
Abstract
Introduction
Intraocular steroid therapy has been an essential part of the treatment armamentarium for disease processes associated with various retinal vascular and uveitis etiologies. Well-known side effects of steroid therapy include ocular hypertension and cataract formation. Ocular hypertension is defined as an intraocular pressure (IOP) of >25 mm Hg or an increase in IOP of at least 10 mm Hg from baseline. Steroid-induced glaucoma has been postulated to occur as a result of decreased outflow at the trabecular meshwork due to physical impedance, toxic effects on trabecular meshwork cells, and upregulation of the myocilin gene. 1 It is estimated that approximately 40% of the United States general population are steroid responders. 2 Generally, steroid-induced IOP spikes are transient and will reverse with cessation of steroid use but can lead to worsening of glaucomatous optic neuropathy. 3 Therefore, it is important for the clinician to be able to identify and counsel those patients at highest risk of developing complications.
Intravitreal (IVT) triamcinolone acetonide and dexamethasone implants are 2 of the most common treatment modalities for intraocular steroid delivery. In phase III clinical studies, the most common adverse effects of the dexamethasone implant were increased IOP, with 32% of patients having a posttreatment IOP of >25 mm Hg and 41.5% having concurrent use of IOP-lowering medication. 4 Mean IOP increases occurred around 6 weeks. In contrast, in a meta-analysis of 3654 eyes treated with IVT triamcinolone, 32.1% of eyes (95% CI, 28.2–36.3) receiving the 4 mg/0.1 mL dose developed ocular hypertension. 2 That same meta-analysis also showed that ocular hypertension was observed in 15.3% of eyes (95% CI, 9.2–24.3) following treatment with 0.7 mg dexamethasone implant. Although no direct comparison was made, the dexamethasone implant was thought to be associated with fewer increases in IOP compared with IVT triamcinolone. 2 Another study, again without directly comparing the 2 steroid therapies, demonstrated results that concurred with those findings, suggesting that dexamethasone implants would have fewer IOP-related issues due to its reduced lipophilic tendency and the lower likelihood of physical obstruction of the trabecular meshwork from triamcinolone crystals. 1
Despite their regular use in clinical practice, the relative adverse effect profiles of IVT triamcinolone and dexamethasone implants remain poorly characterized. The goal of this study was to determine the risk of needing treatment for ocular hypertension after use of IVT triamcinolone compared with a dexamethasone implant.
Methods
Database
De-identified data were abstracted from the Optum Clinformatics Data Mart Database. The database contains all outpatient medical claims (office visits, procedures, and medications given) as well as demographic data and some laboratory values for all patients enrolled in commercial and Medicare Advantage insurance plans. The subset of data available for this study included all patients in the database from January 1, 2009, to June 30, 2022.
Cohorts
For the study, we identified all patients who initiated treatment with either IVT triamcinolone acetonide or a dexamethasone implant after January 1, 2011. The study evaluation period was started in 2011 due to the availability in that year of the dexamethasone implant after US Food and Drug Administration approval. Two cohorts were created based on the first type of treatment received, either IVT triamcinolone or dexamethasone implant. The earliest date of the incident injection was considered the index date. Patients were excluded for having any prior diagnosis of ocular hypertension, suspected glaucoma, or glaucoma or for receiving glaucoma-related procedures or prescriptions prior to the index date (see Supplemental Table 1 for the full list of International Classification of Diseases, Ninth or Tenth Revision codes and Current Procedural Terminology codes used during this study). Patients were also required to have at least 2 years of uninterrupted time within the data set prior to the index date. To further limit the occurrence of secondary glaucoma, all patients before or after the index date who had been diagnosed as having neovascular glaucoma, had received systemic steroids within 90 days of the index date, or had received a fluocinolone or retisert implant were excluded.
Covariates and Inverse Probability of Treatment Weighting
To reduce the effects of confounding due to potential differences in the baseline characteristics between the 2 cohorts, propensity scores were calculated using multivariable logistic regression. Covariates included in the model were age, sex, race, education level, household income, geographic region of the country, index year, smoking status, number of healthcare visits within 1 year prior to the index date, history of uveitis, hypertension, hypercholesterolemia, chronic kidney disease, ischemic heart disease, ischemic stroke, heart failure, peripheral arterial disease, and coronary artery bypass graft, and history of use of steroid drops and sub-Tenon triamcinolone in the 120 days prior to the index date. Inverse probability of treatment weighting with the propensity scores was used in the subsequent analyses.
Outcome of Interest
The primary outcome of interest was progression to ocular hypertension, which was defined as the filling of a prescription for a glaucoma medication or having a glaucoma procedure. Because not all ocular hypertension leads to a diagnosis of glaucoma, a sensitivity analysis anticipating fewer outcomes was used in which the outcome was alternatively defined as having a new diagnosis of glaucoma or suspected glaucoma. Both outcomes have been used previously.5–7
Statistical Analysis
Cox proportional hazards regression modeling with inverse probability of treatment weighting was performed to compare the IVT triamcinolone and dexamethasone implant cohorts. Censoring occurred at 180 days after the index date, when a patient left the insurance plan, when a patient received the other form of steroid treatment (dexamethasone implant in the IVT triamcinolone cohort, and vice versa), or when a patient received another form of intraocular steroid. Patients were allowed to have repeat treatments of the same medication up to the 180-day censoring limit. During the running of the model, it was found that the proportional hazards assumption was violated at 40 days post-index date. Therefore, time-varying Cox models were used in the final analysis for analyses of both the primary outcome and the sensitivity analysis outcomes, with results reported as the hazard ratio (HR) for requiring treatment for ocular hypertension over the first 40 days and then separately for days after day 40.
All statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc.). Statistically significant differences were defined as P values (2-tailed) less than or equal to .05.
Results
Figure 1 details the distribution of patients included and excluded based on each criterion used to devise our cohorts. Table 1 shows the baseline characteristics of our patients both before and after inverse probability of treatment weighting of propensity scores. The 2 cohorts showed good balance in all covariates (standardized mean difference <0.1 for each variable).
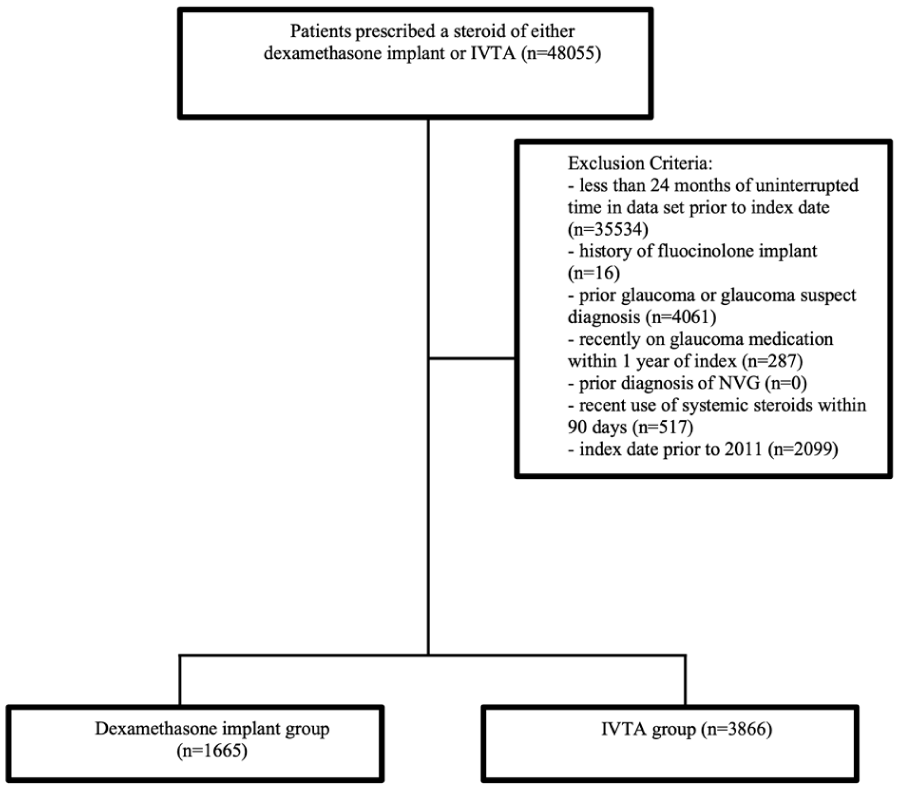
Flow chart showing the distribution of patients in a large US healthcare database who met the inclusion and exclusion criteria for the study and were assigned to receive either intravitreal dexamethasone implant or IVTA injections. Abbreviations: NVG, neovascular glaucoma; IVTA, intravitreal triamcinolone acetonide.
Baseline Characteristics of Patients in Each Treatment Cohort Before and After Inverse Probability of Treatment Weighting of Propensity Scores.
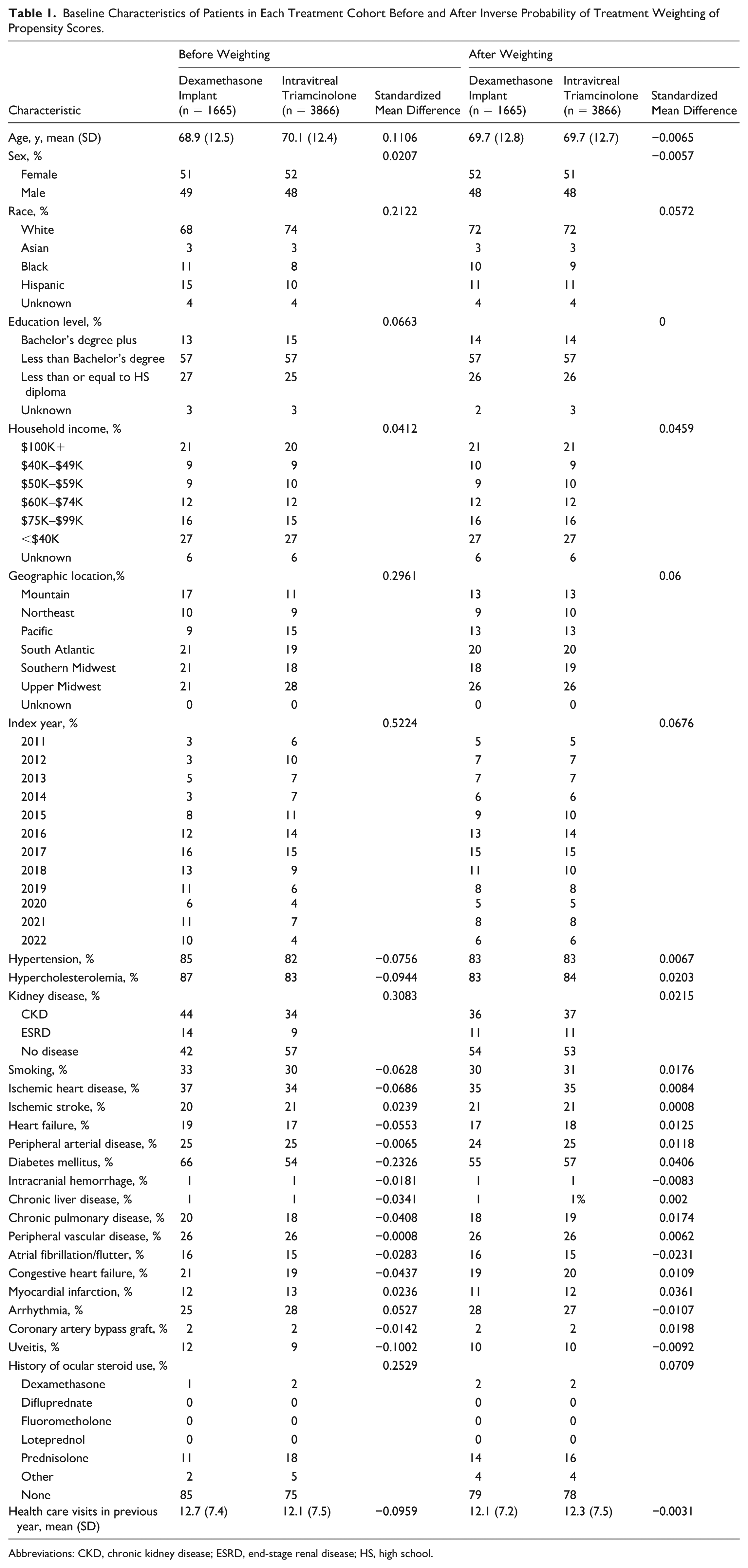
Abbreviations: CKD, chronic kidney disease; ESRD, end-stage renal disease; HS, high school.
A total of 147 (8.8%) of 1665 patients receiving the dexamethasone implant and 282 (7.3%) of 3866 patients receiving IVT triamcinolone injections received medical or surgical therapy for ocular hypertension. A Kaplan-Meier curve for the cumulative probability of requiring ocular hypertension treatment demonstrated a violation of the proportional hazards assumption at 40 days (Figure 2A). The Cox proportional hazards regression analysis for the period of 1 to 40 days showed no significant difference in the risk of requiring ocular hypertension treatment in the dexamethasone implant group compared with the IVT triamcinolone group (HR, 0.77, 95% CI, 0.53–1.12; P = .17) (Table 2). However, analysis after day 40 showed that receiving the dexamethasone implant cohort had an increased risk of requiring ocular hypertension treatment compared with the IVT triamcinolone cohort (HR, 1.41, 95% CI, 1.08–1.86; P = .01).
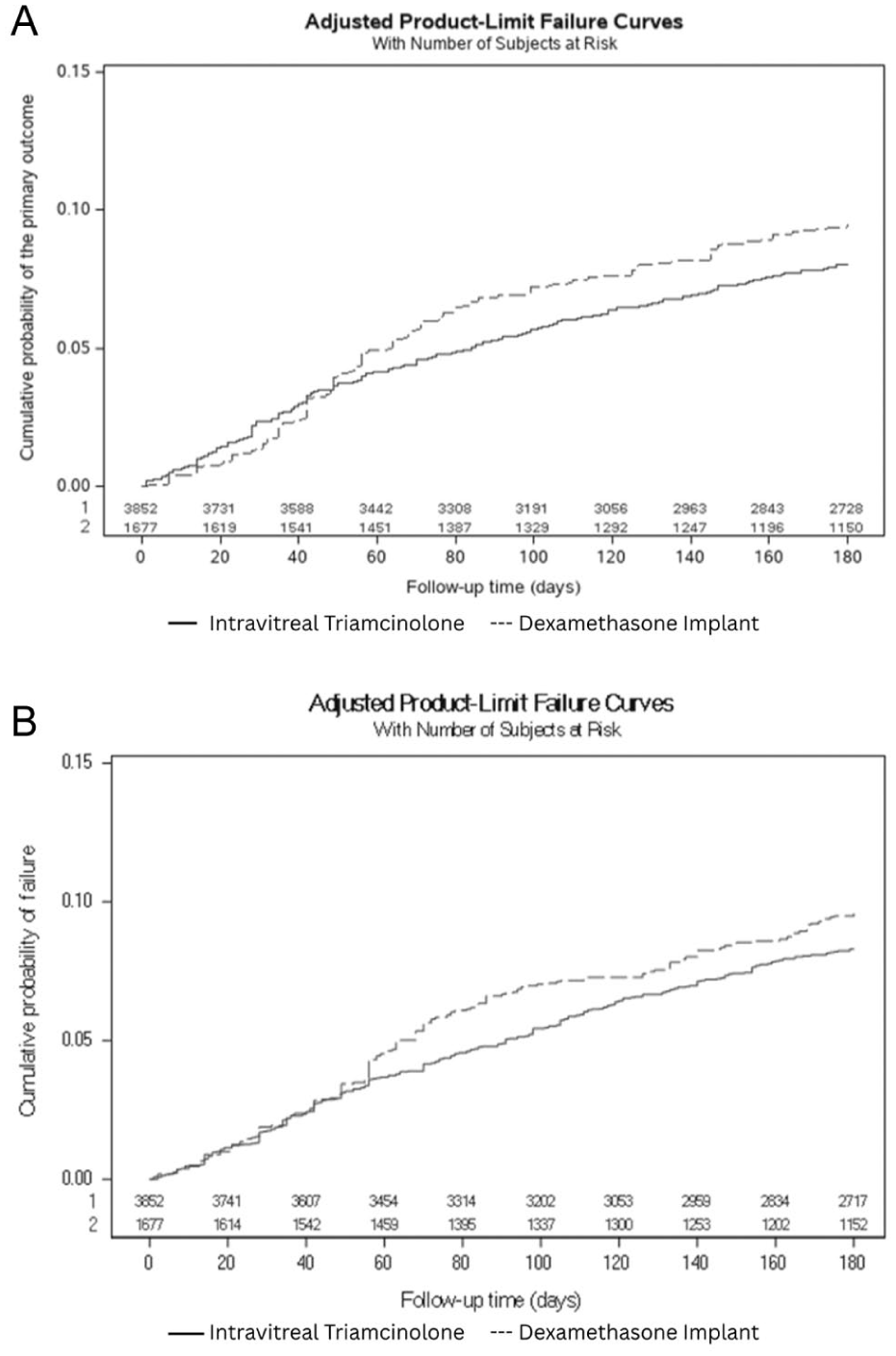
Kaplan-Meier curves showing (A) the cumulative probability of requiring ocular hypertension treatment (the primary outcome), and (B) the cumulative probability of the sensitivity outcome of having a new diagnosis of glaucoma or suspected glaucoma, in patients receiving either intravitreal dexamethasone implant or intravitreal triamcinolone acetonide injections.
Time-Varying Hazard Ratio Multivariate Analysis of Primary Outcome and Sensitivity Analysis.
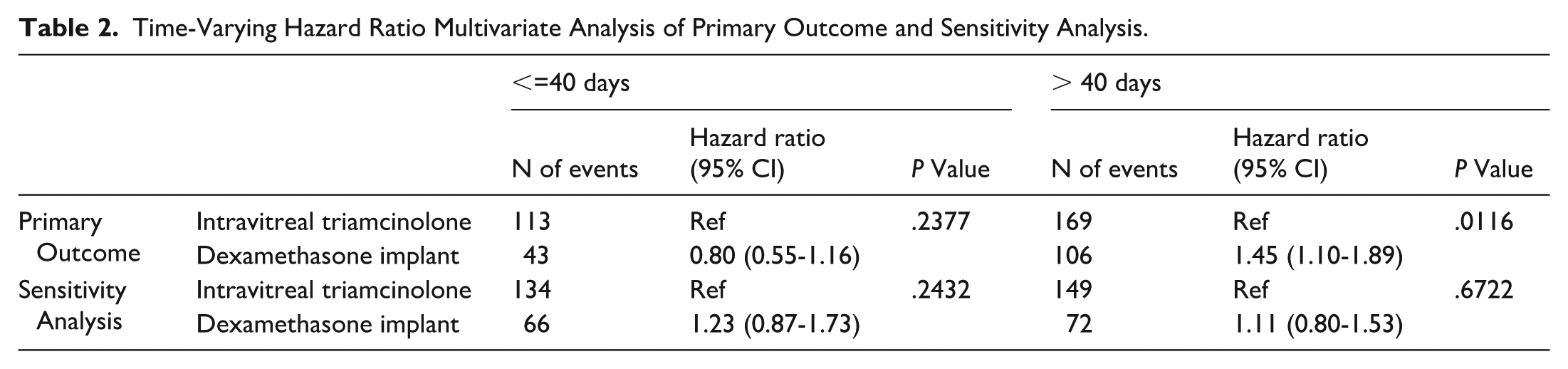
Sensitivity analysis showed that 136 (8.2%) of 1665 patients receiving the dexamethasone implant and 283 (7.3%) of 3866 patients receiving IVT triamcinolone were given a diagnosis of glaucoma or suspected glaucoma. Figure 2B shows the Kaplan-Meier curve for the cumulative probability of the sensitvity outcome. Cox proportional hazards regression analysis showed that the risk of progression to a diagnosis of suspected glaucoma or glaucoma after 40 days postinjection was similar in the dexamethasone implant group compared with the IVT triamcinolone group, but this did not reach statistical significance (HR, 1.24, 95% CI, 0.91–1.70; P = .18).
Conclusions
Our study analyzed real-world data using a large US administrative medical claims database and showed an increased hazard for requiring ocular hypertension treatment 40 days or later after injection in the dexamethasone implant cohort when compared with the IVT triamcinolone cohort. These results contrast sharply with previous studies that have asserted that ocular hypertension was less common in patients receiving dexamethasone implants.1,2 Our study confirms the findings of a small study comparing IVT triamcinolone to dexamethasone implants in vitrectomized eyes. 8
The proportional hazards assumption was violated at 40 days (as shown in Figure 2), thus requiring the Cox regression analysis to be performed with a division at 40 days. While the need to divide the analysis into days 1 to 40 and after day 40 was not preplanned, this timing is consistent with clinical knowledge showing that IOP spikes frequently occur 6 weeks after injection of a dexamethasone implant. 4 Typical practice following an intravitreal steroid injection is for the patient to be seen between 4 weeks and 8 weeks thereafter. One explanation for why the division may have occurred is that some physicians may have given IOP-reducing medications prophylactically at the time of the injection. Indiscriminate prescribing would create the appearance of different glaucoma medication needs during the first 40 days, as compared with physicians who waited to determine which patients were true steroid responders.
Another possible explanation for the increased risk of ocular hypertension in the dexamethasone implant group may be a longer duration of action or greater steroid potency, which may delay the onset of ocular hypertension when compared with IVT triamcinolone.8,9 Although these assertions have not been proven in a direct comparison, even if true, it is important to note that no difference in hazard was noted between the 2 steroid treatments during the first 40 days of the analysis. It is likely that if dexamethasone implant were proven to be more potent, a higher rate of ocular hypertension would be expected, similar to the differences in ocular hypertension rates between the topical steroids difluprednate and prednisolone. 10 It seems less likely that the duration of the medication effects could be attributed to the differences seen in our cohorts. If the timing of peak IOP was the primary cause of the difference in hazard found, then it would be expected that the IVT triamcinolone group would have a higher peak IOP than the dexamethasone implant group in the first 40 days, but that was not seen in our results.
In 2 studies in the literature, 6% to 17% of patients with diabetic macular edema (DME) required treatment with topical ocular hypotensives due to a steroid IOP response from a dexamethasone implant.11,12 In a meta-analysis, 15% to 64% of patients with DME required medical treatment for ocular hypertension secondary to IVT triamcinolone. 2 A smaller minority of patients who failed medical treatment underwent laser trabeculoplasty or surgical intervention. The rates of patients requiring treatment for ocular hypertension in our study (8.9% of patients in the dexamethasone implant group and 7.3% of patients in the IVT triamcinolone group) were within these bounds, although on the lower side of the reported rates of previously published studies. It is possible that the outcome definition that we used may have impacted our results. Other studies have focused on an elevated IOP of ≥25 mm Hg or an increase in IOP of ≥10 mm Hg over baseline, whereas our study relied on the risk of requiring ocular hypertension treatment as the primary outcome. Some physicians may have found an elevated IOP of >10 mm Hg over baseline in their patients, but because of a healthy-appearing optic nerve and an impending drop in IOP with the dissipation of the steroid effect, they may have considered treatment unnecessary. Of note, our results did not appreciably change whether we used ocular hypertension treatments or glaucoma diagnoses as the outcome.
Limitations to our study design need to be acknowledged. First, due to the de-identified nature of the database, we were not able to chart review patient encounters to verify that the correct medication or diagnosis code was documented appropriately. Also, we are unable to verify IOP measurements or specific glaucoma diagnoses; instead we used the proxy outcome of initiating glaucoma medication or having a glaucoma procedure. Specific IOP measurements would be ideal, and these proxy measures have been used previously.5,6 In addition, the data were obtained from a single US-based claims database, which may not be fully representative of trends found outside of the US or US patients without insurance. Furthermore, patients were not offered the 2 treatments in a randomized manner; however, the use of inverse probability of treatment weighting helps to balance the cohorts in baseline characteristics and limit the impact of confounding on our study. Lastly, due to the nature of the data set, we were unable to control for the specific indication requiring the steroid injection; however, we did control for history of uveitis and for history of diabetes at baseline, because these can result in ocular hypertension.
Clinicians need to account for all beneficial and potential adverse effects of the treatments they offer their patients. We found that patients who received dexamethasone implants had an increased hazard of requiring treatment for ocular hypertension compared with patients who received IVT triamcinolone. As more local steroid options become available, direct comparison of the benefits and risks between IVT triamcinolone, dexamethasone implant, fluocinolone acetonide implant, suprachoroidal steroid delivery, and other newer agents should continue to be made.
Supplemental Material
sj-docx-1-vrd-10.1177_24741264261447503 – Supplemental material for Risk of Ocular Hypertension With Intravitreal Triamcinolone Compared to the Dexamethasone Implant
Supplemental material, sj-docx-1-vrd-10.1177_24741264261447503 for Risk of Ocular Hypertension With Intravitreal Triamcinolone Compared to the Dexamethasone Implant by Apoorv P. Chebolu, Yineng Chen, Fangming Jin and Brian L. VanderBeek in Journal of VitreoRetinal Diseases
Footnotes
Author Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical Considerations
The University of Pennsylvania has deemed all projects performed on the Optum database exempt from ethics review due to its de-identified nature. This study follows the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for reporting cohort studies.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University of Pennsylvania Core Grant for Vision Research (grant 2P30EYEY001583). Additional funding was provided by the Metzger Family, Research to Prevent Blindness, and the Paul and Evanina Mackall Foundation. Funding from each of these sources was received in the form of block research grants. None of the funding organizations had any role in the design or conduct of the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Dr. VanderBeek had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Data can be made available through contracting directly with Optum Insights.
Statement of Informed Consent
Informed consent was waived due to the de-identified nature of the data set.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.