
Abstract
Introduction
Intraocular steroids are effective in treating cystoid macular edema (CME) secondary to a variety of diseases, including diabetes, retinal vascular occlusions, and Irvine-Gass syndrome1 –5; however, steroids can be associated with elevated intraocular pressure (IOP). Although the exact pathophysiology is unclear, steroids can result in direct cytotoxicity to the cells of the trabecular meshwork, triamcinolone crystals can cause obstruction of this meshwork, glycosaminoglycans can be deposited, and glucocorticoid receptors can be activated in the trabecular meshwork.6 –10
The risk for steroid-induced glaucoma in the general population is estimated to be 8% to 36%, a risk that increases to 46% to 92% in eyes with primary open-angle glaucoma (POAG). 11 Previous studies have found a higher prevalence of POAG in patients of African ancestry12,13; however, Black patients are underrepresented in clinical trials of glaucoma and other ocular diseases in the United States. 14 In the phase 3 MEAD trials of the 0.7 mg intravitreal (IVT) dexamethasone implant (Ozurdex, Allergan) for diabetic macular edema (DME), only 4.6% of the patients were Black. 15 Only 4% of the patients enrolled in the Ozurdex Geneva study for vein occlusions were Black. 4 In contrast, Black people make up 14% of the US population. 16 Compared with the previous decade, between 2011 and 2020 there were fewer Black participants in diabetic retinopathy (DR) trials, the reasons for which are unclear. 17
Previous studies found some variable treatment responses between different races.18 –20 Black patients with DME had fewer visual improvements after IVT bevacizumab than White and Hispanic patients, even after controlling for baseline vision and hemoglobin A1c. 21 Black race was associated with an increased risk for cataract after CME and prolonged anterior uveitis after combined phacoemulsification with endoscopic cyclophotocoagulation. 22 Black patients with uveitic glaucoma had higher treatment failures with steroids and trabeculectomies. 23 A systematic review by Sharma et al 24 found that preexisting glaucoma and Black race were risk factors for ocular hypertension after keratoplasty, which was related to a steroid response. IVT dexamethasone implants were associated with higher risks for steroid-induced IOP elevations in South Asian and Latino patients than in White patients; however, the study did not include Black patients.
The purpose of the current study was to compare the effects of IVT dexamethasone implants on IOP in Black patients and White patients with DME.
Methods
A retrospective chart review was performed of all patients who received an initial IVT 0.7 mg dexamethasone implant for the treatment of DME at a large retina-only practice between January 2013 and January 2023. Exclusion criteria were no documentation of racial demographics; other etiologies for ME; a history of other IVT steroid injections, including the 0.19 mg fluocinolone acetonide IVT implant (Iluvien, Alimera Sciences) or 0.18 mg fluocinolone acetonide IVT implant (Yutiq, Alimera Sciences); less than 1 year of follow-up; and age younger than 18 years. The Sterling Institutional Review Board waived approval for the retrospective study. The study and data collection were in compliance with the provisions of the US Health Insurance Portability and Accountability Act of 1996, adhered to the tenets of Declaration of Helsinki, and complied with all country, federal, state, and local laws.
Patient demographics, including age, race and ethnicity, medical history, ocular and surgical history, ocular and systemic medications, IOP, cup-to-disc ratios, previous ocular procedures (including lasers, surgeries, and injections), treatment effects and complications, best-corrected visual acuity (BCVA), and central subfield thickness (CST), were analyzed with Prism software (version 9, GraphPad Software). Patients were grouped into the Black cohort or White cohort based on self-identification and the US Office of Management and Budget’s revisions to the Standards for the Classification of Federal Data on Race and Ethnicity. Patients who declined to report, identified as having multiracial ancestry, identified as Asian, identified as a Pacific Islander, or were of Spanish origin were excluded. The appropriate parametric or nonparametric tests were performed, and statistical significance was set at P < .05. The Snellen BCVA was converted to logMAR notation, with counting fingers VA being equal to 1.88 logMAR (Snellen equivalent, 20/1500), hand motions equal to 2.30 logMAR (Snellen equivalent, 20/4000), 25 light perception equal to 2.70 logMAR, and no light perception or enucleation/evisceration equal to 3.0 logMAR. All mean values are ± SD.
Results
A total of 145 eyes in 118 patients met the inclusion and exclusion criteria, with 69 eyes in the Black cohort and 76 in the White cohort. Table 1 shows the patients’ demographics. The Black cohort had more women and a greater proportion with hypertension. The severity of DR was similar between the 2 groups, with approximately 14% having mild nonproliferative DR (NPDR), 39% moderate NPDR, 9% severe NPDR, 39% proliferative diabetic retinopathy (PDR), and 4% tractional retinal detachments (RDs). Of the 12% of patients who had a previous vitrectomy, approximately 50% had PDR.
Patient Demographics and Medical History at Baseline. a
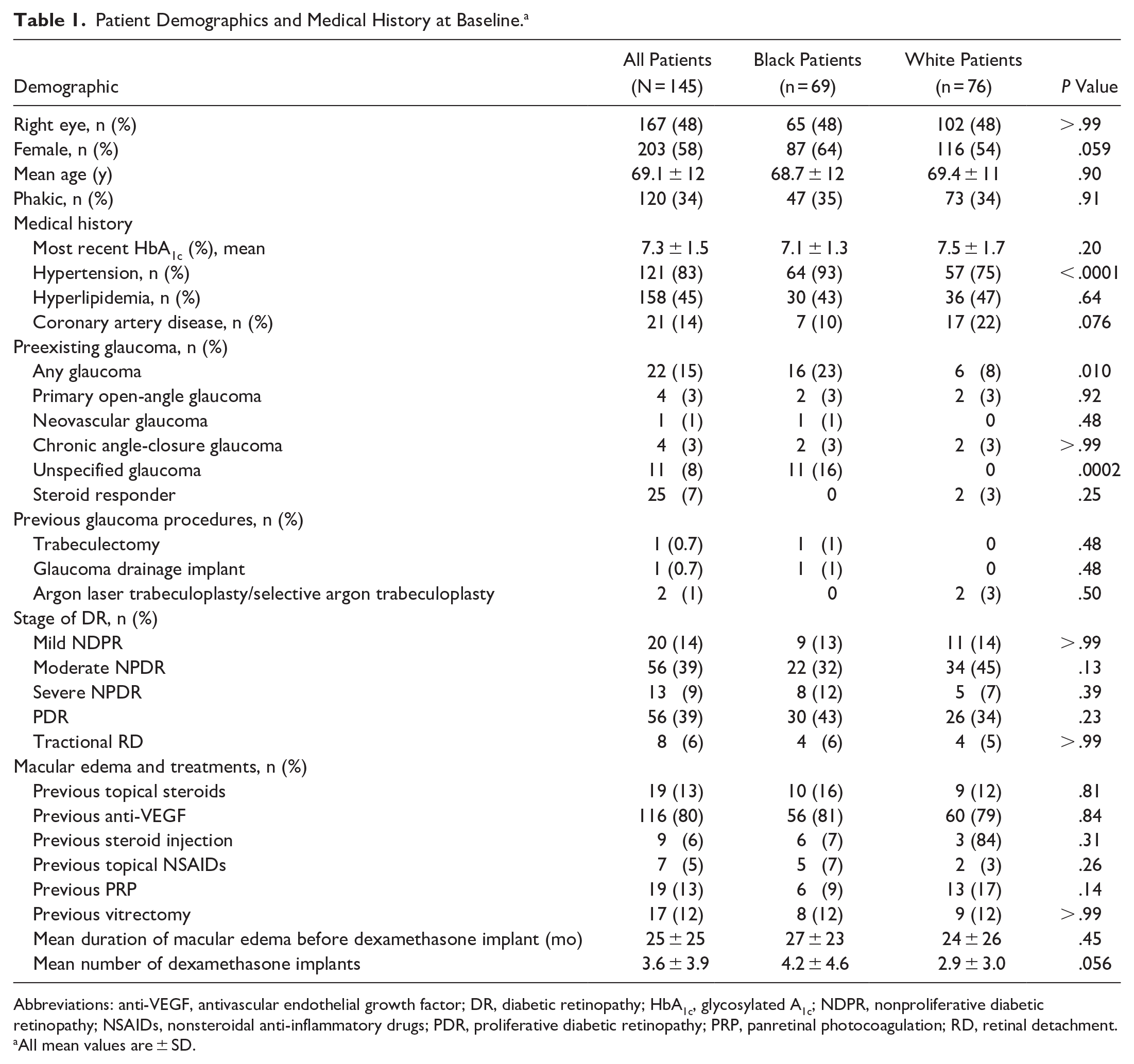
Abbreviations: anti-VEGF, antivascular endothelial growth factor; DR, diabetic retinopathy; HbA1c, glycosylated A1c; NDPR, nonproliferative diabetic retinopathy; NSAIDs, nonsteroidal anti-inflammatory drugs; PDR, proliferative diabetic retinopathy; PRP, panretinal photocoagulation; RD, retinal detachment.
All mean values are ± SD.
Table 2 shows the initial and final examination findings. Black patients had slightly higher baseline cup-to-disc ratios than White patients, were more likely to have preexisting glaucoma (23% vs 8%; P = .010, Fisher exact test), and used more glaucoma drops at the initial visit (mean. 0.54 ± 1.0 vs 0.10 ± 0.4; P = .0012, Mann-Whitney test). The number of previous glaucoma surgeries was similar between the 2 cohorts.
Comparison of Initial and Final Examination Findings. a
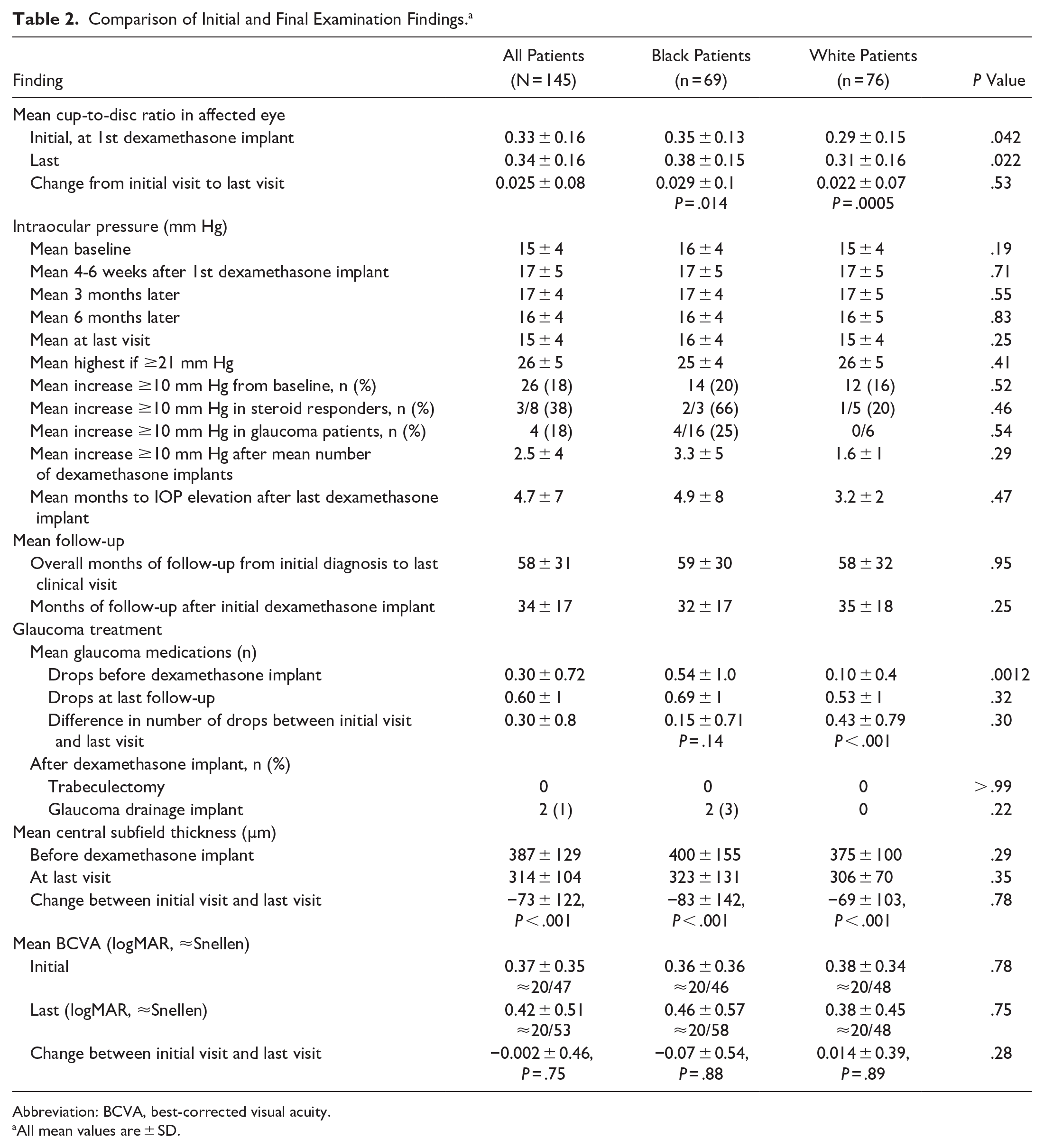
Abbreviation: BCVA, best-corrected visual acuity.
All mean values are ± SD.
Of the eyes, 26 (18%) developed IOP elevations of 10 mm Hg or more above baseline during the study; the proportion was similar between Black patients and White patients (P = .52, Fisher test), regardless of whether the patient had a history of steroid response or underlying glaucoma. The Black cohort and White cohort had a similar number of IVT dexamethasone implants before experiencing IOP elevations (mean, 3.3 ± 5 vs 1.6 ± 1; P = .29, Mann-Whitney test), similar times to IOP elevations after the last dexamethasone implant (mean, 4.9 ± 8 months vs 3.2 ± 2 months; P = .47), and similar maximum IOPs above baseline (mean, 26 ± 5 mm Hg vs 25 ± 4 mm Hg; P = .52). The cup-to-disc ratio increased slightly in both cohorts over the course of the study; however, the change was similar in the 2 cohorts (Table 2).
Black patients used more glaucoma drops at baseline than White patients (0.54 ± 1.0 vs 0.10 ± 0.4; P = .0012); however, the 2 cohorts had a similar number of drops by the last follow-up (P = .32) and similar initial and final IOPs (P = .69). Two Black patients (1%) had incisional glaucoma surgery after IVT dexamethasone implant placement; however, the difference between the 2 cohorts was not statistically significant (P = .22) (Table 2).
Both cohorts had a significant and similar improvement in the CST over the course of the study (387 ± 129 µm initially to 314 ± 104 µm at the last visit; P < .001, Mann-Whitney test); however, there was no race-based difference. Overall, there was no statistically significant difference in BCVA between the initial visit and final visit (0.37 ± 0.35 logMAR vs 0.42 ± 0.51 logMAR; P = .64), regardless of lens status (P = .98) (Table 2). The rates of adverse events, including RDs (3% Black cohort, 1% White cohort; P = .61), were similar between the 2 cohorts.
Conclusions
IVT dexamethasone implants are effective in decreasing ME. They suppress inflammatory mediators and reduce angiogenesis and vascular permeability. Patients may develop elevated IOP, primarily from increased outflow resistance. 26
The current study found that although Black patients had higher baseline and final cup-to-disc ratios and slightly higher baseline IOPs than White patients, there was no statistically significant difference in the percentage who developed ocular hypertension after dexamethasone implant placement. Approximately 18% of our patients had IOP elevations, with 1% requiring incisional glaucoma surgery. In comparison, the MEAD 3-year follow-up study found that 28% of patients developed IOP elevations of 10 mm Hg or more above the baseline, with 1.2% requiring glaucoma surgery or laser treatment. 27 Similarly, the SAFODEX study found that 33% of patients developed IOP elevations, with 1.2% requiring filtering surgery. 28 The CHROME study reported that 21% to 24% of patients developed IOP elevations of 10 mm Hg or higher, with 9% to 29% requiring IOP-lowering therapy. 29
Similar to findings in previous studies, there were baseline differences in systemic and ocular comorbidities in our study, with the Black cohort being more likely to have hypertension and glaucoma.13,30 –33 Although Black patients used more glaucoma drops initially, the 2 cohorts used a similar number of glaucoma drops by the last follow-up visit, with similar final IOPs and similar cup-to-disc ratios.
Some studies have found that patients with POAG may be more likely to have IOP elevations with steroid use, with 20% to 40% of patients having a history of steroid response. 34 The phase 3 clinical trials of dexamethasone implants excluded patients with known histories of steroid response or glaucoma. 27 In the current study, 15% of patients had preexisting glaucoma and 7% had a known history of ocular hypertension after steroid use; fortunately, these patients were not more likely to develop a steroid-induced IOP elevation.
The CST improved significantly in both cohorts. The mean CST improvement of −73 ± 122 µm was less than the −127 µm change reported in the MEAD trial, which may reflect that the patients in the current study had more severe and chronic DR, had persistent DME that was previously treated with more antivascular endothelial growth factor injections, may have had epiretinal membranes, and may have reached a treatment plateau.
Previous studies have noted visual improvement after IVT dexamethasone implant placement5,15,29; however, the current study did not. The discordance between CST improvement and a lack of visual improvement was also noted in the post hoc analysis of DRCR Protocol T, in which Black patients tended to have lower visual gains despite greater reductions in CST. 35 The incongruity likely reflects the underlying effects of chronic ME, macular ischemia, chronic inflammation, and possible concurrent glaucomatous optic neuropathy. 21
The limitations of the current study include its retrospective nature and lack of ancillary glaucoma testing. Additional diagnostics, such as corneal pachymetry, optical coherence tomography (OCT) of the retinal nerve fiber layers, and OCT angiography of the peripapillary vascular density and visual fields, were not performed; thus, early glaucoma changes may have been undiagnosed. 36 The majority of IOPs were obtained with automated handheld tonometers (TonoPen, Medtronic), which may have underestimated the IOP at higher values compared with Goldmann applanation tonometer values37,38; however, elevated IOPs were typically confirmed with applanation tonometry.
In addition, patients were grouped according to their self-identified race; however, many patients were excluded because their race was not specified or they were from multiracial backgrounds. People of Asian or Spanish origin were excluded because of the relatively smaller samples. Race is a social, not a biological, construct, and racial associations may be related to socioeconomic health inequities. 39 Although there was no statistically significant difference in the mean number of IVT dexamethasone implants between cohorts, there was a trend toward Black patients receiving more steroids, which may reflect a sampling bias.
In conclusion, IVT dexamethasone implants were effective in decreasing the CST; however, 18% of patients developed IOP elevations. Fortunately, most cases of ocular hypertension could be managed medically, and only 1% of patients required incisional surgery. Although in the current study, Black patients were more likely than White patients to have preexisting glaucoma, there did not appear to be a statistically significant difference in the risk for steroid-induced ocular hypertension. Larger prospective studies with ancillary glaucoma testing in more diverse patient populations would be needed to detect more subtle changes.
Footnotes
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information were performed in a US Health Insurance Portability and Accountability Act–compliant manner.
Statement of Informed Consent
Informed consent was obtained before the procedure was performed.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.