
Abstract
Neuro-otology and neuro-ophthalmology are clinical fields destined to be combined in a single interdisciplinary center that offers state-of-the-art diagnosis and treatment to patients with vertigo, dizziness, imbalance, eye movements disorders and disorders of the afferent visual pathways. This paper describes the organization of the Oto-Neuro-Ophthalmology (ONO) center at University Hospital Zurich, Switzerland. The ONO center combines physicians and other medical personnel from the departments of neurology, otorhinolaryngology, ophthalmology, and psychiatry as well as dedicated physical therapists. Patients, typically referred to the center by general practitioners or medical specialists, are comprehensively assessed and treated by considering all neurological, otological, ophthalmological, psychiatric and physiotherapeutic aspects of their disorders. Based on the referral, the patient is assigned to a triage examination (duration: 30 minutes; no later than 10 days after referral) or a full examination. The latter includes a complete assessment of the medical history, a bedside examination, a laboratory test battery and imaging procedures. Importantly, the ONO center is partnered by an experimental laboratory dedicated to vestibular and ocular motor research and formed by the academically active members of the ONO center. To justify the collaborative efforts that go into establishing and continuously upgrading an ONO center, outcome measures become increasingly important.
Introduction
Dizziness, vertigo, and imbalance are among the most frequent symptoms that cause patients to see their doctor. 1 –4 The multitude of underlying diseases requires close collaborations of specialists from different disciplines to ensure optimal diagnosis and therapy. 5 Accordingly, the Oto-Neuro-Ophthalmology (ONO) center at University Hospital Zurich combines physicians and other medical personnel from the Departments of Neurology, Otorhinolaryngology–Head and Neck Surgery, Ophthalmology, and Psychiatry and Psychotherapy. Physical therapists, who are specialized in assessing and treating balance disorders, are assigned to the center as well.
This article describes in short the organization of the ONO center, which has evolved since its foundation in 2004, when we combined the neuro-otological resources of the departments of neurology and otorhinolaryngology. Presently, the center is called “Interdisciplinary Center for Vertigo and Neurologic Visual Disorders” (in German: “Interdisziplinäres Zentrum für Schwindel und neurologische Sehstörungen”). Before the formal integration of the neuro-ophthalmological service of the department of ophthalmology, the center was called “Interdisciplinary Center for Vertigo and Balance Disorders” (in German: “Interdisziplinäres Zentrum für Schwindel und Gleichgewichtsstörungen”).
Currently, the ONO center is headed by five physicians, who are specialized in neuro-otology, neuro-ophthalmology, or psychiatry. They are Klara Landau, MD (Department of Ophthalmology), Michael Rufer, MD (Department of Psychiatry and Psychotherapy), Dominik Straumann, MD (Department of Neurology), Vincent Wettstein, MD (Otorhinolaryngology-Head and Neck Surgery), and Konrad P Weber, MD (double affiliation: Departments of Neurology and Ophthalmology). These colleagues affiliated with one of the four collaborating departments. The staff of the ONO center include four attending senior physicians working part-time for the center, namely, Katja Komossa, MD (Department of Psychiatry and Psychotherapy), Arianne Monge, MD (Department of Otorhinolarynology), Alexander A Tarnutzer, MD (Department of Neurology), and Ghislaine Traber, MD (Department of Ophthalmology); four residents; four laboratory technicians; and a part-time secretary. The salaries of the positions are included in the budgets of the respective departments. Over the years, about half of the present positions were created by the directorate of the hospital based on business plans justifying the expansion of the ONO center. The infrastructure for laboratory testing, examination rooms, and offices, although assigned to different departments, is shared within the ONO center.
The typical rotation for residents in the ONO center lasts for 6 months. In our experience, this period is long enough to gain solid skills in bedside testing, differential diagnosis, and therapeutic planning. Interested residents are involved in clinical studies on patients recruited by the center.
Importantly, the ONO center is partnered by the Vestibulo-Oculomotor Laboratory, an experimental laboratory dedicated to vestibular and ocular motor research and formed by the academically active members of the ONO center. The laboratory was founded by the late Volker Henn 6 and has a 45-year research history. From the beginning, the main goal of the Zurich-based research was that clinically relevant results from the in-house basic research could be applied in patient care. With more insights into the fundamental processes involved in eye and head movements and with the refinement of painless examination methods, the possibilities for diagnosing patients have increased significantly. In the Vestibulo-Oculomotor Laboratory, there is a constant flow of studies that involve patients recruited by the ONO center.
First appointment
Patients, usually referred to the center by general practitioners or specialists, are comprehensively assessed and treated by considering all neurological, otological, ophthalmological, psychiatric, and physiotherapeutic aspects of their disorders. A questionnaire, which is sent out together with the appointment and can also be filled out online, facilitates the diagnostic procedure.
Based on the referral, the patient is assigned to a triage examination or a full examination (Figure 1). A triage examination is indicated, if we suspect a benign paroxysmal positional vertigo (BPPV) or a condition that requires a fast decision on whether cranial imaging is required. The triage examination takes place no later than 10 days after the referral and consists of short neuro-otological workup (focused history taking, ocular motor and pupillary testing, head impulse test, provocation maneuvers with Frenzel goggles, Romberg on foam, gait). 7 If the patient suffers from BPPV, a liberation maneuver will be performed during the same appointment. The triage examination lasts for less than 30 min.

Flow chart of the diagnostic procedures. The triage examination is scheduled within 10 days (d) of the referral, while the waiting period for a full examination should not take more than 5 weeks (w).
Unless the patient is assigned to a triage examination, the first appointment is dedicated to a complete assessment of the medical history and to bedside tests. The patient is first seen by the resident. Thereafter, the attending neuro-otologist or neuro-ophthalmologist is asked to review the history and to repeat selected bedside tests. Finally, the patient is informed which laboratory tests and imaging procedures would be required to further delineate the diagnosis and prognosis and to help choosing a rational therapy.
Laboratory tests
A broad battery of tests measuring the functions of inner ear, eye, cranial nerves, and areas of the brain for balance, eye movements, and vision is available.
The choice of tests to be applied depends on the results of the clinical investigation and is thoroughly discussed with every patient. Tests are coordinated such that they can all be completed during the second consultation. Thereafter or, if required, during the next consultation, the final diagnosis is explained to the patient and a tailored therapeutic concept is proposed.
ONO board
The center’s neurologists, otologists, ophthalmologists, psychiatrists, and physical therapists hold a weekly interdisciplinary ONO board meeting. Here, patients with complex ONO disorders are being discussed. The main purpose of this board meeting is to develop personalized therapeutic concepts for each patient. If possible, the patient is present at the discussion. If not, the patient is later informed about the recommendations of the board by phone or during the next consultation. Provided the patient agrees, the recommended pharmacological, optical, physical, and behavioral therapies are initiated.
Canalith liberation maneuvers on motorized three-axis turntable
Positional vertigo is the most common form of dizziness. 4 In most patients, this positional vertigo is elicited by changing the position of head relative to gravity. Calcium crystals, which are usually fixed in the otolith organs, drift freely within the semicircular canals of the inner ear and cause rotational vertigo during sedimentation to the lowest points of the canals. With specific maneuvers, the canals can be liberated from the calcium crystals at the bedside. 5 In therapy-resistant cases or if the patients' mobility is restricted (immobile neck, frailty, invalidity, etc.), the maneuvers are performed on the three-axis turntable (Figure 2).
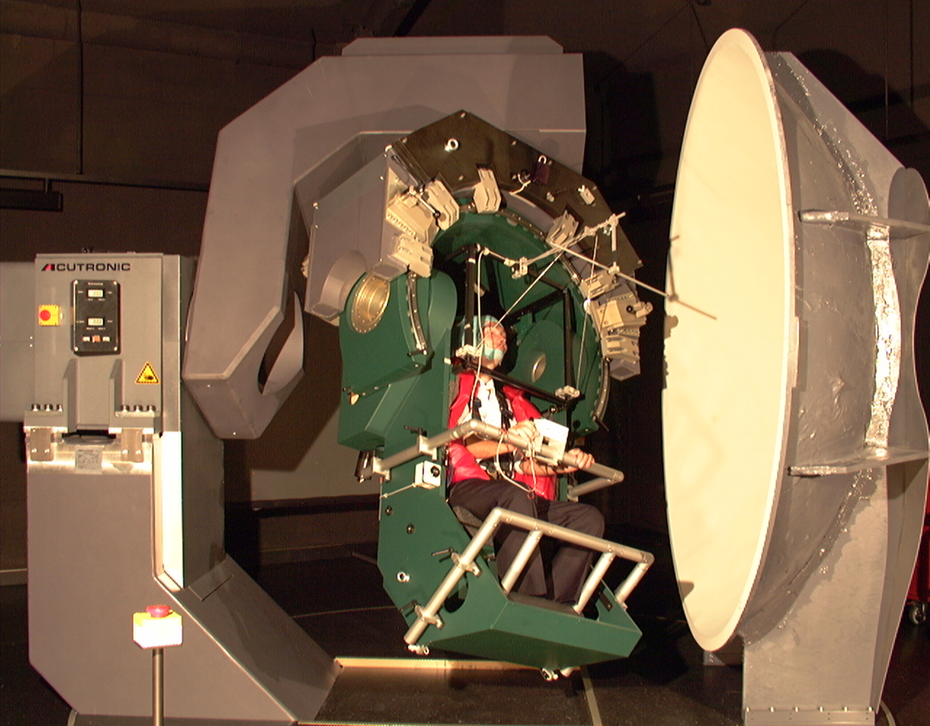
Motorized three-axis turntable for vestibular research. The turntable is also used for canalith liberation maneuvers in patients with BPPV. BPPV: benign paroxysmal position vertigo.
Obstacles
Over the years, the further development of the ONO center repeatedly had to pass through phases of increased viscosity. Key, especially during such phases, is the collegial and open relationship among the leading physicians of the center, who themselves are affiliated with the different collaborating departments.
Hierarchy would be detrimental for an ONO center. One of the senior physicians, however, should volunteer to be the spokesperson vis-à-vis the administration and the directorate of the hospital.
Obstacles may arise at two different fronts:
Personal conflicts among members of the center.
(Subconscious) resistance from administrators of individual departments. They are trained to act in the interest of their departments and may see interdisciplinary activities as distractions and potential threats (especially room-wise) to the department they serve.
On the positive side, department chairpersons and hospital executives are mostly very supportive with respect to the needs of a center dedicated to vertigo and dizziness.
Advice
For other ONO centers being planned or wish to further expand, the following points are advised:
An ONO center can only thrive, if its construction and expansion are bottom-up, that is, if they originate in the motivation and activities of the participating colleagues.
Be patient regarding the slow administrative progress in support of an interdisciplinary center. The basic elements of present hospitals are still the departments. Every room and every position for the center implies sacrifices of the collaborating departments (unless the hospital is expanding). While the value of interdisciplinary medicine is undisputed among physicians, nonmedical staff often lacks the appreciation for interdisciplinary endeavors.
Build up a reputation of the center by top-quality patient care. Especially for ONO disorders, which may cause depression and anxiety, the dedicated dialogue with the patients is so important.
Abstain from noisy advertisement of the center. It will only produce unhappy patients because of irredeemable promises and longer waiting periods.
Outcome measures
To justify the collaborative efforts that go into establishing and continuously upgrading an ONO center, outcome measures become increasingly important. A yearly reporting of statistical numbers on patients’ visits, auxiliary tests, personnel, and resources is indispensable. A growing list of scientific and popular publications can underscore the continuous activity of the center. Finally, scientific evaluations of diagnostic and therapeutic procedures should demonstrate whether the ONO center impacts the management of patients in a significant and beneficial way. 5
Conclusion
Neuro-otology and neuro-ophthalmology are clinical fields destined to be combined in a single interdisciplinary center that offers state-of-the-art diagnosis and treatment to patients with vertigo, dizziness, imbalance, eye movement disorders, and disorders of the afferent visual pathways. ONO also provides great opportunities for interdisciplinary clinical research among neurologists, otologists, ophthalmologists, psychiatrists, and physical therapists. The ONO center in Zurich has slowly evolved by a gradually increasing collaboration among the participating departments and a stepwise creation of positions by the directorate of hospital based on business plans. In contrast, the German Center for Vertigo and Balance Disorders at the University of Munich, which is the most prominent example of a successful ONO center worldwide, was made possible through funding by the federal government. In the absence of such generous funding, a gradual evolution of an ONO center is the only alternative.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.