
Abstract
A 45-year-old man presented to the neurotology clinic, suffering from recurrent attacks of vertigo associated with falls, of unknown origin. Pure tone audiometry revealed a profound right-sided and mild left-sided pantonal sensorineural hearing loss. Caloric videonystagmography showed marked canal paresis on the right side. Video-head impulse test, however, showed bilaterally normal gain. Cranial magnetic resonance imaging (MRI) was normal. No neurovascular compression was noted. We performed locally enhanced inner ear MRI (LEIM). LEIM revealed a marked dilation of the endolymphatic space of the right inner ear, that is, endolymphatic hydrops. In light of the history, clinical, functional and imaging results, therefore, the diagnosis of hydropic ear disease (Menière’s disease) with vestibular drop attacks could be established. This clinical image case illustrates the usefulness of inner ear imaging for the differential diagnosis of vertigo disorders, such as hydropic ear disease (Menière’s disease).
Keywords
Case report
A 45-year-old man presented to the neurotology clinic, suffering from recurrent attacks of vertigo associated with falls. The vertigo was of rotatory nature, but lasted only a few seconds. There was no loss of consciousness and no provoking factors could be identified. There was no concurrent ataxia and no nausea or vomiting. These attacks had been occurring since more than 10 years. In the last few years, they appeared more frequently, recently as often as three times in 3 weeks. Furthermore, he felt a vague dizziness (insecurity) on a few days per month. He has tinnitus bilaterally. No aural pressure, no Tullio phenomenon. Twenty-two years ago, he had suffered a sudden hearing loss on his right side.
In the past, the patient was examined with an electroencephalogram (EEG), suspected of epilepsy and treated with Levetiracetam. The EEG recordings, however, upon review by a universitary epilepsy centre, did not reveal any peaks consistent with epilepsy, and the drug was stopped.
On examination, the patient’s stance and gait tests were normal. Otomicroscopy was normal. There was no spontaneous nystagmus or head-shaking nystagmus. The bedside head impulse test (HIT) was normal. Positioning manoeuvres did not provoke positional nystagmus or vertigo. The neurologic examination was normal.
Pure tone audiometry revealed a profound right-sided and mild left-sided pantonal sensorineural hearing loss (Figure 1(a)). Tympanometry showed type A tympanograms bilaterally. Caloric videonystagmography showed marked canal paresis on the right side. Video-HIT, however, showed bilaterally normal gain, with bilateral minor catch-up saccades (Figure 1). Cervical and ocular vestibular evoked myogenic potentials were present on the left, but absent on the right side. Cranial magnetic resonance imaging (MRI) was normal. No neurovascular compression was noted.

Video-HIT: The gain asymmetry is 2% and therefore normal. On both sides, minor catch-up saccades are present. The finding of a preserved head impulse response in combination with reduced caloric function is typical of hydropic ear disease (Menière’s disease). HIT: head impulse test.
We performed locally enhanced inner ear MRI (LEIM). Under otomicroscopic control, 0.5 ml of diluted (1:8) gadolinium-based contrast (Magnevist) was injected into the right tympanic cavity with the patient in supine position, the head turned 45° contralaterally, for the following 30 min. The MRI scan was obtained 24 h after the contrast application.
For MRI, a 3T scanner (Signa HDx, GE Healthcare, Milwaukee, Wisconsin, USA) with an eight-channel head coil was used. To visualize inner ear contrast, we acquired a high-resolution fluid-attenuated inversion recovery sequence with the following parameters: TR: 9000 ms; TE: 135 ms; TI: 2500 ms; matrix size: 256 × 256; field of view: 16 cm (square); slice thickness (axial acquisition): 0.8 mm; number of excitations: 2. Additionally, an MR cisternography using the fast imaging employing steady-state acquisition sequence was acquired at the same time point (i.e. 24 h after contrast application), for evaluation of the inner ear total fluid space anatomy.
LEIM revealed a marked dilation of the endolymphatic space of the right inner ear, that is, endolymphatic hydrops (ELH; Figure 2). In light of the history, clinical, auxiliary and imaging results, therefore, the diagnosis of hydropic ear disease (Menière’s disease) with vestibular drop attacks could be established. The patient was counselled accordingly and offered vestibular ablative therapy with Gentamicin, but presently wished an observational regimen.

LEIM of the right ear. (a) and (c) Fluid attenuated inversion recovery sequence. Here, the perilymphatic space appears with high signal intensity (white), whereas the endolymphatic space appears with low signal intensity (black). Brain tissue and cerebrospinal fluid appear grey. (a) The cochlear endolymphatic duct is markedly enlarged, therefore only the scala tympani perilymph signal is visible. At the location of the scala vestibuli, the high-intensity perilymph signal is missing (arrows). (c) The vestibular endolymph space (arrow) is mildly dilated. (b) and (d) Renderings of magnetic resonance cisternography of the inner ear for anatomical reference. Here, the whole inner ear fluid system, endolymph and perilymph, appears equally with a high signal. LEIM: locally enhanced inner ear magnetic resonance imaging.
Discussion
The differential diagnosis of dizziness and vertigo is a frequent clinical problem. Particularly, recurrent vertigo attacks are often difficult to classify, when differential diagnoses such as hydropic ear disease (Menière’s disease), vestibular migraine, vestibular paroxysmia, and psychogenic vertigo are considered. When sudden falls occur, even epilepsy has to be considered as potential cause.
Hydropic ear disease (Menière’s disease) is one of the most common inner ear disorders and is characterized by sudden attacks of rotatory vertigo, hearing loss, tinnitus and aural pressure in its full-blown clinical manifestation. 1 Furthermore, drop attacks may occur, and in the long-term, there is progressive and permanent loss of audiovestibular functions.
In the present case, the duration of the attacks was only a few seconds. Furthermore, there were no auditory symptoms associated with the vertigo attacks. This stands in contrast to the diagnostic criteria for Menière’s disease, 2 even though the presence of hearing loss points toward an inner ear disease as the cause for the vertigo attacks. The vestibular auxiliary tests revealed a pattern which is typical of hydropic ear disease (Menière’s disease): decreased caloric function, but preserved high-frequency vestibulo-ocular reflex as assessed by video head-impulse testing. 3 However, only the morphological demonstration of ELH completed the clinical picture and could therefore ascertain the diagnosis of hydropic ear disease.
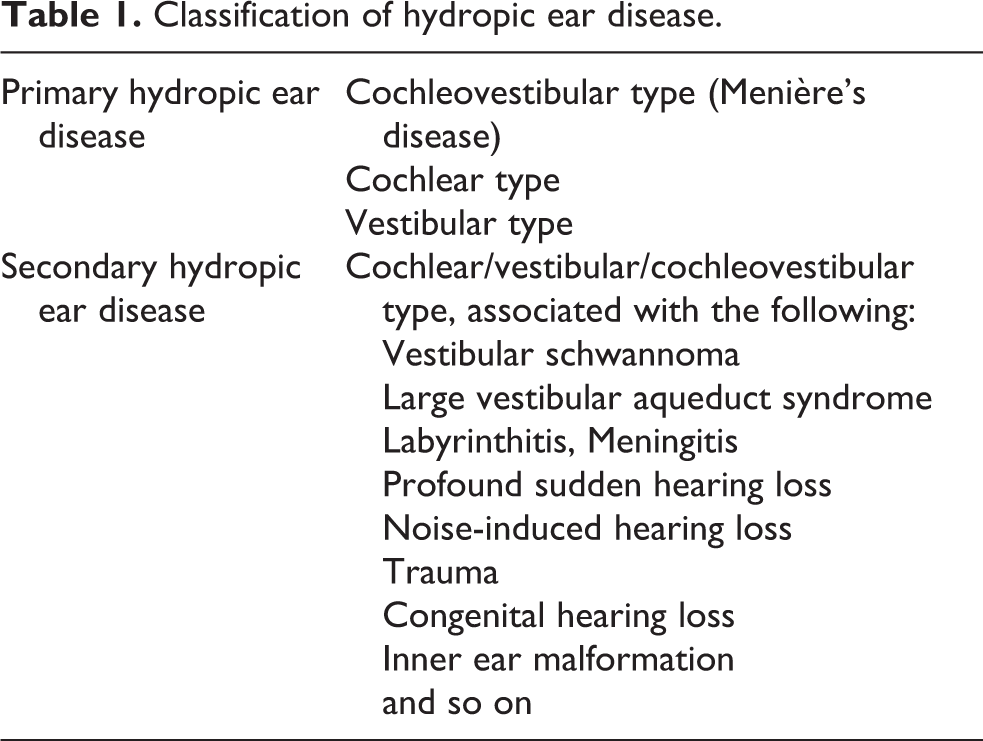
Since the first visualization of endo- and perilymphatic spaces in a living patient by clinical MRI in 2005 4 and the first visualization of ELH in Menière’s disease (MD) patients, 5 the imaging of ELH has been installed in various centres across the world and gathered important insights. 6 –8 The correlation between the degree of ELH and the audiovestibular function loss has been demonstrated, 9,10 the differential diagnosis between MD and vestibular migraine has been improved, 11 and first attempts at volumetric quantification of the minute endolymphatic space (about 50 µl) have been made. 12,13 Furthermore, the in vivo discovery of the hydropic hernation into the semicircular canal 14,15 has provided a morphological basis for the understanding of the caloric-HIT – paradox typical of MD and also present in the case described above. Recently, these new insights have been translated into the new classification of hydropic ear disease. 1,16,17 In this classification, all the clinical subgroups of ELH are summarized in a logical and comprehensive manner (Table 1). Since Menière’s disease is defined as the idiopathic syndrome of ELH, 18 it is to be expected that the translation of ELH imaging into clinical practice will improve diagnostic accuracy. Especially those cases with an “incomplete” MD picture will likely be more frequently recognized, for example, fluctuating low-frequency hearing loss (=hydropic ear disease of cochlear type), or delayed ELH (=secondary hydropic ear disease), such as the case of secondary hydropic ear disease associated with pre-existing profound sudden hearing loss presented here.
Classification of hydropic ear disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.