
Abstract
Introduction:
Conflict between nurses and doulas can contribute to miscommunication, delays in treatment, and decreased patient satisfaction, especially among marginalized populations. Nurses and doulas both play essential roles in supporting birthing individuals, yet their interactions are often strained by unclear role boundaries, differing philosophies of care, and institutional policies that fail to integrate doulas into clinical teams. The purpose of this study is to examine the underlying sources of tension between nurses and doulas and identify facilitators that support more effective collaboration within maternity care teams.
Methods:
We conducted semi-structured interviews with 20 participants (9 nurses and 11 doulas) recruited from both clinical and community settings in South Carolina. Interviews were analyzed using thematic analysis to identify barriers and facilitators to nurse-doula collaboration in maternity care.
Results:
Three key themes emerged: (1) lack of institutional recognition and role legitimacy (structural conditions), (2) territorialism and perceived competition in shared care spaces (interpersonal dynamics), and (3) blurred boundaries between advocacy and scope of practice (role-level influences). Participants also identified strategies to enhance collaboration, including clearer role definitions, institutional support, and mutual respect.
Discussion:
Findings underscore structural, interpersonal, and role-level barriers to nurse-doula collaboration. Integrating doulas into maternity care teams through inclusive hospital policies, joint training, and explicit role clarification may improve teamwork and advance equitable, patient-centered care.
Health Equity Implications:
Strengthening nurse-doula collaboration is a critical step toward addressing the U.S. maternal health crisis, particularly for marginalized communities. Integrating doulas more fully into maternity care teams can promote equitable, patient-centered care and reduce avoidable disparities.
Introduction
Over the past 20 years, national data have consistently shown that the United States is facing a persistent and worsening maternal health crisis. 1 Unlike other high-income countries where maternal outcomes have improved, maternal mortality and morbidity rates in the United States have either stagnated or increased, particularly among groups who experience systemic barriers to high-quality care, including Black and Indigenous birthing people, rural residents, and those facing economic marginalization. 2 These disparities do not reflect inherent vulnerability but rather the effects of structural inequities, historical exclusion from research, and unequal access to respectful, evidence-based perinatal care. 3 Non-Hispanic Black mothers bear the brunt of this crisis, experiencing maternal mortality rates that are three to four times higher than those of their White counterparts. 4 These disparities are not solely the result of individual health behaviors or socioeconomic differences but are deeply rooted in structural racism, chronic underinvestment in communities of color, and unequal access to high-quality, respectful maternity care. While doula care has the potential to mitigate systemic challenges by providing advocacy, culturally responsive support, and continuous care, many doulas remain insufficiently integrated into the health care system, limiting their capacity to advance equity. In this study, we operationalize health equity as care that is responsive to the diverse needs of all birthing individuals and results in equitable outcomes, free from disparities. Without coordinated action across clinical, community, and policy levels, inequities in maternal health will persist, continuing to harm generations of birthing people and families.
During a birth in a hospital setting, mothers are cared for by nurses who are licensed health care providers responsible for medical monitoring, clinical assessments, and interventions during labor and postpartum care. Nurses are integral members of the health care team, working within hospital protocols and evidence-based clinical practices. Complementing this clinical role can be the presence of a doula who offers nonmedical support to birthing individuals and their families before, during, and after birth.
Doulas play a distinct and essential role in maternity care that is grounded in continuous advocacy and emotional and informational support for birthing people. 5 Rather than serving as a substitute for nursing care or a mechanism to offset clinician workload, doula care is rooted in a model that prioritizes autonomy, agency, and person-centered support throughout the perinatal period. 6 Unlike nurses and other health care workers who must balance multiple patients, documentation requirements, and institutional responsibilities, doulas are uniquely positioned to offer uninterrupted, individualized care aligned with the birthing person’s preferences, cultural context, and evolving care needs. A 2022 national policy analysis describes doula care as essential contributors to respectful and equitable maternal care, particularly for those who face systemic barriers, discrimination, or a history of medical mistrust. 7 As research continues to demonstrate that doula support improves satisfaction, reduces unnecessary interventions, and strengthens informed decision-making,8–13 ongoing efforts focus on integrating doula care into maternity systems not as a supplement to clinical gaps, but as a care model that affirms dignity, empowerment, and holistic support during childbirth.
Doulas can also help reduce the sense of burnout in nurses by tending to patients’ basic needs, which is particularly beneficial when nurses are caring for multiple patients, as it alleviates the sense of guilt associated with limited personal attention and ensures that patients still receive individualized care. 14 When working collaboratively, nurses and doulas have the potential to significantly improve the quality and experience of care for birthing individuals. 15 However, the lack of a standardized model for integrating doulas into maternity care teams has resulted in inconsistent collaboration and communication, which are challenges that health care systems are only beginning to address. 16
Although doulas and nurses share a goal of supporting safe, positive birth experiences, research has documented tension or misalignment in how each group conceptualizes their role in labor support. 17 Differences in scopes of practice, care philosophies, and positions within the health care hierarchy can create power dynamics that disrupt collaboration and affect the quality of care provided to birthing individuals. 18 Professional conflicts often arise from unclear role boundaries, communication breakdowns, and rigid institutional hierarchies. 17 Building relationships rooted in mutual respect is essential to overcoming these barriers and achieving better outcomes. 19 Research suggests that nurses may view doulas as outsiders to the clinical care team, leading to challenges in communication, power dynamics, and care coordination. 18 Similarly, doulas report feeling dismissed, overlooked, and excluded in the clinical setting, which can restrict their ability to provide emotional advocacy and support to their full scope.20,21 However, despite growing evidence documenting these interpersonal and structural tensions, there remains limited qualitative exploration specifically focused on the lived experiences of nurses and doulas navigating shared care environments. Few studies center the relational aspects of this dynamic or examine how these tensions intersect with institutional culture, racialized hierarchies, and power structures within maternity care. This gap underscores the need for deeper inquiry into how role boundaries are understood, negotiated, and contested and how these dynamics ultimately shape the birthing environment.
In the context of persistent maternal health inequities, reimagining perinatal care requires moving beyond siloed professional roles toward collaborative, equity-centered models that value diverse forms of expertise. Doulas have increasingly been recognized as critical contributors to respectful, culturally responsive maternity care, yet their integration into hospital-based systems remains inconsistent. Examining nurse-doula relationships offers a unique opportunity to interrogate how dominant biomedical models structure authority, legitimacy, and collaboration—and how these structures might be reimagined to better support birthing individuals, particularly those from historically marginalized communities.
This study contributes to efforts to reimagine perinatal care by centering the perspectives of nurses and doulas to identify not only sources of tension but also pathways toward more collaborative, equitable models of maternity care. The purpose of this study is to examine the underlying sources of tension between nurses and doulas and identify facilitators that support more effective collaboration within maternity care teams. By examining these barriers and facilitators, this research highlights opportunities to strengthen interdisciplinary teamwork, support the integration of clinical and community-based doulas, and advance more coordinated, equity-focused maternity care systems.
Methods
We conducted a focused qualitative descriptive study, a methodological approach well-suited for exploring how nurses and doulas experience collaboration, role boundaries, and sources of tension within hospital-based maternity care. 22 We led a series of key informant interviews from March to April of 2025 with doulas and nurses working in labor and delivery units across South Carolina to get a broad understanding of their working relationships, the barriers and facilitators to implementing an interdisciplinary team-based approach to maternity care, and the perceived needs for improving collaboration. A semi-structured interview guide, featuring open-ended questions and follow-up probes, was used to explore key topics aligned with the research aim. The interview questions were initially informed by preliminary themes identified through a review of the existing literature on nurse-doula relationships, collaboration, and role tension,18,23,24 as well as informal discussions with nurses and doulas and the primary author’s lived experience as a labor and delivery nurse, which highlighted common sources of tension and areas of collaboration. These questions served as a starting framework; however final themes were refined and developed through analysis of the interview data. The study was considered exempt by the Institutional Review Board at the corresponding author’s institution.
Participants and Procedures
A diverse sample of doulas and nurses working in labor and delivery units who had at least 1 year of experience within the last calendar year were recruited through purposive and snowball sampling approaches. For the purposes of this article, the term “nurses” refers to labor and delivery nurses working within hospital settings. We collaborated with community-based doula organizations, doula collectives, and nursing organizations to recruit interview participants who represented perspectives across different health care settings and who had an understanding of maternity health service implementation. Recruitment concluded when the planned sample size of 20 participants was reached based on available project resources and study scope rather than thematic saturation. Emerging themes were monitored during data collection to ensure adequate variation in perspectives across participants. Interviews were about an hour, and participants were given a $50 e-gift card as an honorarium for their time. We obtained and reaffirmed informed consent prior to beginning each interview. Interviews were conducted via a video conference platform, Zoom, audio recorded, and transcribed verbatim. All interviews were conducted by the primary investigator (C.T.), who has lived experience as a labor and delivery nurse, and a trained co-investigator (M.M.), both with experience in qualitative interviewing. Participant demographic data were self-reported and collected at the conclusion of the interview.
The research team consisted of a primary investigator with previous labor and delivery bedside nursing experience, two co-investigators with expertise in qualitative descriptive design, a co-investigator with bedside labor and delivery bedside nursing experience, a co-investigator with expertise in perinatal epidemiology, and an undergraduate research assistant.
Analysis
Interviews were analyzed using an inductive thematic approach. 22 We conducted iterative reviews of the data to allow key themes or ideas to emerge and then used qualitative data analysis software (Dedoose) to code data and organize the analysis. All interviews were transcribed and analyzed using open coding techniques. Two research team members independently reviewed an initial set of interview transcripts. After individual review, the team met to discuss and compare interpretations of initial themes and emergent codes. After resolving differences in interpretations, a list of themes to focus the analysis was developed. A codebook was organized around those emergent themes. Coding disagreements were resolved through iterative discussion to refine and finalize the codebook. The research team engaged in reflexive practices throughout the study to account for positionality and potential bias. Because no members of our research team had experience working as a doula, reflexive memoing and team-based coding were used to ensure interpretations remained grounded in participant perspectives rather than researcher assumptions.
Results
Sample
A total of 20 key informant interviews were completed with doulas (n = 11) and nurses (n = 9) working in labor and delivery units in South Carolina (Table 1). All participants identified as female. Across both groups, most participants identified as non-Hispanic Black or African American, and a smaller proportion identified as non-Hispanic White or Hispanic or multiracial. The majority of participants were between the ages of 25 and 34, with fewer participants in older age groups. Education levels ranged from associate to master’s degrees, with bachelor’s degrees most commonly reported. Years of professional experience also varied, with nearly half (45%) of participants reporting 1–3 years of experience, followed by 40% reporting 4–6 years of experience. Among participating doulas, only one held a formal hospital-employed position, while the remaining doulas worked independently or through community-based organizations.
Participant Characteristics by Role (N = 20)

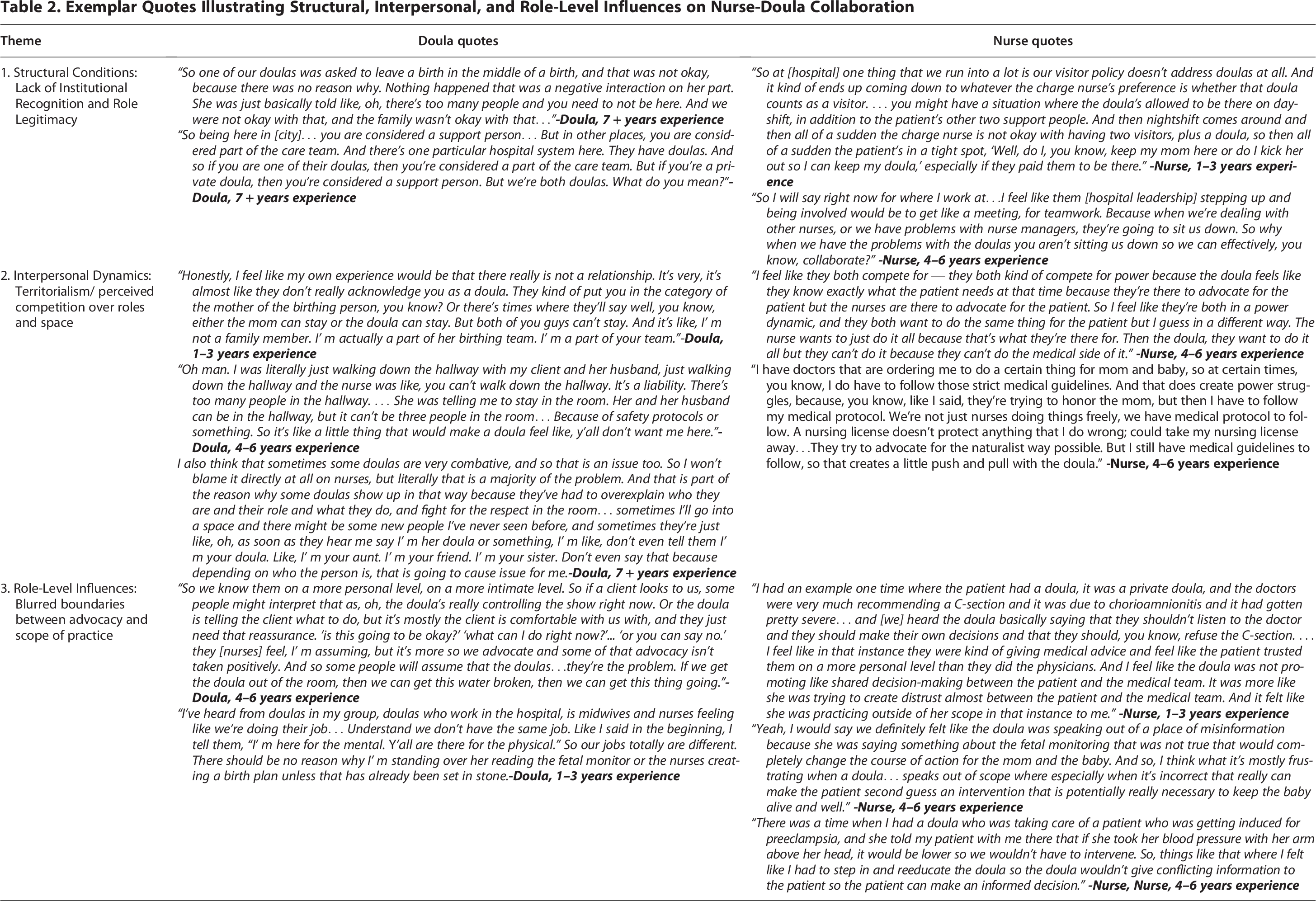
Most nurses stated they occasionally, as much as 2-4x per month, interacted with doulas in their practice. Most doulas in our study were community-based, or non-employed by a health care system, and stated they interacted with nurses only when providing support during the hospital birthing experience of their clients. Through thematic analysis, we identified three unifying themes that reflected multilevel influences on nurse-doula collaboration: (1) lack of institutional recognition and role legitimacy (structural conditions), (2) territorialism and perceived competition in shared care spaces (interpersonal dynamics), and (3) blurred boundaries between advocacy and scope of practice (role-level influences). These themes, illustrated in Figure 1, demonstrate how systemic, relational, and role-specific factors collectively shape the collaborative environment within maternity care settings. Exemplar participant quotes supporting each theme are presented in Table 2.
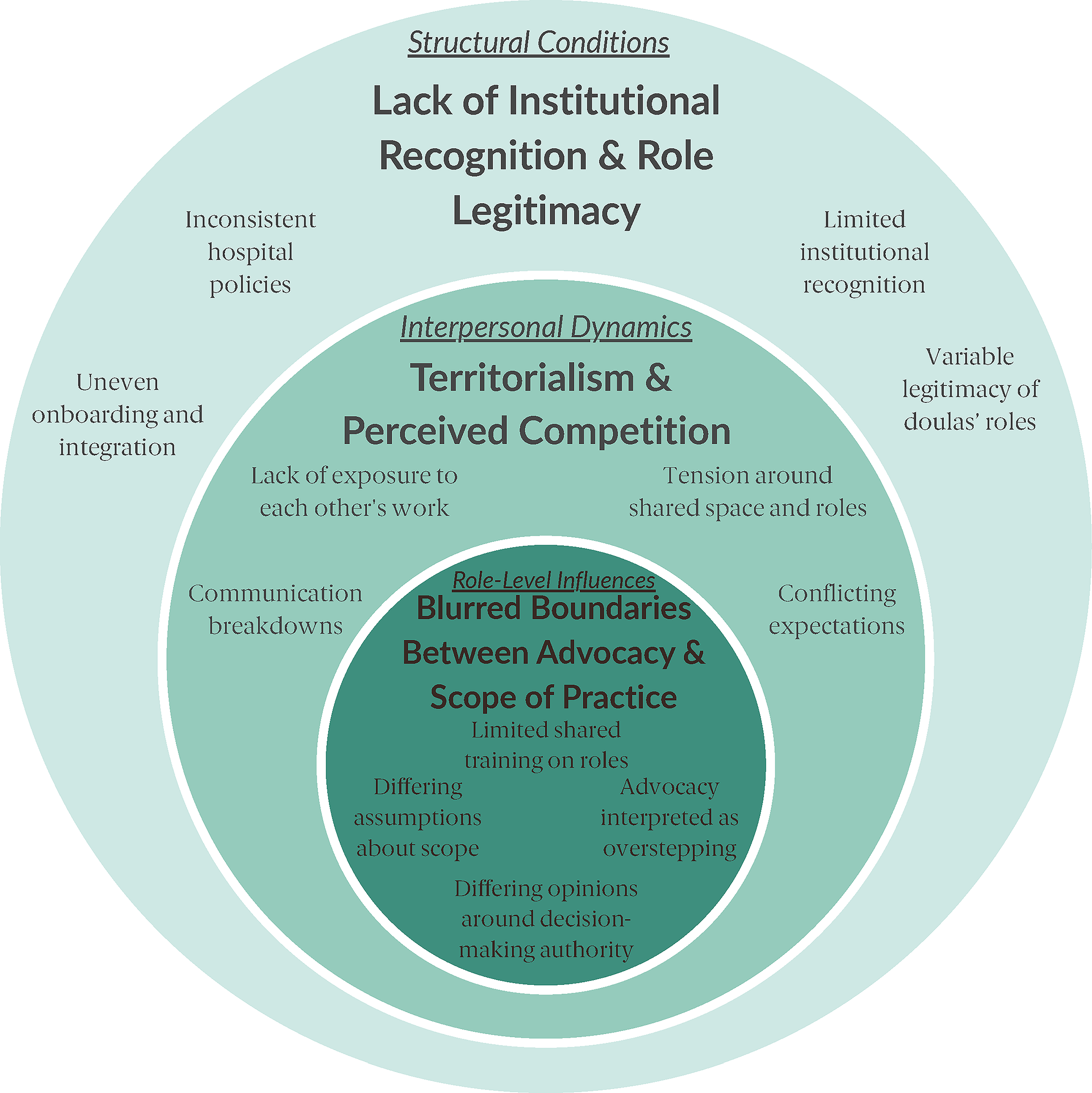
Layered model illustrating structural, interpersonal, and role-level influences on nurse-doula collaboration. The outer circle represents structural conditions, the middle circle reflects interpersonal dynamics, and the inner circle depicts role-level influences related to advocacy and scope of practice. Themes were organized according to the level at which they operate within maternity care settings to show how systemic, relational, and role-specific factors collectively shape nurse-doula collaboration.
Exemplar Quotes Illustrating Structural, Interpersonal, and Role-Level Influences on Nurse-Doula Collaboration
Theme 1: Lack of institutional recognition and role legitimacy
Participants described how institutional structures such as hospital policies, employment arrangements, and leadership practices shaped doulas’ recognition and legitimacy within maternity care teams. They described how doulas’ status within hospital systems is often unclear or inconsistent, shaping whether they are treated as part of the care team or as visitors. This ambiguity influenced collaboration and contributed to feelings of marginalization among doulas. One nurse contrasted her experiences with hospital-employed and community-based doulas: “I feel like the relationship at [our hospital] is amazing with our doulas that are employed by the hospital. I feel like they respect us and what we do, and we do the same to them. There’s a lot less tension. As for private doulas, I feel like there’s typically more tension and not always as much respect both ways.”-Nurse, 4–6 years’ experience. Some doulas described working hard to establish themselves as legitimate members of the care team despite not being medical providers. One doula explained: “I’ve kind of established my own relationships with each and every one of them, and so it’s good. It’s good collaborating… I’m a non-medical worker, but I am a part of the care team.”-Doula, 7 + years’ experience.
At the same time, doulas shared that in many settings they are still treated primarily as support people rather than recognized contributors to care. For example, some described needing special permission to access the unit, waiting in public areas until staff decided whether they could enter, or being limited by visitor policies that did not explicitly account for doulas. One doula recounted an experience during an obstetric emergency that highlighted how institutional policies, and the absence of clear role designation, shaped her exclusion from care processes, “The baby’s heartrate dropped, and then all of a sudden she’s [the nurse] like, “Oh, so we’re gonna have to do an emergency C-section.” And they didn’t interpret, you know, they didn’t really explain to them what was happening. And so, when I was trying to explain it to him, the nurse comes over…and said, “We’re gonna get everything on, we’re going straight to the emergency room.” And … the nurse said to me, “You can go into the waiting room, and visiting hours end at eight.” And I was just, like, “They don’t have an interpreter, give her a minute.” -Doula, 1–3 years experience. Rather than reflecting individual disrespect, these experiences illustrate how institutional policies and practices fail to consistently recognize doulas as part of the maternity care team. Doulas described feeling more replaceable and less protected than clinical staff, particularly in high-acuity situations, reinforcing perceptions that hospital systems had not fully articulated or institutionalized their role within maternity care.
Nurses also acknowledged that hospital leadership had not done enough to create clear structures for nurse-doula collaboration. Several noted that, unlike conflicts between nurses, tensions involving doulas were rarely addressed through formal processes or facilitated conversations. This absence of institutional guidance left collaboration dependent on individual relationships rather than standardized systems, contributing to variability in how doulas were integrated and how legitimate their role was perceived to be.
Theme 2: Territorialism and perceived competition in shared care spaces
Participants described interpersonal tensions related to perceived ownership of the birthing space, particularly when nurses and doulas navigated overlapping responsibilities in supporting laboring patients. Rather than agreement on who should lead, interviews reflected mixed views about authority, legitimacy, and who ultimately directs care in the room. One doula shared, “No one person is in control, but sometimes a lot of people feel like they are in control because they have more education… I do feel that power struggle and that dynamic of ‘I’m the boss here.’” -Doula, 7 + years experience. Another participant reflected, “They think we’re taking over, but no, I want a nurse to still come in and help mom… We can learn from each other, just that collaboration.””-Doula, 1–3 years experience. Similarly, a nurse shared, “Sometimes it’s like they’re trying to run the room, and I’m the nurse. I’m responsible. Someone has to be in charge.” -Nurse, 4–6 years experience.
Importantly, both nurses and doulas described how these interpersonal dynamics were shaped by prior experiences. Participants noted that past negative interactions could heighten defensiveness or suspicion in future encounters, while positive relationships built over time tended to reduce competition and foster trust. Several participants described “reading the room” early in an interaction to determine how collaborative the relationship might be.
Participants also explained that when territorial tension occurs, the birthing person feels it, and the emotional environment shifts. One doula said, “Birth and labor… are sacred. Moms have to be comfortable, reassured, relaxed. When that can’t happen, the experience becomes negative—not just the outcome, but the whole experience of being there.” -Doula, 4–6 years experience. Nurses similarly described that when collaboration is intact, patients benefit: “When we’re all on one page, everyone has a role… the client feels the care from your nurses, your doula, your doctor… she would feel protected and understood on every angle.””-Doula, 1–3 years experience.
Together, these accounts illustrate how territorialism operates as an interpersonal process, shaped by perceptions, communication, and relational history. When competition for authority or control surfaced, collaboration deteriorated; when mutual respect and trust were established, nurses and doulas described a more cohesive and patient-centered care experience.
Theme 3: Blurred boundaries between advocacy and scope of practice
Participants described role-level tension rooted in differing interpretations of advocacy, professional scope, and decision-making authority. Across interviews with both nurses and doulas, participants highlighted how unclear role boundaries, particularly during moments of patient advocacy, could be misinterpreted as overstepping or undermining clinical care.
Some doulas expressed that in the process of advocating for their clients, it can be interpreted by nurses that they are talking “for” the patient. Generally, most community-based doulas have a long-standing relationship with their patients that typically begins early in the prenatal period, whereas hospital-employed doulas are assigned to patients at admission. In the end, their roles encompass both advocacy and support. Many times, when there is a pre-existing relationship, the patients communicate their preferences ahead of time to their doula and rely on the doula to be their voice. A doula explained, “So we know them [the client] on a more personal level. So, if a client looks to us, some people might interpret that as, oh, the doula’s really controlling the show right now. Or the doula is telling the client what to do, but it’s mostly the client is comfortable with us, and they just need that reassurance.” -Doula, 4–6 years experience. Several doulas noted that their clients often struggle to interpret the medical terminology nurses use and therefore look to the doula to help them understand. Doulas explained that while nurses may see this as the patient asking the doula to give a second opinion on the medical care, they are only helping the client interpret what is being said. Nurses, on the other hand, said that advocacy can be seen as “undermining” the medical advice, especially during emergencies, and minimizing the urgency of the situation thus also contributing to tension and leaving the patient unsure as to who to trust. A nurse stated, “…because now [the doula is] telling the mom, ‘They’re going to give you an unnecessary intervention.’ And again, they have that trust factor with the doula, so they’re looking at us like what she’s saying is right, because I’ve talked to her, I trust her, I know her. So, it does undermine us.” -Nurse 4–6 years experience.
Some nurses described instances where doulas acted outside of their perceived scope of practice, for example, offering clinical recommendations or contradicting medical guidance, which they felt complicated communication and care coordination. One nurse shared: “There was a time when I had a doula who was taking care of a patient who was getting induced for preeclampsia, and she told my patient with me there that if she took her blood pressure with her arm above her head, it would be lower so we wouldn’t have to intervene. So, things like that where I felt like I had to step in and reeducate the doula so the doula wouldn’t give conflicting information to the patient so the patient can make an informed decision.” -Nurse 4–6 years experience.
Doulas recognize the challenges of the blurred boundaries as well. For example, one doula stated, “I also feel like overarching, they just don’t think a doula is a real job or that you have any value or that you do anything because it’s like, oh, well, I’ m a nurse. Okay, you’re a nurse, but you’re a nurse and you do nursing things, and I’ m a doula and I do doula things. So, your scope of practice is completely different than mine, but I promise you if we work together, I’ m going to make your job so much easier.” -Doula, 4–6 years experience. Another doula said this scope of practice tension is often misinterpreted, “I think that parties can shut down or get really activated about it, become a little—I won’t even say snarky, but sometimes snarky when they’re feeling like ‘Oh, you’re overstepping. I know the medical parts of things. You as a doula don’t know the medical parts of things.’ So, then there’s a defensiveness that sometimes happens.” -Doula, 1–3 years experience.
Nurses noted that doulas aren’t trained in medical decision-making skills. During emergency situations, this can be a barrier to nurses and doulas working together. Nurses also explained that because doulas lack medical training, they don’t always understand or recognize the importance and time-sensitive nature of medical care during emergencies. A nurse explained, “They’re there to support them with their labor process. But sometimes…I feel like in emergent situations, when I look at the holistic model and what’s going on right then and there and [the] baby is not looking great, that they kind of deter the patient a little bit on what is an actual emergency in the hospital.” -Nurse 4–6 years experience. Doulas, however, acknowledged that emergencies heighten emotions and create uncertainty, not only for nurses and doulas, but also for patients and families. One doula explained: “When things are fast and emergent, it’s like just get out of the way, it becomes a medical issue. But sometimes nobody explains anything to the partner either. If a baby’s heart rate drops, suddenly five people rush into the room. My client is anxious, the partner is in shock, and nobody is talking. So, I step in to bridge the communication gap, even though I’ m not a medical person. Once an emergency occurs, it’s like nobody else exists.” -Nurse, 4–6 years experience.
Together, these accounts suggest that tensions surrounding scope of practice stem less from deliberate role violations and more from differing assumptions about advocacy, authority, and responsibility in high-acuity moments. Participants across both groups described parallel intentions to protect and advocate for the birthing person; however, the absence of shared training, explicit role definitions, and opportunities to build mutual understanding made alignment difficult in practice.
Facilitators to Effective Collaboration
In addition to describing sources of tension, participants articulated ways nurse-doula relationships could be reimagined in practice. These reflections did not constitute a separate theme but rather cross-cutting insights that emerged when participants described conditions under which collaboration worked well or could be improved. These recommendations centered on communication practices, shared training, and institutional policy changes to clarify roles and support coordinated care.
A key facilitator was the establishment of structured communication processes that intentionally include doulas in relevant care discussions. Several nurses suggested incorporating doulas into bedside reports so that all parties receive consistent information related to the patient’s care plan, preferences, and changes in clinical status. As one nurse explained, “I feel a bedside report with the doula would be super helpful… if there’s a doula present, they should be part of that conversation.” -Nurse, 4–6 years experience. This approach was seen as a way to reduce confusion, prevent conflicting messaging, and support a unified care experience for the patient.
Participants also emphasized joint learning opportunities as an important facilitator for building trust and clarifying expectations. Nurses and doulas described interdisciplinary simulation training and shared continuing education as opportunities to learn together outside of high-stakes clinical situations. One doula explained that routine opportunities to interact with nurses prior to working together in a patient room could reduce assumptions about competence and scope of practice. She shared, “If we had more regular meetings or simulations together, then when we’re in a real birth we already know each other and nurses wouldn’t assume a doula ‘doesn’t know what they’re doing.’ That’s where a lot of tension comes from.” -Doula, 4–6 years experience. These joint training opportunities were described as critical for fostering mutual respect and relational familiarity.
Beyond interpersonal and educational practices, participants highlighted the role of institutional policies in shaping collaboration. Nurses noted that role ambiguity was often reinforced by inconsistent hospital policies, particularly visitor policies that did not explicitly address doulas. As one nurse described, “Our visitor policy doesn’t address doulas at all… then the patient has to choose between support people and their doula, which isn’t fair, especially if they paid for that support.” -Nurse, 4–6 years experience. Participants described clearer policy language recognizing doulas as part of the care team, distinct from visitors, as facilitating smoother access, reducing confusion, and supporting coordinated care.
Finally, participants identified system-level supports, such as insurance and Medicaid reimbursement for doula services, as facilitating both access to care and professional legitimacy. Doulas described how reimbursement could expand access for families who might otherwise be unable to afford doula support and create pathways for more formal integration into maternity care systems. One doula shared, “There’s been talk about Medicaid covering doulas, and that could make a big difference… a lot of families can’t afford doula support, and coverage could improve outcomes here.” -Doula, 7 + years experience.
Together, these facilitators reflect participants shared descriptions of conditions under which nurse-doula collaboration was more effective. Rather than functioning as prescriptive recommendations, these practices illustrate how communication, shared learning, and institutional support can create care environments where doulas are recognized, supported, and included as collaborative partners—ultimately strengthening interdisciplinary relationships and enhancing patient-centered maternity care.
Discussion
The objective of this study was to examine the underlying sources of tension between nurses and doulas and identify strategies to promote more effective collaboration within maternity care teams. Through semi-structured interviews with key stakeholders, we identified three key themes affecting the nurse-doula relationship: (1) lack of institutional recognition and role legitimacy (structural conditions), (2) territorialism and perceived competition in shared care spaces (interpersonal dynamics), and (3) blurred boundaries between advocacy and scope of practice (role-level influences). Improving collaboration requires not only clearer communication and mutual role understanding but also institutional policies and professional frameworks that acknowledge doulas as legitimate contributors to maternity care. Taken together, these findings suggest that nurse-doula conflict is not simply a matter of interpersonal disagreement but reflects deeper assumptions embedded in dominant models of perinatal care, particularly around authority, expertise, and legitimacy. Reimagining perinatal care through an equity lens requires challenging these assumptions and recognizing collaboration as a structural and relational practice, rather than an individual skill. As illustrated in Figure 1, participants’ experiences highlight how structural conditions, interpersonal dynamics, and role-level boundaries intersect to shape collaboration, underscoring the need for system-level reconfiguration rather than isolated interventions.
Existing literature offers limited but growing insight into nurse-doula collaboration in hospital settings. An online survey of nurses, doulas, and educators across the United States done in 2016 found that more exposure to doulas was analogous to more positive views of doulas by nurses, and when doulas consistently worked in the same hospital system, they had more positive views of nurses. 23 Ballen and Fulcher’s 25 study, which was conducted in the Southeastern United States, was one of the earliest qualitative studies to examine this relationship and identified similar challenges in nurse-doula collaboration described in the present study, including role conflict, professional mistrust, and perceptions that doulas lack legitimacy in clinical environments. Their work emphasized that unclear scope boundaries contributed to tension, yet recommended collaborative models rather than exclusion. Two decades later, our findings suggest that similar tensions remain despite increased visibility of doulas and broader recognition of their benefits for maternal health, particularly among Black and Indigenous birthing people.
Research focused on doula integration with other clinicians, including midwives and physicians, has also documented role ambiguity and variable acceptance in clinical environments. Studies conducted by Adams & Bowen 26 and Burke et al. 21 highlight that doulas are often positioned outside formal care structures, even when evidence demonstrates their positive impact on outcomes such as cesarean reduction, breastfeeding initiation, patient satisfaction, and emotional safety. The persistence of these dynamics suggests that the issue may not be about doulas themselves, but rather about the absence of structural frameworks to support collaborative practice.
Scope of practice surfaced as a central tension in our study, yet very few participants could cite formal institutional language defining the boundaries between roles. This reflects the national landscape: most states do not regulate doula practice, and there is no standardized credentialing body comparable to state boards of nursing. Many states across the United States have implemented Medicaid coverage for doula services, 27 which has prompted discussion about formalizing competencies, role descriptions, and hospital onboarding processes. Early evaluations of these programs suggest that reimbursement alone does not guarantee integration; rather, successful models pair payment policies with structured clinical orientation, ongoing training, and intentional partnerships with community-based doula organizations. These cases demonstrate that institutional support, rather than reliance on individual nurse-doula relationships, may be key to scaling collaboration.
Our findings also suggest meaningful differences in how collaboration unfolds with hospital-employed versus community-based doulas. Several nurses in our sample described smoother interactions with doulas who were employed by the hospital, noting that these doulas often had clearer access to the unit and were more familiar with institutional routines. Although our data does not speak directly to how hospital employment affects doula advocacy, broader conversations within maternity care have raised questions about how employment structures may influence a doula’s autonomy and role expectations. While our study was not designed to compare these models, the perspectives shared by participants indicate that employment structure may shape collaboration, role negotiation, and how doulas are integrated within clinical teams. Future research should examine how different employment models affect both collaboration and advocacy in maternity care settings.
Our findings align with Lyndon, et al. 28 ’s recommendations for improving intrapartum teamwork, including approaching interactions with curiosity and reducing assumption-based conflict. Incorporating models from interprofessional education, such as simulation training, structured communication tools, and standardized role introductions, may support clearer understanding of scope and shared care philosophies. As participants in this study expressed, when doulas and nurses understand each other’s roles and communicate openly, collaborative care is possible and may enhance safety, satisfaction, and patient-centered decision-making.
These findings have important implications for clinical practice, institutional policy, and future research. Hospitals and maternity care systems should continue to invest in formalizing the roles of doulas within the care team by developing clear guidelines for collaboration, offering joint training opportunities, and revising visitor policies to ensure that community-based doulas are not excluded from the birthing space. 29 Medicaid reimbursement and insurance coverage offer an opportunity to institutionalize doula services, but payment must be paired with policy, training, and accountability structures to avoid reinforcing hierarchies or limiting doulas’ autonomy. Future research should evaluate models of successful doula integration within health care teams, such as the HoPE Doula Program for Pregnant People, 30 which is an integrated community doula program in New York City health systems, to determine which approaches foster cultural safety, respectful care, and equity-focused practice. From a reimagining perspective, these findings point toward models of perinatal care that intentionally redistribute authority, formalize collaboration, and center relational care. Rather than positioning doulas as adjunct or optional supports, reimagined models integrate doulas as essential partners whose expertise complements clinical care and advances reproductive justice.
While this study provides rich insight into nurse-doula collaboration, several limitations should be considered. First, participants were recruited from a single state, which may limit generalizability to other clinical or policy environments. Second, while our sample size aligns with standards for qualitative research, our findings are based on self-reported experiences, which may be subject to recall or social desirability bias. Our analytic approach was designed to prioritize depth and richness of data, consistent with established qualitative methodologies. 31 Finally, the perspectives of birthing individuals themselves were not included, which limits our understanding of how nurse-doula dynamics affect the patient experience directly. Future studies should consider including patient voices and exploring institutional-level perspectives to further contextualize the findings. Another limitation is that all doulas in our sample identified as Black or African American, and only one hospital-employed doula participated. This limits the transferability of findings to more diverse doula populations or settings where doulas are integrated into hospital systems. Future studies should explore how racial identity and employment model influence nurse-doula collaboration.
Conclusion
This study provides critical insight into the structural, interpersonal, and role-level dynamics shaping collaboration between nurses and doulas in maternity care. A lack of institutional recognition and role legitimacy (structural conditions), territorialism and perceived competition in shared care spaces (interpersonal dynamics), and blurred boundaries between advocacy and scope of practice (role-level influences) emerged as key sources of tension. Together, these findings demonstrate how challenges in nurse-doula collaboration are produced not only through individual interactions, but through layered systems, relationships, and role expectations. These challenges reflect broader gaps in U.S. maternity care, where fragmented care models and inequitable access continue to contribute to preventable disparities in maternal health outcomes.
Our findings underscore that improving nurse-doula collaboration is not solely a matter of interpersonal rapport but a structural and organizational imperative. Meaningful integration of doulas into maternity care teams has the potential to strengthen communication, enhance patient-centered decision-making, and reduce inequities, particularly for Black birthing people and other communities disproportionately affected by the maternal health crisis. As health systems explore models such as Medicaid reimbursement, hospital-based doula programs, and interprofessional training, intentionally centering doula perspectives and formalizing collaborative structures will be essential.
Reimagining perinatal care to consistently include doulas as valued partners can advance reproductive justice and foster maternity care environments where all birthing individuals receive respectful, culturally responsive, and continuous support. Achieving this transformation will require coordinated efforts across structural, interpersonal, and role-level domains, including clearer role definitions, shared training frameworks, and institutional policies that recognize doulas as integral contributors to maternity care.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board at the University of South Carolina. All methods were carried out in accordance with relevant guidelines and regulations to ensure the protection of participants, including gathering informed consent for each individual.
Availability of Data and Materials
The data generated and analyzed during the current study are not publicly available to protect the privacy of those interviewed. The survey was developed specifically for this study. The full survey is available upon author request.
Authors’ Contributions
C.T.: Conceptualization (lead); methodology (lead); investigation (lead); formal analysis (lead); data curation (lead); writing—original draft (lead); writing—review and editing (equal); supervision (lead); project administration (lead); funding acquisition (lead). M.M.: Conceptualization (supporting); methodology (equal); investigation (equal); formal analysis (equal); data curation (equal); writing—original draft (equal); writing—review and editing (equal). K.R.: Writing—review and editing (equal). N.B.: Writing—review and editing (equal). R.G.: Formal analysis (equal); writing—review and editing (equal). L.W.: Methodology (equal); writing—original draft (equal); writing—review and editing (equal). All authors have read and approved the final article. Each author meets the criteria for authorship and agrees to be accountable for their contributions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was funded by the NIH Common Fund through the Office of the Director, National Institutes of Health (OD) and under Award Number U54CA272171.