
Abstract
Positron emission tomography (PET) has a long history in the assessment of brain physiology and pathology; however, its initial use was limited to more academic and scientific settings. This changed radically with the clinical introduction of PET–computed tomography (PET-CT). PET-CT has become an integral part of the radiological armamentarium, especially in the assessment of patients with oncological or cardiovascular disorders. It has until now not found a clear role in neuroradiology. Indeed, magnetic resonance techniques have proven superior for the investigation of brain tumors and inflammatory diseases. However, some newer applications are emerging that can re-center PET-CT clearly in the neuroradiological world such as the investigation of vascular diseases.
Introduction
Positron emission tomography (PET) is a technique that predates Magnetic Resonance Imaging (MRI) for the exploration of the central nervous system. 1 –4 The technique has been used with great advantage for metabolic studies of the central nervous system due to the possibility of developing specific tracers. PET was also used to clinically map brain function in patients and research subjects. 5 An advanced use of the technique requires to have a cyclotron close by if short life radiopharmaceuticals are to be used. 6 With the widespread development of clinical computed tomography (CT) and magnetic resonance (MR) scanner installations, while not entirely abandoned, the technique went dormant a few years. PET studies were often reserved to studies of human brain function, which in part has been replaced by functional magnetic resonance imaging, at least for clinical studies. The technique has known a second life with the advent of PET-CT. 7 The main applications of PET-CT have been in the oncologic 8 and in the cardiovascular domains where the combined technique has allowed improved all-in one imaging protocols that have been clearly beneficial. 9 –14 The advantages of PET techniques are that besides some well-established tracers, such as Fluoro-deoxy-glucose (FDG), it is also possible, given the proper expertise and equipment, to produce and use more specific tracers. For example, in studies of cerebral ischemia, the gold standard for human studies is and remains oxygen PET. 15 Studies of brain perfusion with labeled oxygen were the standard until the development of fast MR techniques that allowed to perform studies of brain diffusion and perfusion parameters easily in the clinical setting. The precision and the robustness of the PET studies have not been equaled by the newer techniques even if they provide similar results in most given cases. It is surprising that, while CT is clearly a technique that along with MRI has known its first evolutionary steps in the domain of neuroradiology, PET-CT has been a slower starter for the specialty. The aim of this article is to address this, and on the one hand discuss what the technique can do that is specific and might be of interest to patients with neurological diseases and on the other hand discuss the drawbacks. PET indications exist that are quite clear for brain pathologies such as epilepsies or dementias but the contribution of the CT part done during PET-CT acquisitions is minimal and therefore these pathologies are not discussed here. Additionally, special makers for brain tumors can be used but again are more often used in addition to three-dimensional MR studies for exact anatomical localization purposes.
Background
PET and its clinical application have evolved in two phases mainly: the pre PET-CT and the post PET-CT years. Before the advent of PET-CT, there was not a great incentive to implement these systems in clinical settings despite the clear advantages they had. Indeed, besides the neurological applications, the use of PET for physiological imaging in both oncological and cardiovascular diseases was obvious. In neuroimaging, it was also the only technique that could reliably measure both brain function and metabolism and provide a means for cerebral mapping. All this changed on the one hand with the advent of the fast MR techniques providing functional MRI as well as MR perfusion and diffusion measurements and on the other hand with the advent with PET-CT, where applications of mainly body oncological indications became clear. The nearly indisputable applications for PET-CT have been mostly oncological for investigations of the whole body or cardiologic disease. In oncology, PET-CT is used to mainly assess the extension of metastatic extension or also the search of an unknown primary, while in cardiology, the capacity to perform cardiac metabolic studies at the same time as imaging of the cardiac vessels has shown itself useful. “While by extension, MR is mostly used in neuroradiology for the work-up of primary brain tumours, some new indications have emerged, due to its capacity to also investigate inflammatory diseases 16 or atherosclerotic disease. 17,18 The cases here refer to the use of FDG PET that is easily available; other tracers that require specialized radiopharmaceutical experience (e.g. for dementia or brain tumors) are not covered here. Overall, the presence of hypercaptation or increased uptake of FDG will serve as a maker of increased metabolism that can be found in inflammation or in increased cellular turnover.
Oncologic imaging
PET-CT is rarely indicated for the workup of primary brain tumors (Figure 1). This is partly due to the fact that MRI allows an improved anatomical differentiation and localization of the tumor. While metastatic disease in the body is very often detected by PET-CT, PET-CT is rarely used in primary intention for the detection of metastatic disease. However, in the spinal area, it can help improve lesion count and localization. Also, in cases where it is uncertain what type of lesion one is dealing with, PET-CT of the whole body can help demonstrate either the single or multiple nature of the lesion, thus helping with the differential diagnosis (Figure 2). Rare cases of benign tumors that show hypermetabolism will also be seen. PET-CT will be helpful for the evaluation of possible extension, especially in lesions involving the spine (Figures 3 and 4). Additionally, tracers such as FET (using 18Fluoro-O-(2) fluoroethyl-l-tyrosine ([18F]FET) are more and more commonly used in the evaluation of primary brain tumors. It will be used when MRI is inconclusive as to treatment response and follow-up. 19

Patient with a left hemispheric glioblastoma. MRI shows a lesion with annular enhancement on T1-Weighted-imaging (WI) ((a) and (d)); PET shows also annular hypercaptation with central necrosis ((b) and (e)). Flair shows diffuse perilesionnal edema (c). PET: positron emission tomography.

Brain CT shows hypodensity in the left striatum, with a strong enhancement (b). On T1-Weighted-imaging (WI), there is a hypodensity in the left striatum but also in the right occipital cortex, which enhances (c) with a strong dural attachment (d). T2 shows perilesionnal edema and a slight inhomogenous center with hypo and hyper intensities (e). (a) PET shows diffuse hypercatation in the left striatum, confirming the diagnosis of lymphoma, whereas the less enhancing lesion in the right occipital region is a meningioma (f). CT: computed tomography; PET: positron emission tomography.
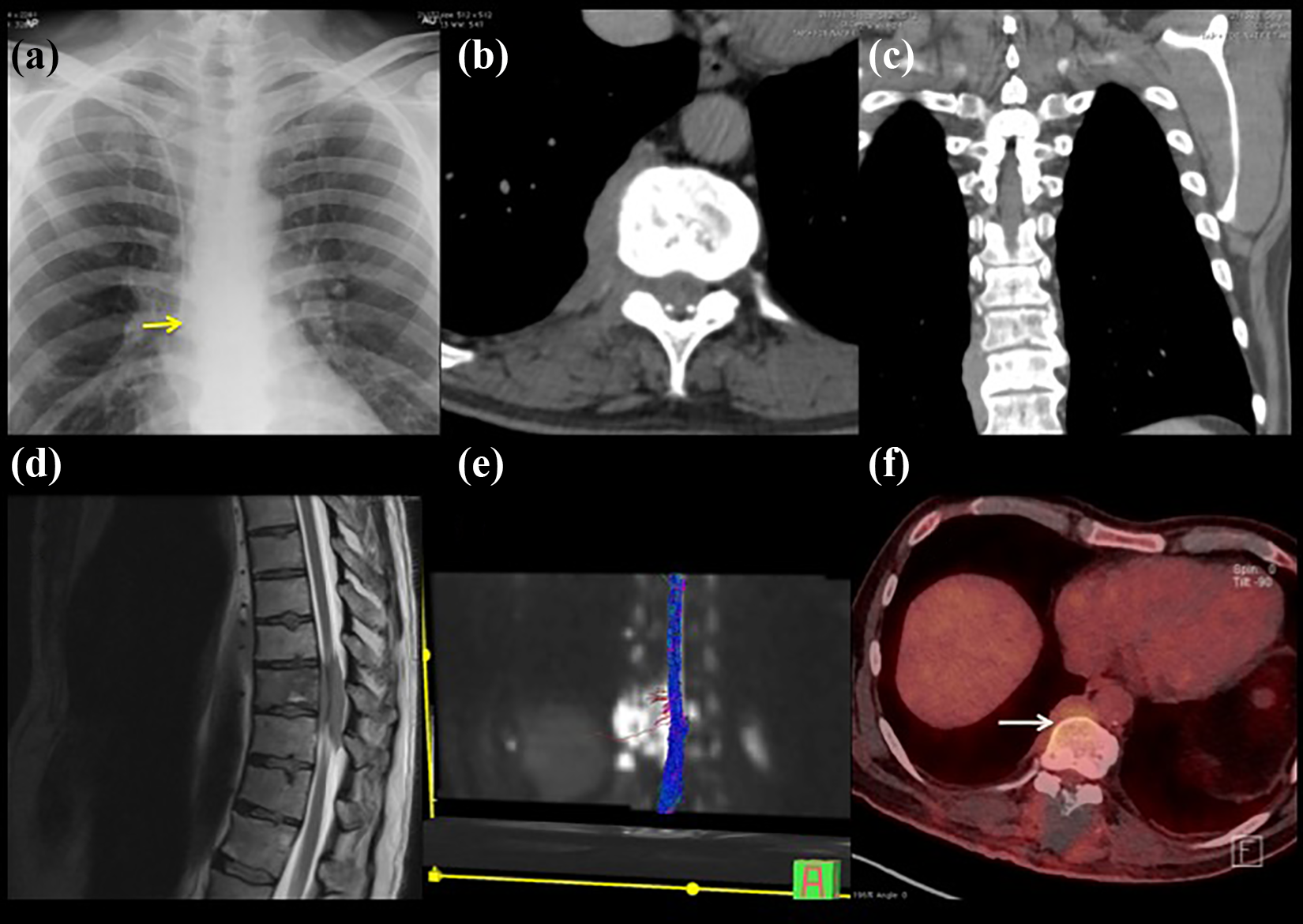
Patient with spinal metastasis: There is displacement of the right paraspinal line (a) on the chest X-ray image (yellow arrow). On CT, there is a paravertebral mass ((b) and (c)). On MRI, intraspinal component can be seen (d) which compresses the myelon as seen on Diffusion tensor imaging (DTI) (e), and PET shows the hypercaptation of the lesion (f). CT: computed tomography; PET: positron emission tomography.
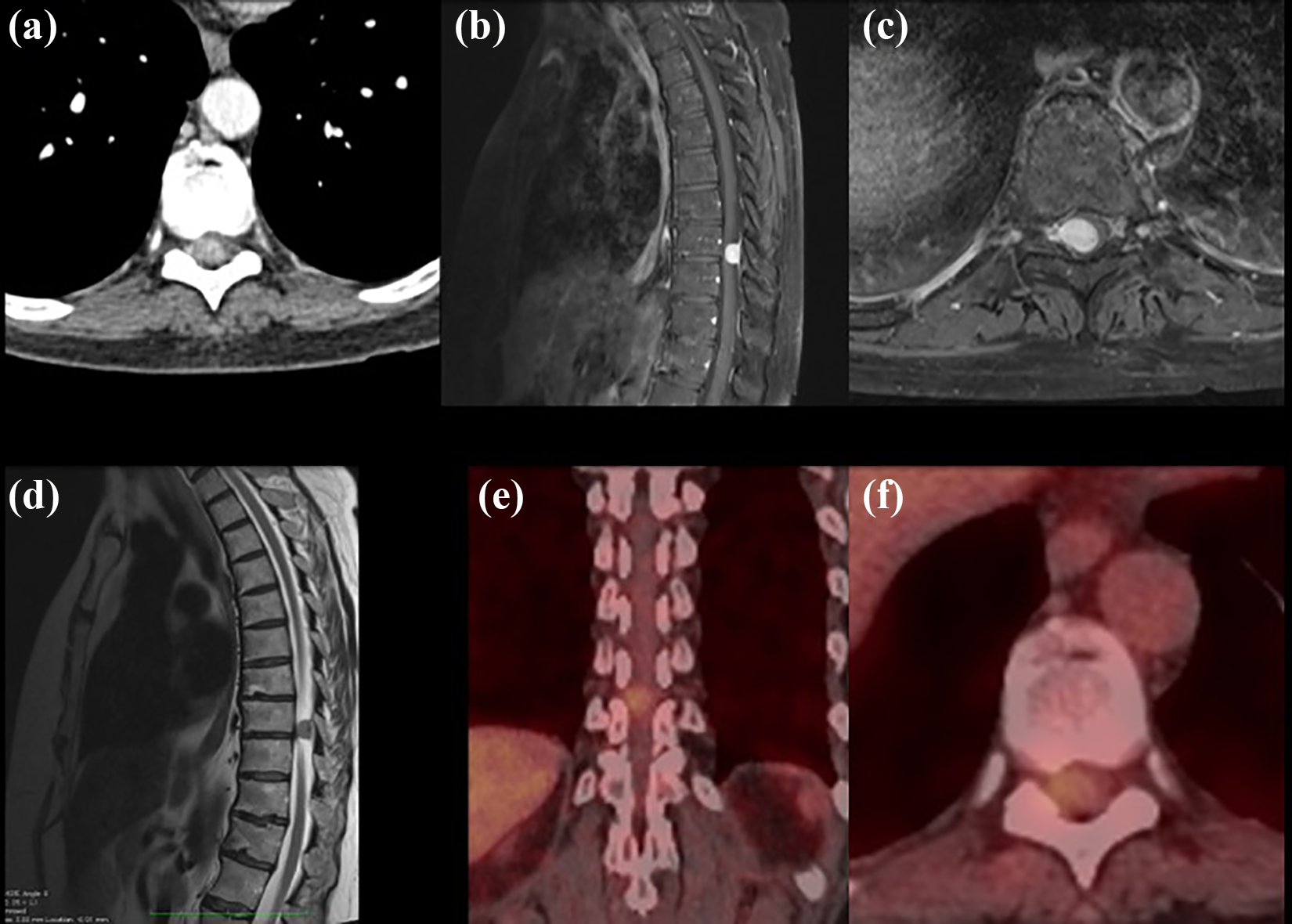
Spinal meningioma. CT shows enhancing intraspinal lesion (a), which is also seen on the contrast-enhanced T1-Weighted-imaging (WI) on MRI ((b) and (c)). The lesion is seen to compress the myelon (d). On PET-CT, no further lesions are seen but there is a slight enhancement of this highly vascularized meningioma (f). CT: computed tomography; PET-CT: positron emission tomography–computed tomography (e,f).
Vascular imaging
The most promising new indication for PET in the neuroradiological domain is clearly its increasing application to vascular diseases. Indeed, carotid artery disease, which is a cause of stroke, is generally due to arteriosclerosis. The indication for treatment, which generally involves intravascular surgery, is based upon the presence of significant and symptomatic stenosis in the cerebral vasculature (Figure 5). Decisions will be often done by a multidisciplinary cerebrovascular board where surgeons, interventionalists, radiologists, and others will confront the clinical data with the findings in order to decide which is the best therapeutic option, with the patient also having a say. Clinicians must often resolve the conflicting indications when a nonsignificant stenosis becomes symptomatic, which can lead to treatment decision contrary to accepted rules. Then, in that circumstance, the detection of an unstable plaque can be helpful. Plaque instability is usually considered to be a prediction of the risk for a vessel wall lesion to give rise to an embolism. In order to demonstrate the associated inflammation, PET-CT can be proposed, given the high uptake of FDG in the actively inflamed plaques that are prone to rupture. Ischemic or hemorrhagic brain lesions will display a typical area of hypocaptation (Figure 6).

Stroke due to carotid stenosis with an unstable plaque: CT perfusion shows acute right-sided Middle cerebral artery (MCA) hypoperfusion (a). Computed tomography angiography (CTA) shows the presence of a right-sided inhomogeneous plaque, that is approximately 60% according to north american symptomatic carotid endarterectomy trial (NASCET) criteria ((b) and (c)). Fat-saturated T1-Weighted-imaging (WI) of the neck in a coronal plane shows hyperintensities in the plaque corresponding to hemorrhage ((d) and (e)). On PET-CT, there is hypercaptation in the right-sided plaque (f). PET-CT: positron emission tomography–computed tomography.

Brain hematoma in the left hemisphere visible on CT (a). On Digital subtraction angiography (DSA), there is mass effect with displacement of the Middle cerebral angiography (MCA) upward but no tumor blush (b). MRI shows an inhomogeneous lesion in the left temporal lobe ((c) and (d)), while PET shows the absence of hypercaptation (e), compatible with a hematomas, as well as the absence of other lesions on the whole-body examination (f). PET: positron emission tomography; CT: computed tomography.
Imaging of inflammatory lesions
Inflammatory lesions will very often show hypercaptation. In some instances, where they have not been definable by conventional X-ray images, MRI, or CT, PET-CT can be helpful to demonstrate either the single or multiple aspect of the lesion or the pathology which can help to differentiate a primary from a secondary lesion (Figure 7).

Young patient with persistent headache: Skull X-ray image (a) shows a slight area of bone erosion at the vertex, confirmed by CT (b). MRI shows an enhancing lesion ((c) to (e)) which also has hypercaptation in PET-CT, compatible with histiocytosis X (f). PET-CT: positron emission tomography–computed tomography.
Conclusions
PET-CT from a neuroradiological point of view is a technique that is probably underutilized but still has some drawbacks. One impediment to its wider use in radiology arises from the relatively high cost of PET-CT instrumentation and examinations, which require purchase or local production of the radiotracer. However, in centers that avail themselves of the state-of-the art PET-CT instruments, and with the recent advent of hybrid PET-MR imaging, there are clear indications for the technique even of they have to be defined clearly. PET is of established value in clinical neuroradiology, and its use tends to increase due to its effectiveness in surgical guidance for intractable epilepsy, and the burgeoning demand for diagnosis of dementia. However, in these applications, anatomic registration is usually made to an MR image. While in comparison with MRI, it is very expensive and does not have the spatial resolution of high-resolution MRI, and it is superior to MR for certain tasks such as defining zone of radiation necrosis, which has a positive impact with regard to patient management and outcome. Due to the current progress and developments in the area of the diagnosis and management of cerebrovascular diseases, the area where PET-CT seems positioned to present the most clear-cut advantages is for the monitoring of carotid artery disease. While the indications for treatment have been clearly stratified, it is unequivocal that a symptomatic high-grade stenosis is to be treated, what is more unclear is how to deal with patients who have for example a symptomatic low-grade stenosis. Here, by adding PET, it is possible in certain cases to demonstrate inflammatory changes that may be a sign of plaque instability and fragility.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.