
Abstract
In great part due to recent advances in medical technology, ischemic cerebral stroke has become an increasingly treatable condition, which requires urgent measures and which rely on pharmacological and/or interventional measures. Due to its high prevalence, preventive measures should also be undertaken, and this is a situation where the use of advanced neuroimaging techniques could be helpful in certain underlying diseases. What is proposed here is to discuss how modern neuroimaging techniques (advanced magnetic resonance (MR) techniques and/or nuclear medicine techniques such as positron emission tomography (PET)) could help in situations that would otherwise lead to a stroke. Since both primary and secondary prevention measures are often required, we see that the techniques can be helpful in both situations. The diseases that cause stroke that can be investigated are, among others, carotid stenosis; transient ischemic attacks (TIAs) may also be followed by a major stroke if nothing is undertaken. It has been established that carotid stenosis is to be treated in the presence of a significant lesion that has neurological symptoms. The question of how to deal with these patients often arises when the relationship between the stenosis and symptoms is not significant or the symptomatology unclear. In such situations, either PET and/or fat-saturated T1 images of the carotids can help to demonstrate the embolic nature of the plaque. We have seen that carotid plaque vulnerability, which can cause embolism, can be associated with plaque inflammation (seen on PET) or plaque haemorrhage (seen on MR images). Also, while PET and MRI will demonstrate different stages of plaque vulnerability, they can both help to demonstrate vascular lesions that are at risk of causing significant ischemic events. Diffusion-weighted imaging (DWI) has shown that some TIAs may indeed be ischemic brain lesions with a transient symptomatology. The early use of DWI can thus help treat these patients more acutely. Based on this, we have seen that newer imaging techniques can provide additional knowledge about conditions that may lead to stroke and be treated. This should have a major impact on patient outcomes and ultimately on healthcare costs related to this condition.
Keywords
Introduction
Acute ischemic cerebral stroke affects a large part of the world’s population as a major cause of morbidity and mortality. Over the last two decades, evidence has been accumulating that stroke has become a treatable entity, partly due to major developments in both diagnostic and interventional neuroradiological modalities, and this has been reflected in recently published major trials. 1 –4 Indeed, given the current absence of clearly functioning neuroprotective drugs, the standards have been achieved at first using thrombolytic pharmacological agents, 5 but accumulating evidence shows that a higher degree of safety and recanalization can be achieved with neuro-interventional techniques such as thrombectomy using so-called stentrievers. 6 These rather drastic changes in patient care have occurred in a parallel fashion with advances in neuroimaging techniques over the last two decades 7 –10 : indeed, during this time frame we have seen such developments as ultra-fast brain imaging with computed tomography (CT) and magnetic resonance imaging (MRI). These modern neuroimaging techniques can be used to detect in certain subpopulations patients who may benefit from therapeutic measures to prevent a major stroke. The modern neuroimaging techniques that are now proposed for neuroimaging ischemia are fast multi-slice CT, MRI techniques, as well as positron emission tomography (PET), and we will discuss their use and implications here, in diseases such as carotid stenosis, transient ischemic attacks (TIAs) mainly. CT techniques have gained importance due to its fast accessibility, absence of contraindications (except iodine contrast allergy) for the acute management of stroke. Indeed, CT techniques since the development of spiral and multi-slice techniques have evolved very far and allow fast coverage of the brain and vessels in order to provide both anatomic, haemodynamic and vascular images. Both CT and MR can additionally provide perfusion techniques to establish the presence of underlying haemodynamic alterations. 11 –13 Therefore these techniques could not only be helpful in the acute stroke situation but also in the prevention of stroke. Primary prevention deals with preventing the onset of a disease, whereas secondary prevention deals with preventing a disease from getting worse and tertiary prevention with improving quality of life. Neuroimaging techniques can clearly have an effect on primary prevention (such as detecting early on causes of stroke where no clear symptoms and/or lesions have appeared such as patent foramen ovale (PFO)) and on secondary prevention mainly (in cases of symptomatic carotid stenosis).
Imaging of stroke and stroke treatment
Modern neuroimaging techniques have been implemented both to image stroke and to help the work-up for treatment as well as to follow-up the patients after treatment. When dealing with acute stroke symptoms, it is first to assess the parenchyma for possible haemorrhage. 14 Haemorrhage exclusion is still best done at the moment with CT. After this comes the need to detect easily an ischemic lesion. MRI is more sensitive in the acute setting: indeed, MRI with diffusion techniques was initially likened to an electrocardiography-like technique for stroke detection 15 –19 – on diffusion imaging, the light-bulb sign will attract attention to a certain ischemic lesion. However, many practical issues made the real implementation of MRI in acute practice difficult. However, for cases where urgency of treatment is not necessary, MR and other techniques may well play an increasing role in not just helping to diagnose but to initiate and monitor less invasive treatment. This would be the case in patients where stroke prevention is being contemplated. Perfusion techniques will often be added to a CT or MR protocol but there has been a difficulty in standardization due to the multitude of perfusion techniques.
The clinically used perfusion techniques today rely on the use of CT and MR techniques. CT techniques rely on the use of iodine contrast material injected, whereas MR can be done either with or without contrast. Using contrast, MR techniques will use either T2* sequences (which are the most often used) or T1 sequences (rarely used in clinical routine) or even using the endogenous contrast of labelled blood with the arterial spin labelling techniques. These techniques all provide relative maps of cerebral blood flow (CBF) and cerebral blood volume (CBV) and do not allow the quantitative measurements provided by PET but have proven to be easily implemented clinically and to provide sufficient information about the presence or absence of altered perfusion.
While the detection of the acute ischemic lesion is important, additional important information can be gathered for treatments election such as the haemodynamic status, done with perfusion techniques. Adding perfusion will show the presence or absence of a penumbra and can help in certain cases to detect stroke mimics. Initially, CT perfusion only provided with a few slices and could not provide a full perfusion volume of the affected area. When using CT, as is done in the acute phase, multi-detector units now permit to cover a large area of the brain and to provide reliable maps of perfusion with evaluation of CBF and CBV as well as additional parameters. For CT perfusion, clinicians and investigators have relied on many variables: initially a mismatch between CBF and CBV maps would signify a penumbra. Then many vendors have tried to implement automated penumbra detection, with various degrees of success. Very often maps of mean transit time are used simply to detect a hypoperfusion, but these maps tend to overestimate the hypoperfused area.
Over the years, there has been a difficulty in standardization due to the multitude of techniques: while on the one hand CT settings are more or less standardized, the post-processing softwares have been shown to provide variable results. 20,21 The trend has changed over the years from predictive maps to using the basic maps and back again to software solutions such as, for example, the RAPID software that was shown to provide reliable results in the recent trials 22 by providing multi-parametric maps of brain perfusion as well as predictive penumbral maps. Today, most proposed software solutions are able to provide sufficiently solid data regarding hypoperfusion. RAPID was the first whole-brain software that was shown in a positive trial to have been easy to use and of benefit to the patients. Very often previously it was necessary to adjust manually arterial input functions manually, which could be difficult outside of regular working hours as well as inaccurate. 20 –22 When using MR, the typical diffusion–perfusion mismatch model is used, which relies on T2* images performed after contrast administration.
Additionally, non-contrast perfusion techniques such as arterial spin labelling techniques are possible with MRI. 23 The MR model of the penumbra rests on the model that the central diffusion deficit may constitute an initially dead core while the surrounding hypoperfused tissue is at least in part constituted of penumbra. It has been shown that diffusion lesions tend to grow with time until they fill out the hypoperfused area. 23 While PET imaging has been for a long time the main way of investigating physiology and physiopathology in the brain, due to the short half-life of even rather simple radiotracers such as O15, it has been relegated for the brain at least now to a research role, since it can be used as a gold standard for the quantification of studies of blood flow using other techniques. 24 Due to issues regarding its difficulty of use, it has no clear use in the acute setting of stroke.
Overall in the acute setting, an extensive evaluation should be performed including the brain parenchyma, the intracranial and extracranial vessels with angiography, and perfusion. In order to plan eventual intervention and assess the possibility of carotid wall pathology, angiography from the aortic arch should be provided. Since in many instances CT is done in first intention, very often follow-up MR may be necessary in order to find smaller lesions that may be only visible on diffusion-weighted imaging (DWI) but mainly a fat-saturated sequence T1 3D of the neck in order to detect plaque pathology. These protocols will be the same for the brain when dealing with preventive type protocols.
Transient ischemic attacks
TIAs 25 are defined as the occurrence of a neurological deficit syndrome that does not persist more than 24 h and were traditionally considered apart from clear ischemic lesions. About one-third of acute TIA patients will develop a major stroke, within 3 months, and a significant percentage of those patients will develop a final stroke in the first 2 days after the initial event. Indeed, according to the literature, patients with a TIA are at risk of experiencing a subsequent stroke in approximately one-third of cases. In their analysis of previous studies, Shah et al. found that in the first days, the occurrence would vary in 9–12% of cases. Roughly one can say that 10% will have a stroke over the next 3 months and half of those in the 48 h after the initial TIA. 26 –28 Due to the increased use of MRI and especially diffusion techniques, the view on TIAs has changed drastically, 29 which has been seen in many cases. Indeed, since it has been shown that a great number of clinical TIAs are actually strokes with transient symptoms due to the detected presence of a brain lesion, this means a change in attitude. 30 –33 On the one hand these patients must be seen as patients with a stroke and thus receive the same treatment within limits. Also it has been well established that these patients with TIA will present a second bigger ischemic event in the near future. Thus depending on the severity of the signs, MRI can be done within 24–48 h in order to detect or exclude any ischemic lesion (Figure 1). Taking the patients thus in charge will allow a great number to be taken care of quickly in order to prevent a subsequent second stroke. Overall, it seems that up to 75% of cases with TIA will have some kind of alteration on acute imaging. 33 Due to the findings described in the literature, it has been decided to add the imaging findings to the already existing clinical score for evaluating TIA. Indeed, the ABCD score, which took into account age, blood pressure, clinical features and duration of symptoms, was in its third version ABCD3, when findings of imaging (mainly DWI) were included in the new ABCD3-I score. 34

Patient with TIA: MRI with axial DWI (a) and coronal FLAIR (b) shows a deep left-sided hyperintensity. TIA: transient ischemic attack; MRI: magnetic resonance imaging; DWI: diffusion-weighted imaging; FLAIR: Fluid attenuated inversion recovery.
Another clinical syndrome, transient global amnesia, has been shown to be associated with hyperintensities on diffusion-weighted MRI that most probably correspond to ischemic events. These DWI hyperintensities are often found in the left mesial temporal lobe (Figure 2). The presence or absence of such small lesions will be the sign of the occurrence of a cerebrovascular event that needs to be investigated in order to establish its cause. 34 Indeed, a clinical syndrome such as a TIA may be due to a carotid stenosis that causes embolism: in this case, a first imaging series will just exclude haemorrhage and eventually show the ischemic lesion while the patient can then be worked-up completely in order to establish the cause (Figure 3).

Patient with TIA and carotid stenosis. Acute stroke CT revealed no lesion of the parenchyma (a) and no hypoperfusion (b). Angio-CT showed a calcified stenosis of the left carotid artery (d). MRA shows severe stenosis of the left ICA (c) and there is haemorrhage of the plaque (e) on the coronal T1-weighted fat-saturated images (arrow). TIA: transient ischemic attack; MRA: magnetic resonance angiography; CT: computed tomography; ICA: internal carotid artery.

Frontal left lesion on DWI (a). Bilateral hyperintensities in the carotid walls on the coronal fat-saturated T1-weighted images, but more marked on the left side (b). No stenosis on CTA (c) but hypercaptation on the left (d). DWI: diffusion-weighted imaging; CTA: computed tomography angiography.
Extracranial carotid artery disease
Carotid stenosis is an important cause of stroke, even though not all stenosis will be associated with an ischemic event. Carotid stenosis is due to the presence of atheromatous plaque, which will evolve through phases of plaque inflammation, necrosis, haemorrhage and rupture. 35 However, the globally accepted management is surgical treatment, that is, carotid endarterectomy (or endovascular in certain cases) when one is confronted with a stenosis that is severe and symptomatic. 36,37 The diagnosis of carotid stenosis may primarily be done either after a first event or during a work-up in a patient with risk factors. If the first event is a stroke, patients will often have had a stroke CT with angiography of the neck. Otherwise, very often, carotid stenosis will be discovered during a routine clinical examination where a carotid bruit is detected and first imaging is usually carotid ultrasound with Doppler that allows looking at the stenosis as well as grade the plaque and looking at the effects on vascular flow. While digital subtraction angiography (DSA) techniques remain a gold standard, they are reserved to cases where treatment is planned and more and more non-invasive techniques such as CT angiography (CTA) and MR angiography (MRA) have replaced it. 38 –40 The degree of stenosis can be evaluated by either the North American Symptomatic Carotid Endarterectomy Trial (NASCET) or European Carotid Surgery Trial (ECST) criteria: the more easy to use clinically are in our opinion the NASCET criteria where the stenosis diameter is divided by the stenotic ‘normal’ diameter of the same carotid. In order to obtain a measurement with the NASCET criteria, a measurement is done on the lateral projection of a DSA at two levels: one at the level of the stenosis and one at the level of the carotid artery at a point where it has no post-stenotic dilatation. To obtain the ratio or degree of stenosis (in %), the stenotic diameter is subtracted from the distal diameter and divided again by the stenotic diameter. While this was initially done on DSA, this is currently done on MRA and CTA; MRA is known to overall overestimate the degree of stenosis due to flow effects and CTA can be prone to artefacts due to calcification (also MR) but both techniques do provide satisfactory results. 38 The ECST criteria use the estimated size of the carotid wall at the level of the stenotic lesion and again subtract the distal carotid artery diameter and divide by the diameter of the estimated carotid artery. Additionally, it is also important even in the absence of neurological signs to look at the brain parenchyma, and this will often be best done with MRI; indeed diffusion MRI can show the presence or absence of acute lesions and T2-weighted images will detect lesions that usually will be constituted since there is not just a shift of water but an increase of local water that contributes to the signal. Then usually in order to assess the exact degree of stenosis, nowadays either CTA or MRA will be performed. Indeed, the gold standard technique, which remains DSA or conventional angiography, is now more and more reserved for patients where an intervention is planned and will no longer be performed for diagnostic purposes alone. The atheromatous plaque is known to evolve through stages of lipid accumulation, inflammation and necrosis, which can be seen with the various advanced neuroimaging techniques that we have at our disposal. Where additional imaging techniques can certainly play a role is in the detection of not just plaque morphology but the presence of neovascular changes probably related to inflammation. Neovascularization can be demonstrated on the one hand by ultrasound techniques that have their inherent problems with user capabilities and reproducibility. Hence the need for techniques that can additionally demonstrate these changes.
MR techniques have the advantage that one can perform diffusion-weighted MR techniques at the same moment that have a very high sensitivity for even small acute ischemic events. Angio-MR has the slight disadvantage that it does slightly overestimate stenosis degree but experienced readers will compensate this. Angio-MR techniques can also be done with or without contrast agents: the main techniques for the acquisition of angiographic images with MR are with or without contrast; with contrast we have the so-called contrast-enhanced MRA techniques and we have the non-contrast ones such as time-of-flight or phase-contrast angiography. The contrast-enhanced techniques can provide images covering the head and neck regions from the aortic arch to the circle of Willis and are therefore the preferred way to image the extracranial carotids, whereas for the intracranial arteries time-of-flight techniques are preferred. Phase-contrast images are more used for the visualization of vascular malformations such as aneurysms and arteriovenous malformations. MR techniques such as fat-saturated T1 images can also show T1 hyperintensities in the plaque and vessel wall that may be attributable to haemorrhage. CT techniques such as angio-CT have a few other distinct advantages: on the one hand the use of iodine contrast provides a true luminographic effect that is the same as the one provided by DSA and the technique also allows to better see and delineate eventual calcifications that may occur. Another important aspect is the capacity of the technique to determine the presence additionally of lipid changes that will be reflected as hypodensity on the plaque. On PET imaging, evidence has shown that hypercaptation corresponds to inflammation in the plaque (Figures 3 and 4). 41 –44 Perfusion or rather post-contrast imaging since dynamic imaging at the moment would provide a too low resolution is possible also with CT and MR. One example where enhanced imaging has been of help is the so-called carotid ring sign that helps to differentiate acute from chronic occlusions. 45 From a radiological point of view, the degree of stenosis from which treatment will be decided is usually done by using the NASCET or ECST criteria, with measurements done on the images in a sagittal projection. While this applies to plaque measurements, further criteria for the evaluation before treatment may be taken into account such as plaque progression (following stenosis degree on multiple follow-up examinations) or also by looking at plaque morphology. The presence of an irregular plaque with, for example, an ulcer will be another sign that there is pathology on the endoluminal side of the vessel. An ulcer, which angiographically can sometimes be seen as a button sign, consists of a stenosis with a crater due to necrosis and rupture of the plaque with remnants at the bottom. This type of lesion is considered to be an active cause of embolism. Also, sometimes a patient will be referred for the presence of symptoms or emboli but in the absence of a significant stenosis: how can we demonstrate further that the vessel is sicker than expected from simple vessel lumen measurements? One possibility that is gaining acceptance is the use of advanced neuroimaging techniques; indeed, plaque vulnerability can be addressed by the following techniques: CT criteria, MR criteria and PET criteria. These techniques have been alluded to previously: MRI allows a more detailed detection of brain emboli and allows to see plaque haemorrhage on T1 images, while CT is excellent at providing a luminographic effect close to DSA with also an improved detection of calcifications that can be differentiated from the fibrotic elements in the plaque.
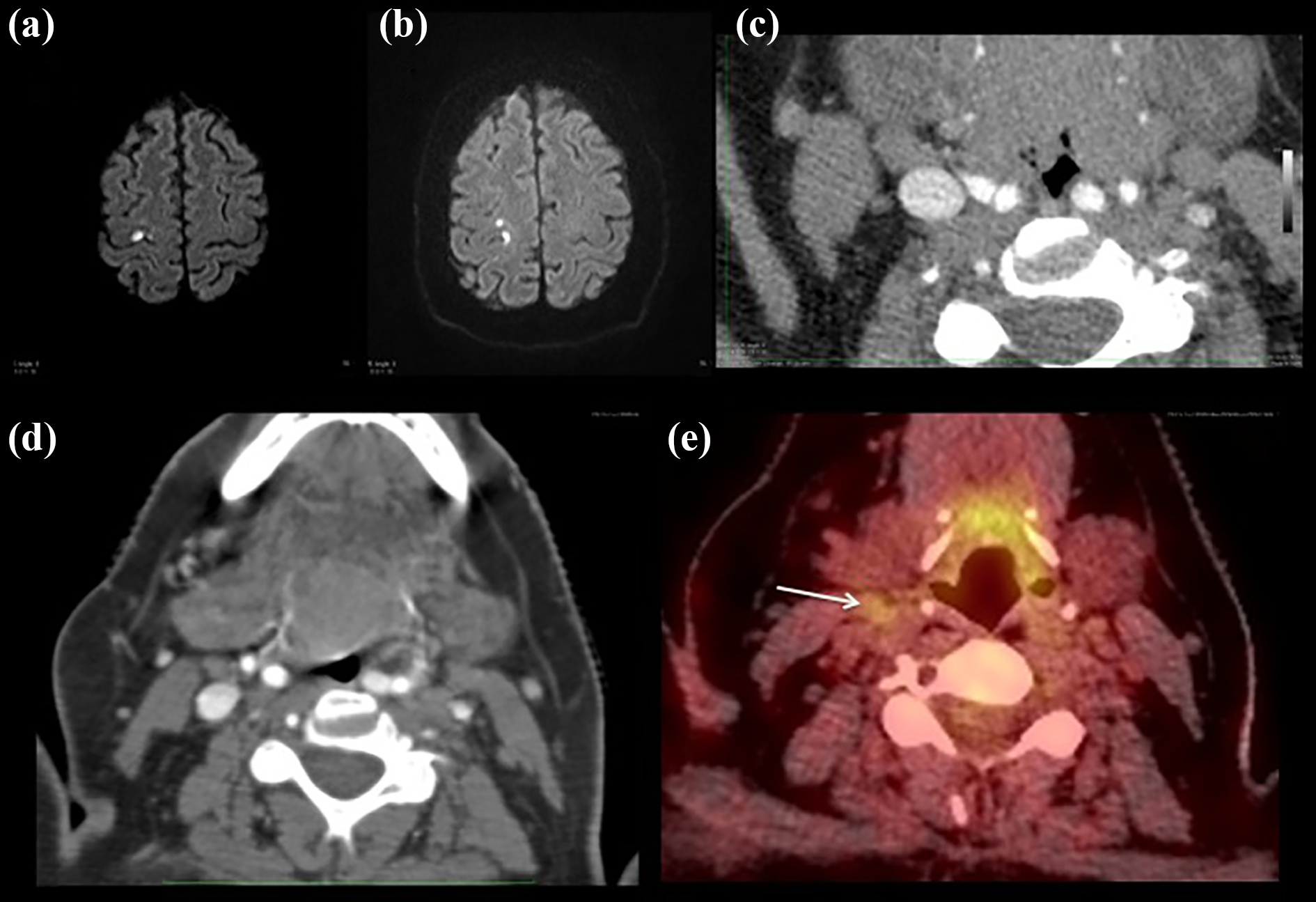
Patient with left-sided hemiparesis. On DWI (a and b) we see multiple small embolic lesions, CTA shows a non-significant stenosis (c and d). PET CT demonstrates clearly hypercaptation in the right carotid artery (arrow) (e). DWI: diffusion-weighted imaging; CTA: computed tomography angiography; PET: positron emission tomography.
Additionally, newer CT techniques such as multi-detector CT (MDCT) and dual source CT (DSCT) can provide additional information: MDCT will provide faster and improved imaging of the vessels since a better bolus tracking can be obtained along with high resolution images – this can provide partially the demonstration of lipidic necrosis which is seen as a hypodensity of the plaque in addition to calcifications; DSCT on the other hand will additionally help in reducing the stellar artefacts induced by carotid calcifications as well as help showing the presence or the absence of plaque enhancement which may occur. 46,47
Plaque enhancement while not yet entirely a standard procedure using either MRI or CT is also a possibility. In order to assess inflammation in the plaque, however, it seems more logical to use PET CT techniques that have been shown to detect plaques that embolize by showing hypercaptation on fluorodésoxyglucose (FDG) PET. It is clear that further studies are needed to validate clearly the impact of plaque morphology imaging on clinical management.
In the routine management of patients with known or suspected carotid disease, ultrasound plays an important role: indeed, it is a non-invasive and non-irradiating technique that is easily available. Done by expert hands, it can provide excellent morphological evidence on the presence or absence of stenosis, it can demonstrate the morphology of the vessel wall as well of the plaque and also by the use of ultrasound demonstrate changes in velocity. Indeed, a change in velocity is very often associated with an increase in stenosis. This technique may be done more frequently in first intention and radiological techniques such as CT and MR may be performed only in cases of symptoms or in cases of progression of stenosis on ultrasound.
Additionally, further vascular diseases can lead to ischemic stroke. Indeed, any generalized vascular process can be imaged and detected with the techniques above (e.g. vasculitides, etc.) and lesions at the level of the aortic arch can also cause stroke. When considering investigating the intracranial portion of the vessels, vessel wall imaging can be performed with MR techniques in order to assess the presence or absence of intracranial stenosis, or if there is one on angio-MR, try to help differentiate a stenosis due to vasculitis (where the vessel wall will enhance on a longer segment) from one due to dissection or arteriosclerosis. As both CTA and MRA very often examine the aortic arch at the time of the investigation, one is well advised to also to look there. Indeed, many authors have proposed to perform a vast one-stop shopping approach not just in stroke patients but also in patients with any vascular cerebral event in order to assess the state of the general vasculature. However, often during head and neck MR examinations, the aortic arch, which is at the coil limit, may not always be adequately assessed, whereas on CTA the quality of the axial images very often allows to demonstrate aortic wall calcification.
Cardiac pathology
Embolic stroke of cardiac origin may have many causes such as atrial fibrillation with thrombus formation, or even ventricular disorders such as post-infarction motility issues with thrombus formation. While some of these issues may or may not be always visible on even an extensive neuroimaging examination, they should be included in the potential differential.
PFO is associated with the occurrence of stroke, primarily of cryptogenic stroke. Thus, it is believed that some patients with a PFO will benefit from closure of this defect if there is the presence of symptoms referable to lesions. 46 Here again it is usually brain MRI with diffusion techniques that is going to be helpful in order to assess these patients. Indeed, patients with ischemic lesions referable to a PFO with diffusion and/or T2 changes that could be embolic can benefit from operative treatment (Figure 5). We have seen a move over the last years to more extensive examinations of the vascular system in cases of stroke to include not just the aortic arch and carotids but also part of the heart itself. In order to be able to perform these extensive examinations in an acceptable time, additional progress imaging speed will have to be attained both in MR and CT. 47 It seems that up to 40% of strokes may be due to a cardiac pathology so that including the heart in the acute evaluation of patients with stroke seems entirely logical. One additional way to proceed would also to try to identify the origin of the cerebral clot by performing high-resolution imaging of the clot itself to determine whether its density may point to a cardiac or non-cardiac origin. Indeed, clots that contain more red blood cells may have a higher density that could be seen on initial CT and identified better by emergent techniques such as dual-energy CT. 48 –52

Patient with PFO and ischemic lesions in the right hemisphere on DWI (a and b). T2-weighted image shows the lesion to be preset as well (c). DWI: diffusion-weighted imaging; PFO: patent foramen ovale.
Conclusions
Now that in part at least, one of the first major battles with stroke has been won, since there is no longer a limiting time frame, it seems time to evaluate the possibility of radiology to help in preventing the occurrence of acute stroke.
The possibilities provided by both diagnostic and interventional imaging techniques have provided us with new insights into how we can deal with many diseases. Cerebrovascular diseases are a prime example, where the progressive improvements in imaging speed and quality have changed what used to be exclusion tools into precise diagnostic ones. While the basic protocols for both haemorrhagic and ischemic stroke are rather similar with a combination of tissular imaging with angiography and perfusion measurements, it may often be necessary to acquire further imaging types in order to safely establish a diagnosis. The need for a more extensive evaluation of the brain tissue has been shown by the recent stroke trials: indeed, with the DAWN trial, we have seen that there is no longer the rigid 4.5 h therapeutic window for stroke patients. 53 This was even better seen by investigators in the WAKE-UP trial where it was shown that MR could help in showing what patients did not have a completed stroke yet by using the DWI-FLAIR mismatch concept. 54 Perfusion techniques can also demonstrate the viability of tissue. 55
Thus, by carefully selecting patients based on advanced imaging technique findings it will be increasingly possible to find patients who will benefit from medical treatment instead of acute treatment and long-term rehabilitation. Thus patients with an acute TIA should undergo within 24–48 h an MRI, since there is a high risk of stroke occurrence in that period. Since these patients will often have had a stroke CT with angiography and perfusion, the MR protocol can be shorter than usual due to the single question asked; usually we propose four sequences: diffusion-weighted MRI, T2*-weighted images, MRA with time-of-flight and T2-weighted MR images (or Fluid attenuated inversion recovery [FLAIR]). This will allow to detect or exclude new lesions on DWI, old lesions on T2, detect any small haemorrhagic lesions on T2* and finally detect the absence or presence of occlusion. Depending on the findings, it will always be possible to add FLAIR as well as contrast-enhanced MRA of the carotids if an acute lower pathology is excluded. At the moment, we very often add instead already the coronal fat-saturated T1-weighted images in order to detect either a dissection or a haemorrhagic plaque. For patients with carotid stenosis, the presence of a significant symptomatic stenosis on any kind of angiographic technique will indicate treatment. The problem arises mainly with patients who have symptoms and even lesions in the presence of a non-significant stenosis. What we recommend here is to look at the plaque morphology, which can be done with ultrasound or even CT; on CT one can see the presence of ulceration but also of calcific and especially hypodense changes that correspond to lipid necrosis of the plaque. Then, MRI should be performed first with coronal fat-saturated T1-weighted images of the neck region. Since hypervascularity of the plaque plays an important role, this can be assessed by ultrasound, MRI or CT. Indeed, both CT and MRI are very often acquired with contrast material for patients with cerebrovascular diseases; depending on the protocol very often stroke patients will have a CTA or an MRA after which images of the neck can be performed. MR perfusion techniques, while possible at the level of the plaque, are still in an early investigational phase, mainly due to resolution issues. Then if these are still negative and there is a strong suspicion of plaque inflammation, PET CT can be performed in selected patients. Thus for patients having a potentially vulnerable plaque, CT can demonstrate lipid deposits, MRI can demonstrate the presence of haemorrhage and finally PET techniques will reveal inflammatory changes. Thus these techniques probably provide a different vision of the vulnerable plaque time-wise. From what we have seen these changes may in part overlap. Finally, patients having an underlying cardiac disease are also at risk for embolization of thrombosed material; the most clear case is PFO where paradoxical embolism is known to occur and to cause potentially devastating effects. Thus in certain populations, among other divers, it can be thought appropriate to close these lacunes in the cardiac septum in order to not have embolism during Valsalva movements. Additionally to the purely radiological techniques discussed above, in the management of patients with proven embolic disease, be it caused by PFO or an unstable plaque, microembolic signal detection can be performed with Doppler ultrasound in order to assess the presence or absence of intravascular signals referable to active embolism. These techniques however open new therapeutic options for patients who are at risk for undergoing a major cerebrovascular event. Most important is their implication in cases where secondary prevention may have to be undertaken: that is, patients with a minor cerebrovascular event and where primary examination may not have clearly identified the severity or the source of the underlying problem. Therefore the use of additional radiological techniques can help prevent the occurrence of devastating cerebrovascular events and thus decrease long-term healthcare costs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: KOL is the recipient of research grants from the Swiss National Science Foundation (grant 160222 & SPUM grant 124114) on the topic of cerebrovascular diseases.