Table 1), 16 one patient complained migraine (patient C in Table 1), and one patient suffered from episodes of vertigo and dizziness (patient E in Table 1).
Any morphological, signal, or dimensional modifications on MRI studies during follow-up period.

MRI: magnetic resonance imaging; CSF: cerebrospinal fluid.
Only one patient (patient D in Table 1) with recent episodes of epilepsy presented symptoms that could be related to the lesion which was initially suspected to represent a tumor on unenhanced CT scan (Figure 1). Overall, in the other three of five cases, MRI findings were stated as VRSs on the initial radiological report, while in the remaining case, the radiological report included VRS as a possible diagnosis. The range of differential diagnoses in initial reports included low-grade glioma, ganglioglioma, neuroepithelial cyst, old trauma/infarct, gliotic changes of microvascular origin. 6,10

Axial unenhanced CT scan (patient D) shows the presence of an intraparenchymal expansive lesion in the right temporal lobe, with cystic component and surrounding hypodensity, suspected for a tumor. CT: computed tomography.
The mean follow-up time was 35.4 months (range 24–74 months) (Table 1). Mean short axis size was 8.49 mm (range 5–10.5 mm) while mean maximum diameter was 12.74 mm (range 0.81–18–8 mm) (Table 1). VRSs appeared mostly oval-shaped (3/5), in one case the lesion had roundish morphology while in the remaining case the lesion appeared bilobed (Table 1; Figure 2). All lesions had internal signal characteristics identical to CSF in all sequences performed without showing restricted diffusion neither CE. In two of five patients was observed extensive perilesional T2-w/FLAIR hyperintensity without relationship between the size of the VRS to presence or severity of perilesional signal (patients C, D, Table 1; Figure 3).
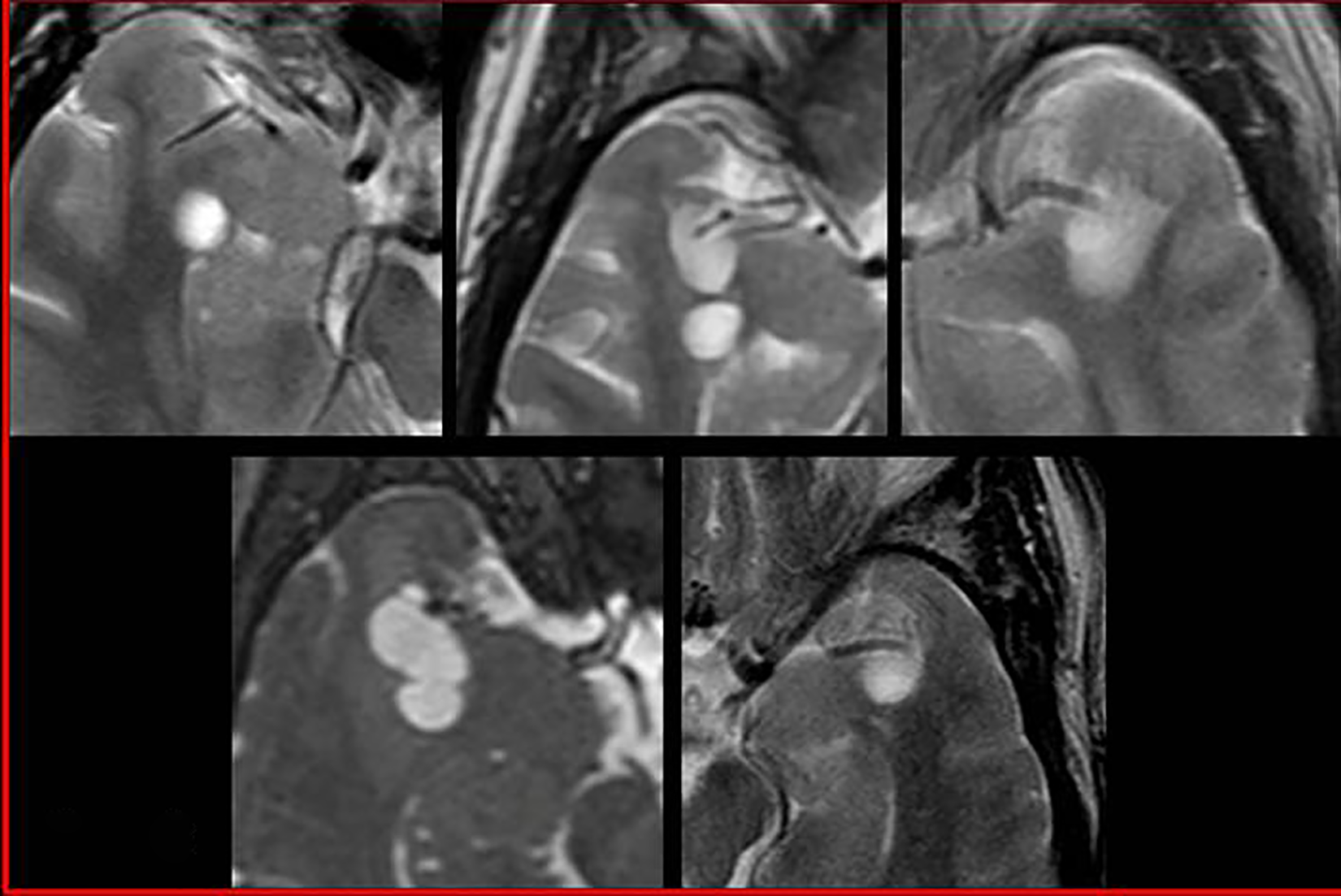
Axial T2-weighted MR images show the morphology of dilated perivascular spaces in five patients; letters refer to corresponding patients in Table 1. Notice the linear sign in patients B, C, and E due to traversing vessel. MR: magnetic resonance.

Axial FLAIR MR images show extensive perilesional hyperintensity in patient C (A) and D (B). FLAIR: fluid-attenuated inversion recovery; MR: magnetic resonance.
Angio-TOF images allowed to better recognize a branch of MCA in contact with VRS (Figure 4), and in three of them, it was associated to focal cortical distortion or thinning (patients B, C, D in Table 1 and Figure 4).

Axial TOF-MR images show vascular structures adjacent to the dilated perivascular spaces, better evident in B, C, E; sagittal (B) and coronal (C, D) T2-weighted images in the corner reveal the associated cortical indentation in patients B, C, and D. Letters refer to corresponding patients in Table 1. TOF: time of flight; MR: magnetic resonance.
In our sample, four patients had smaller adjacent VRSs (patients A, C, D, E in Table 1 and Figure 5) while in one patients two close dilated VRSs were found (patient B, Table 1; Figures 2 and 5). Contiguous CSF intensity tract was identified in three cases (patients B, C, E, Table 1; Figure 6, Figure 7).
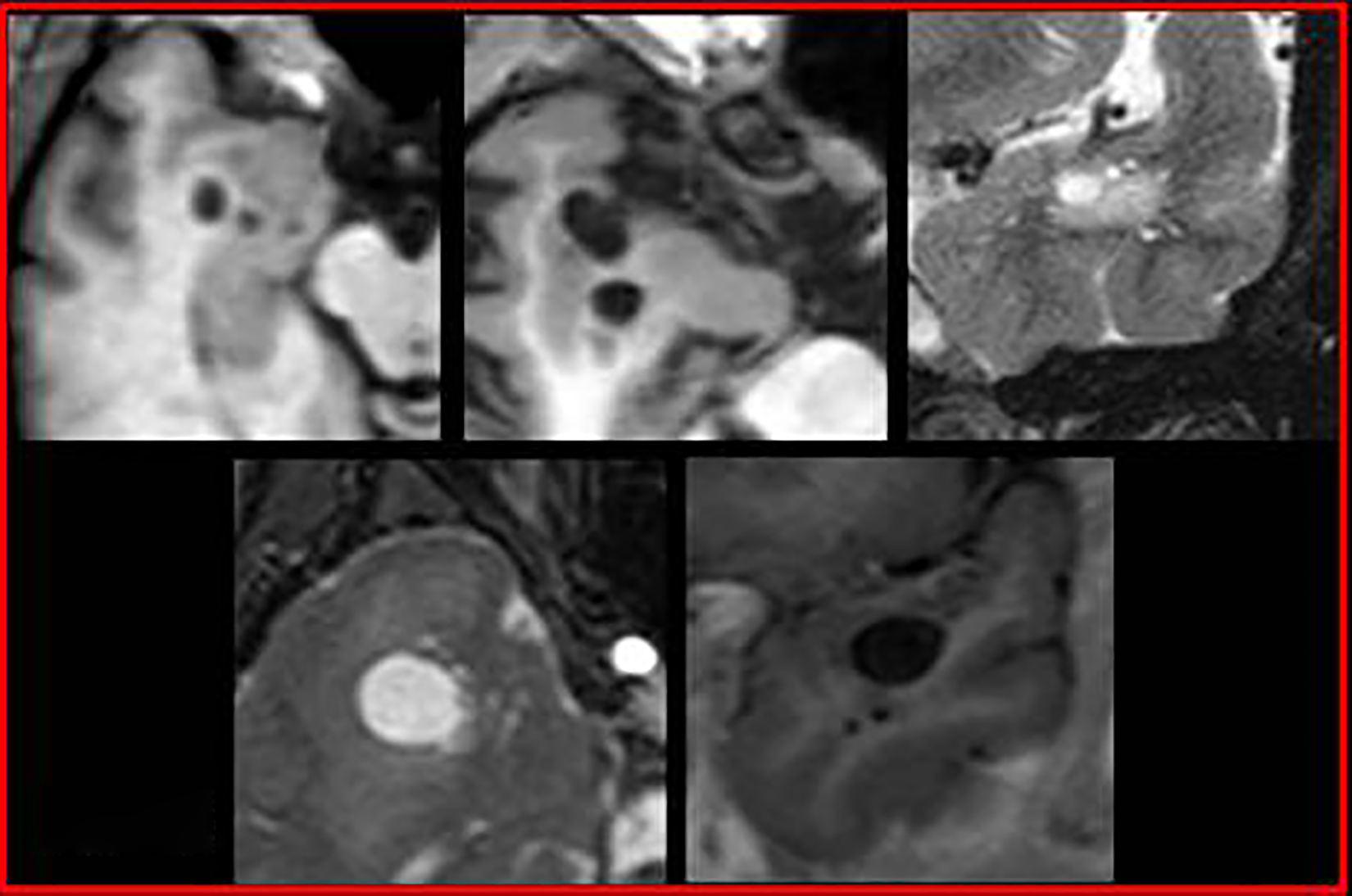
Axial (A, B) and coronal (E) T1-weighted MRI images and coronal (C) and axial (D) T2-weighted MRI images reveal the presence of smaller adjacent perivascular spaces in patients A, C–E; letters refer to corresponding patients in Table 1. MRI: magnetic resonance imaging.

Coronal FLAIR images show the presence of linear tract isointense to liquor in patient B (A), C (B), and E (C). FLAIR: fluid-attenuated inversion recovery.

MRI spectroscopy evaluation revealed no Cho peak increase of the lesion (A); reference normal parenchyma (B). MRI: magnetic resonance imaging.
No variations of MRI morph-dimensional and signal features were observed during the follow-up period (Figure 8).

T2-weighted images show the stability of the lesion throughout the longest MRI follow-up period (74 months). MRI: magnetic resonance imaging.
Discussion
Previous literature on dilated VRSs demonstrated their tendency to typically involve the inferior basal ganglia along the anterior commissure. 10 Although less common, dilated VRSs have been reported to exist focally elsewhere in the brain parenchyma, including the subcortical WM. 10 Among subcortical locations, the large anterior temporal WM has been recently described as a site for large VRSs where, in association to the presence of perilesional T2-w/FLAIR signal, they can be misdiagnosed with cystic tumors. 6 In agreement with results of Lim et al., we observed that large VRSs in the anterior temporal lobes showed a predilection for women. 6 To date, about 59 cases of dilated VRSs located in the subcortical WM of the anterior temporal lobe have been described in the literature, the majority (73%) with increased perilesional FLAIR signal. 6,10,14,15
In our study, perilesional T2-w/FLAIR hyperintensity was noted in four of five (80%) patients according to that reported by Lim et al., Rawal et al. and Cerase et al. who observed perilesional signal alterations in the majority of cases. 6,10,14 However, in our cohort, two of five patients had extensive perilesional T2-w/FLAIR signal change, which is a higher result to those reported by Lim et al. (11/39) and Rawal et al. (1/15). 6,10 In one case (patient D in Table 1), the extensive perilesional T2-w/FLAIR high signal was associated to bilobed shape and clinical presentation with seizures so it was initially misdiagnosed for cystic neoplastic lesion (Figures 1, 2(D), 3(B), 4(D), 5(D)). Further MR spectroscopy evaluation revealed no increase of choline peak and the stability of MR features over the time confirmed the benign nature; the presence of typical MRI features for large VRS—discussed below—suggested the final diagnosis.
Both cases with increased perilesional T2-w/FLAIR signal did not exhibit sustained growth during imaging surveillance, making low-grade glioma extremely unlikely. 6 The cause of surrounding T2-w/FLAIR signal change is uncertain with postulates including accelerated WM ischemic change resulting from compression of the adjacent parenchymal vessels by the enlarged perivascular space or chronic mechanical stress from high blood pressure on the brain arterioles. Another theory, however, is that the high signal may be the result of gliosis in addition to multiple smaller perivascular spaces that can be revealed only with pathologic specimen. 6,10
Smaller adjacent VRSs have been suggested as a potential MR feature of anterior temporal VRSs. 6 In our study, we were able to identify smaller perivascular spaces surrounding the dominant lesion in four patients (Figure 5), while in the remaining patient they were not recognized probably because they were too small to be resolved by the MR imaging technique despite the use of 3-D T2-w sequence which is reported to allow a better visualization of smaller VRSs compared to FLAIR imaging. 6,16
Recently, it has been reported in the literature that VRSs may be a marker of neurodegeneration or cognitive decline in patients with multiple sclerosis and that these patients have significantly more and greater VRSs than healthy subjects with a marked increase for atypical locations such as observed for one of our patients (patient B in Table 1). 17 –19
While the majority of large anterior temporal VR spaces remain stable, an occasional change in the extent of perilesional FLAIR signal, increase or decrease in size may occur. 6 Modification of the extent of perilesional T2-w/FLAIR hyperintensity was observed by Lim et al. who reported that 5/22 patients demonstrated change in perilesional signal or overall size during MR follow-up (mean 24 months; range 4–100); one case, with 4 years of serial MR imaging, developed new perilesional FLAIR signal which later regressed and was replaced by smaller VRS with overall increase in size of the large VR space. 6,10,14 This progression of perilesional FLAIR signal over time in that patient was explained by development and coalescence of tiny surrounding VRSs that were too small to be resolved by the initial MR imaging technique. Lim et al. postulated that alteration in perilesional signal and size was related to reversible mechanical obstruction or altered CSF flow dynamics. 6 In our cohort, no change in size was noted in any patient on serial MR imaging follow-up (mean 36 months; range 24–74), either involving the lesion itself or the degree of perilesional signal hyperintensity according to the results of Rawal et al. in nine patients during the follow-up period (mean 38 months; range 6–112 months) for both VRS size and surrounding signal change. 10 On the contrary, few rare cases of dilated VRSs that regressed with time have been described and explained by reversible mechanical alteration of flow dynamics. 14,20
VRSs have two histologic components—a vessel traversing the brain from the pia and a fluid-filled space surrounding the vessel—and the recently described characteristic linear sign was observed in our patients on T2 and TOF images indicating the presence of traversing vessel of dilated VRS. 6,21 It was clearly depicted in three patients (patients B, C, E, Table 1; Figures 2 and 4) and less evident in the other two patients. However, it is reported that not all of VRS had flow-related enhancement, especially on 1.5 T MRI scan, because some arteries within VRSs might be too fine to be detected in current MR images or because a VRS is traversed by a vein that cannot be visualized due to the saturation pulse for cephalocaudal flow. 21
The characteristic linear sign represented by the traversing vessel, in three our patients was observed (Figure 4(B) to (D). It is reported that in some patients, tortuous arterial branches may cause focal distortion of the overlying cortex that may in turn obstruct small tracts traversed by perforating vessels that connect the perivascular and subarachnoid spaces 7 ; this mechanical obstruction could result in secondary dilation of the VRS. 6
Histological studies have identified penetrating vessel passing along pial-lined canals from the subarachnoid space to dilated VRS in some patient can be identified a clear CSF intensity tract either leading from the subarachnoid space to the large VRS or extending posteriorly toward the temporal horn. 6 According to this, in our cohort, CSF intensity tract was identified in three patients.
Our study has several limitations. Fist of all, no patient had histopathological correlation. Nonetheless, all cases had identical internal MR imaging signal characteristics and were similar in location and morphology except for one case which differed having bilobed shape. Moreover, characteristic linear sign represented by the traversing vessel was observed in all cases. Further limitations are related to the retrospective nature of the study with heterogeneity in MR scanners and study protocols and mainly to the small sample size; however, in literature are described only 20 cases having a follow-up ≥24 months. 6,10,14,15
Conclusion
Large anterior temporal lobe WM, in agreement with the results of other authors, may represent a newly identified preferential location for dilated VRSs 6,10,14 ; they commonly demonstrate perilesional T2 or FLAIR signal and can be misdiagnosed as cystic tumor. Accurate prospective recognition of dilated VRS as benign “do-not-touch” abnormalities will avoid unnecessary invasive treatment. In our study, despite perilesional FLAIR/T2 hyperintensity, the presence and the stability of characteristic MR imaging features certainly increased our diagnostic confidence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.