
Abstract
Cervicogenic headache (CH) is a syndrome which is postulated to originate from nociceptive structures in the neck or head. The anatomical neck or head structures that are responsible for the pain in CH have not been clearly identified, but the pain in these patients probably originates from the structures of the cervical spine. In this study, cervical MRI were studied in 22 patients with cervicogenic headache and 20 control patients who did not have any disease which may effect the bone and muscle structures of cervical region. MRI imaging of cervical vertebra showed a disc bulging in 10 (45.4%) out of 22 patients with CH and in 9 (45.0%) of 20 controls (P > 0.05). The distribution of pathological lesions in patients and controls were not significantly different (P > 0.05). As a result, MRI may not be an adequate method to detect pathological findings underlying the aetiology of CH such as nerve roots, intervertebral joints and periosteum.
Introduction
Cervicogenic headache (CH) is a clinically described syndrome that presents as recurrent or continous unilateral headache without side shift (1–3).
The anatomical neck or head structures that are responsible for the pain in CH have not been clearly clarified, but the pain in these patients probably originates from nerve roots, uncovertebral joints, intervertebral joints, muscle, nerves, ganglions and ligaments (3–6).
Symptoms and signs in patients with CH are generally referable to cervical spine (3, 7). The upper part of cervical spine seems to be major important part, but it was suggested that headache may also originate from structures in the lower cervical spine (7, 8).
In this study, our aim was to evaluate cervical structures in patients with CH using magnetic resonance imaging (MRI).
Patients and methods
Cervical MRI were performed in 22 patients with cervicogenic headache and in image studies MRI analysis was performed blindly. The radiologist had no information concerning the clinical symptoms of patients. All patients fullfilled the diagnostic criteria which were described by Sjaastad et al. (3) (Table 1). Blockage with 0.5–1 ml of lidocaine was applied to the region 2 cm lateral and 2 cm inferior of the protuberencia occipitalis externa to confirm the diagnosis and patients whose pain was relieved by more than 50% were confirmed with the diagnosis of CH.
Diagnostic criteria of cervicogenic headache (3)

Twenty patients, without any disease which could have an effect on the bone and muscle structures of cervical region, were included in the control group. Characteristics of patients in control group are shown in Table 2. There was no difference between patients with CH and control group in the terms of age and gender (Table 3). Informed consent were obtained from all patients.
Characteristics of patients in control group
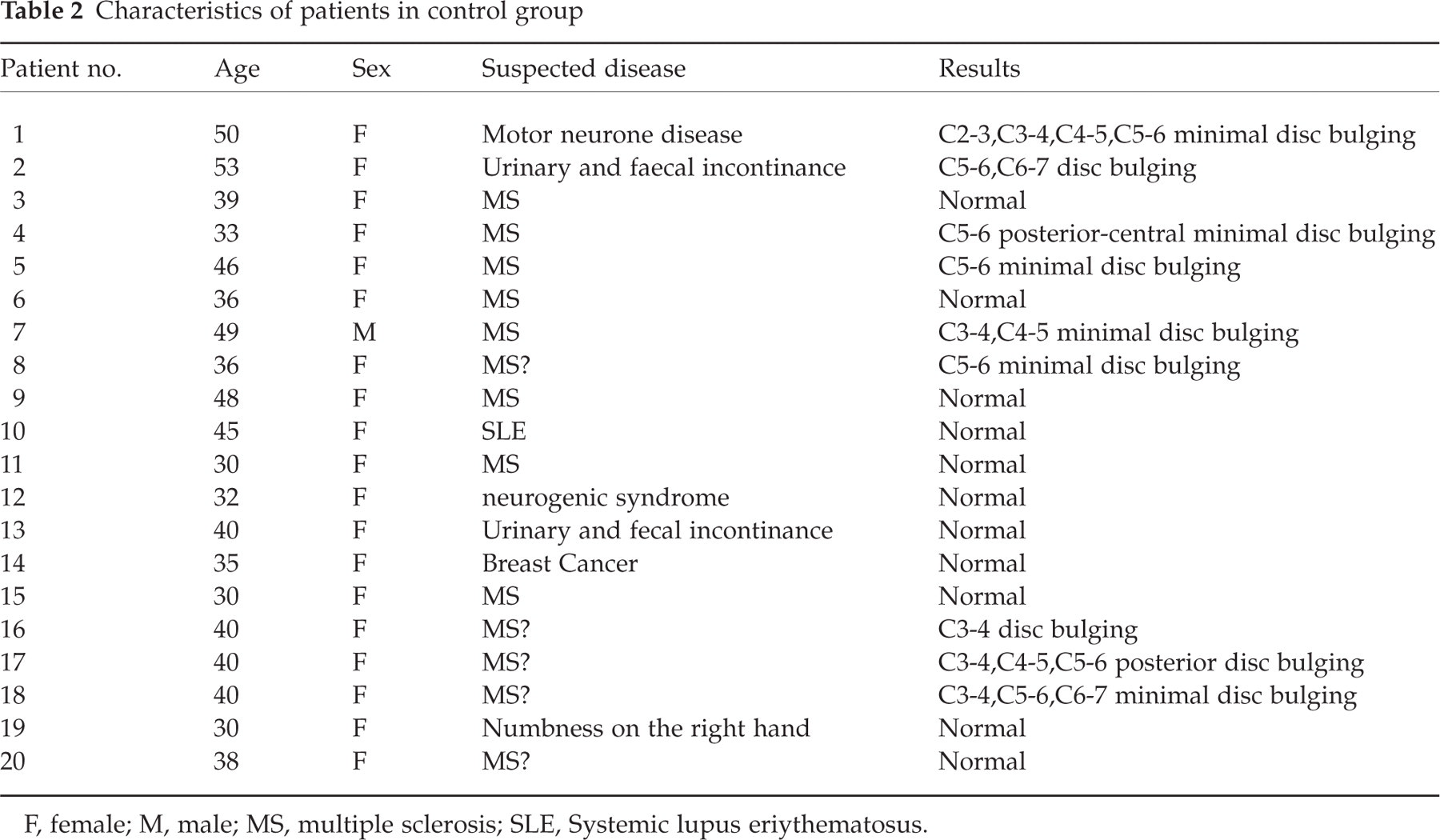
F, female; M, male; MS, multiple sclerosis; SLE, Systemic lupus eriythematosus.
Pathological findings of patients and control subjects

All patients had minimal disc bulging in their intervertebral space.
Mann–Whitney U-test, Fisher's χ2 test and Pearson correlation analysis were used for statistical analysis. P-values < 0.05 were considered significant.
Results
MRI imaging of cervical vertebra showed a disc bulging in 10 of 22 (45.4%) patients with CH and in 9 of 20 (45.0%) controls (P > 0.05).
In patients with CH, there was no pathology in C2-3, and C7-8 vertebrae. The pathology was found in C3-4 vertebra of two, in C4-5 vertebra of 8, in C5-6 vertebra of 11 and in C6-7 vertebra of 3 patients.
In control group, there was no pathology in C7-8 vertebras. The pathology were found in C2-3 vertebra of one, in C3-4 vertebra of 5, in C4-5 vertebra of 3, in C5-6 of 7 and in C6-7 of 2 patients. The dis-tribution of pathological lesions of patients and controls were not different as shown in Table 3 (P > 0.05).
There was a history of neck trauma in two patients (9%), but neither of them was a whiplash injury. No patient had suffered a neck trauma in the control group.
Discussion
CH is a syndrome characterized by intermittent or continous unilateral headache without sideshift (1, 3). Although some patients with CH may present with bilateral headache, detailed history often indicate that intensty of the pain predominates on one side (9).
The diagnostic criteria of CH were reported in 1990 by Sjaastad et al. (3). Firstly, response to diagnostic nerve blocks were not included in these criteria, however, in 1998, the use of diagnostic nerve blocks was added to these criteria (5). In our study, all patients had a positive response to a diagnostic nerve block to confirm the diagnosis of CH in addition to having fullfilled the diagnostic criteria described by Sjaastad et al. (3).
Although the pathogenesis of CH is not clear at the present time, it is generally thought that CH may originate from various structures in the neck (3). The anatomical neck structures that are responsible for both the local and referred pain in CH have not been clearly described (4, 5). However, CH has been suggested to be closely related to the cervical spine (10). The pain sensitive structures in the cervical spine include nerve roots, muscles intervertebral joints and parts of the vertebral column (11).
Radiological findings of 15 patients with CH were investigated by Pfafferath et al. (12) and cervical X-rays and functional radiograms showed no difference between patients and control subjects. However, Fredrikten et al. (13) showed slightly increased insidence of degenerative changes of inferior cervical region in patients with CH than control subjects by using cervical X-rays and tomographies with the lack of statistical significance. Vincent et al. (14) showed no significant change on MRI scans of the cervical spine in patients with CH. In the present study, 10 (45.4%) patients had a disc bulging on MRI but this was not found to be statistically significant when compared to the control subjects (45.0%) (P > 0.05) and there was no other pathological finding associated with CH on MRI studies. This suggests that MRI does not have an important role in detecting the pathological conditions of cervical structures which lead to CH. In this study, we selected patients who did not have any disease which may effect the bone and muscle structures of cervical region as the control group. Some cervical pathologies could accompany the suspected disease in our control group, but no association between symptoms and cervical lesions were found. We could also have used healthy volunteers as a control group but, due to economic considerations, they were not included in the control group.
It has been suggested that CH mainly orignates from the structures innervated by upper cervical nerve roots (11, 12). However, relief from CH was observed in some patients after an operation to the C6-7 spine which indicates the involvement of the lower cervical part in the aetiology of CH (11). In our study, MRI findings were not different between upper and lower parts of cervical spine in patients with CH.
CH shows a female predominance and trauma may precede the onset of the disease (9). It has been suggested that the mechanism underlying CH vary with age. Older patients could experience the syndrome because of degenerative disorders while in younger patients CH could be linked to trauma or other predisposing factors (9). In our study, there was a history of neck trauma in two (9%) patients, but none of them was a whiplash injury. No patient had suffered a neck trauma in control group.
In conclusion, pathological findings of cervical MRI were not different in patients with CH compared to those in control subjects. MRI may not be an adequate method to detect the pathological findings underlying the aetiology of CH such as nerve roots, intervertebral joints and periosteum.