
Abstract
Background:
Involving husbands in maternal and child health programs can reduce maternal morbidity and mortality. The study aimed to analyze the factors related to the husband’s involvement in antenatal care (ANC) visits in Indonesia.
Methods:
The study was a cross-sectional study. The research employed secondary data from the 2017 Indonesian Demographic and Health Survey. The analysis units were wives aged 15–49 years old, married, and pregnant in the past 5 years, and the final samples obtained were 14,319 respondents. In addition to the husband’s involvement were residence, age, education, occupation, wealth, and parity. The study used a binary logistic regression test in the final stage.
Results:
Husbands who lived in urban areas have odds of being involved in ANC visits 1.2 times greater than those in rural areas. The better the husband’s education was, the more involved they were in ANC. The results show husbands who work in any field were better at being involved in ANC. Poorer husbands had odds of being engaged in ANC visits 2.0 times more likely than the husbands’ lowest group. The most prosperous husbands have odds of being involved in ANC visits 5.4 times than the poorest husbands. The husbands’ wealth is better, the more the husbands were engaged in ANC. The more children were born, the less frequent the husbands’ involvement in ANC is.
Conclusion:
The study concluded five variables associated with husbands’ participation in ANC in Indonesia, including residence, education, occupation, wealth, and parity.
Keywords
Introduction
The Maternal Mortality Rate (MMR) in Indonesia has significantly decreased. Based on the 2010 Population Census, the Indonesian MMR was 346 maternal deaths per 100,000 live births. The 2015 SUPAS (Survei Penduduk Antar Sensus/Inter-Census Population Survey) data showed the MMR in Indonesia dropped to 305 maternal deaths per 100,000 live births. Although it is pretty significant, this figure has not met the 2015 Indonesian MDGs target, 102 maternal deaths per 100,000 live births. 1 Moreover, in the Sustainable Development Goals (SDGs), the MMR target is 70 per 100,000 live births by 2030. 2
Compared to other South East Asia region countries, the Indonesian MMR has the highest record. The Indonesian MMR was nine times higher than Malaysia, five times higher than Vietnam, and almost two times higher than Cambodia. The World Health Organization (WHO) estimated the MMR in developed countries was at 12 maternal deaths per 100,000 live births. While in developing countries, there were 239 maternal deaths per 100,000 live births. On the other hand, the WHO estimates the MMR was 216 per 100,000 live birth globally.3,4
The government’s primary strategy is reducing maternal morbidity and mortality by conducting antenatal care (ANC). ANC is an early strategy to monitor and maintain mothers’ and fetuses’ health and safety, detect all pregnancy complications, take necessary actions, respond to complaints, prepare for birth, and promote a healthy lifestyle. Antenatal care is essential to detect and prevent all unexpected conditions during pregnancy.5,6 ANC should be conducted at least four times throughout pregnancy, according to the Indonesia Ministry of Health: once in the first trimester, once in the second trimester, and twice in the third trimester.7–9 The 2018 Indonesian Basic Health Survey reported 86.0% of the first ANC visit in Indonesia. Meanwhile, the percentage of the fourth ANC visit was 74.1%. 10 More than a quarter of pregnant women in Indonesia have not optimally done an ANC visit.
In the early 2000 period, the government issued a “Suami Siaga” policy (literally known as “Alert Husband”). The policy release addresses the high MMR in Indonesia. “Suami Siaga” is a national campaign to promote husbands’ participation in Indonesia’s maternal and child health programs. The previous evaluation in 2012 showed that husbands’ involvement was proven beneficial in increasing ANC’s involvement in Indonesia. 11
In many countries, including Indonesia, males or husbands play as the primary decision-makers in the household. 12 They commonly decide to allow wives or women access to maternal care services. 13 The majority of husbands supported their partners to allocate funds for maternal care services but were less involved in labor preparedness and postnatal care. 14
Several studies conducted in various countries showed that one of the ANC barriers was poor husbands’ support and involvement in the antenatal and labor processes. The poor of husbands’ permission is why women delay maternal health care.15–18 Some -research in Lao People’s Democratic Republic (Lao PDR) and Bangladesh found that husband involvement is the determinant of a continuum for maternal care. Husbands’ support in companying their wives to receive health services positively correlates with maternal and newborn health services.13,19
Indonesia recently has thousands of cultures that believe in their local medical knowledge. Local medical knowledge is sometimes contradictory to modern medical knowledge. 20 Pregnancy and childbirth are always judged as domestic affairs, specifically women’s experiences. In the Papua Muyu tribes, pregnant women must be exiled to a separate hut far from home because blood affects families’ health after childbirth. 21 It is different from the Gayo female tribes in Aceh, who felt ashamed and scared during pregnancy. Gayo women must hide their pregnancy because they were afraid of spiritual fetal kidnapping by evils as her stomach suddenly can be deflated by itself. 22
Husband’s participation is essential in encouraging their wives to utilize maternal care services. Therefore, research on husbands’ involvement in maternal care is required. This study aimed to analyze the aspects of the husband’s participation in the wife’s antenatal care visits in Indonesia. Based on the background narration, what factors can affect the husband’s involvement in ANC in Indonesia?
Materials and methods
Study design
The study was a cross-sectional study that used secondary data from the 2017 Indonesian Demographic and Health Survey (IDHS) (Female file: IDIR71FL_Individual Recode). The 2017 IDHS utilized stratified two-stage sampling. Stage 1: Using a systematic proportionate to size probability with the number of households from the 2010 population census listing, choose various census blocks. The survey utilizes an implicit stratification technique based on urban and rural areas to sort census blocks depending on their wealth. 23
Setting
To address the high MMR, Indonesian public health Institution actively supported (since the beginning of the 2000s) the involvement of husbands in the ANC through a national campaign called “Suami Siaga.” 11
Participants
The study population was women of childbearing age, aged 15–49 years old, and pregnant in the last 5 years before the interview. The study employed 14,319 respondents as the samples.
Outcome variables
The study used husbands’ involvement (Yes or Not) in ANC as the binary outcome variable. The related survey question was “Does husband accompany his wife in ANC visit?”
Independent variables
We focused on husband characteristics to avoid collinearity problems and according to paper aims. The explanatory variables were: residence (urban or rural), husband age (as continuous), an education level (no education, primary, secondary, and higher education), occupation (unemployed, professional/technical, managers/administrators, clerical, sales, services, agricultural self-employed, industrial workers, other), wealth status (poorest, poorer, middle, richer, richest), and parity (primiparous = 1, multiparous = 2–4, grand multiparous > 4).
The urban or rural place was based on the Central Bureau of Statistics requirement. The husband’s age is the respondents’ acknowledgment of their husbands’ last birthday. Primary education refers to junior high school, secondary to senior high school, and higher to tertiary education. The survey assessed wealth status through types of furniture and their prices. It counts a television, a bicycle or a car, and household goods, such as drinking water sources, bathroom amenities, and building materials for flooring—the study calculated assessment of this variable with the principal component analysis. National wealth quintiles were arranged based on household scores for each household and then divided into the same five categories, each contributing 20% of the population based on the distribution. 24
Data analysis
The first step used chi-square to select the categorical variables and the T-test to choose the continuous ones. Both tests identified the relationship between the independent variables and the husbands’ involvement in ANC as the dependent variable. This study employed Binary Logistic Regression to determine predictors because of the dependent variable’s nature. The research performed all statistical analyzes with IBM SPSS Statistics 21 software.
In addition, the study used ArcGIS 10.3 (ESRI Inc., Redlands, CA, USA) to produce a distribution map of the percentage of husbands’ involvement in antenatal care by the province in Indonesia. The Indonesian Bureau of Statistics provided a shapefile of administrative border polygons for the study.
Ethical approval
The study used secondary data from the 2017 IDHS for its materials analysis. The 2017 IDHS removed all respondents’ identities from the dataset. Respondents signed written consent forms to participate in this study, and children’s parents or guardians signed consent forms (under 16 years). For this study, the author obtained permission to use data from the website https://dhsprogram.com.
The 2017 IDHS follows the Standard DHS survey methodology established by ICF International’s Institutional Review Board under The Demographic and Health Surveys (DHS) Program (DHS-7) and evaluated and approved by the ORC Macro IRB in 2002. The Institutional Review Board of ICF International follows the US Department of Health and Human Services’ “Protection of Human Subjects” requirements (45 CFR 46). DHS surveys that meet the criteria are labeled DHS-7 Program authorized, and the paperwork for approval is included.
Results
This study presents the distribution map of the portion of husband’s participation in antenatal care by the province in Indonesia in Figure 1. The figure shows a random distribution pattern. The analysis results show that nationally, the average percentage of husbands’ involvement in antenatal care is 75.927%. Meanwhile, as the center of government, the island of Java offers husband’s participation in antenatal care is better than in other regions.

Distribution map of the percentage of husband’s involvement in antenatal care by the province. Indonesia, 2017.
Table 1 shows the descriptive statistics of the husband’s involvement in ANC and other related variables. The study discovered that husbands involved in ANC visits were dominant in both residence types: urban and rural areas. Meanwhile, the average age of husbands involved in ANC visits was slightly younger than those not engaged in ANC.
Descriptive statistic of husband’s involvement in ANC (n = 14,319). Indonesia, 2017.
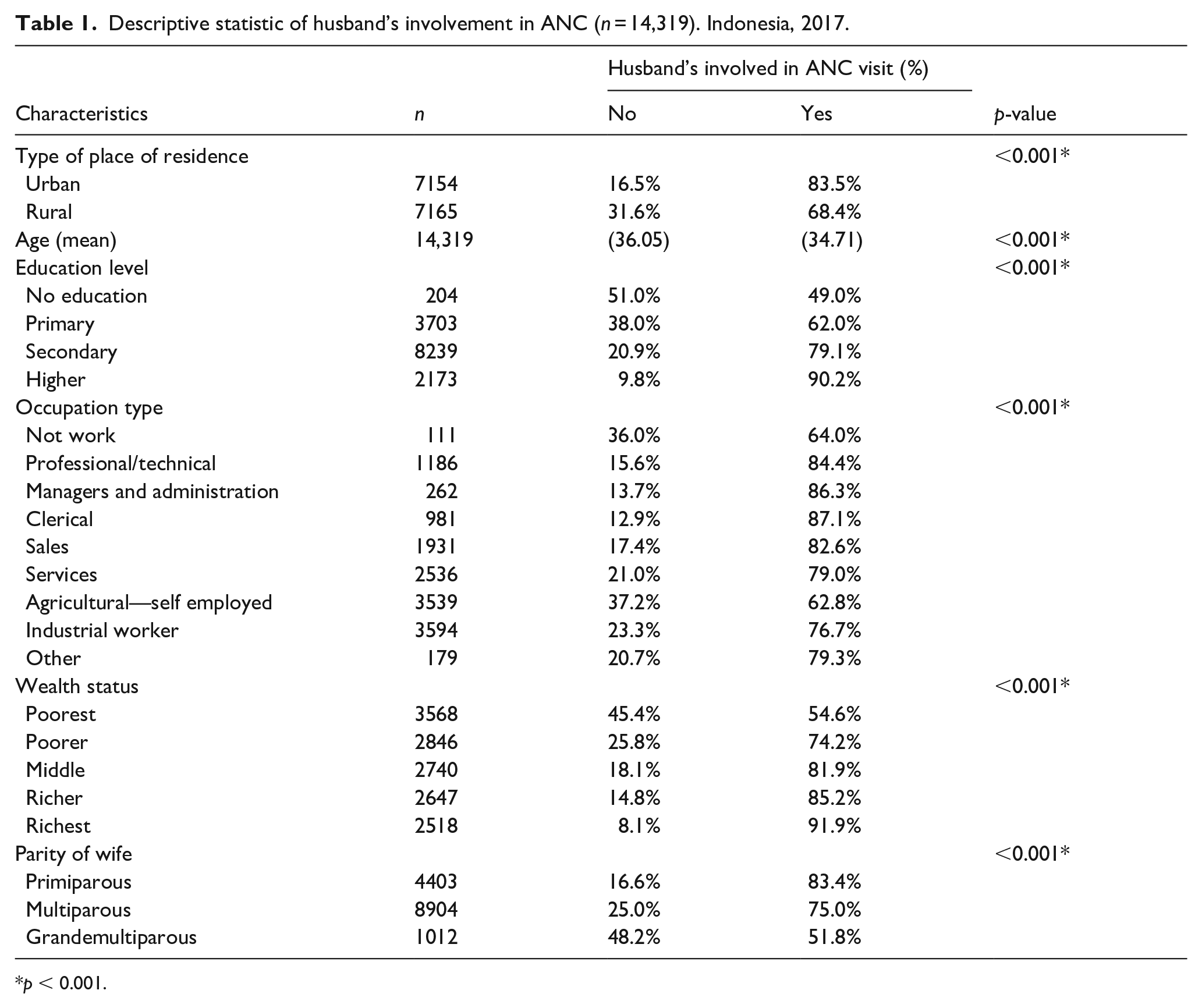
p < 0.001.
On the other hand, husbands of all education levels are dominantly involved in ANC visits. Except for the no education husband was not engaged in ANC visits. Moreover, husbands with any work type, wealth status, and parity are dominantly involved in ANC visits.
Table 2 displays co-linearity test results of the husband’s involvement in ANC and other related variables. It shows that all variables’ tolerance value, between the dependent and independent variables, is more significant than 0.10, while the variance inflation factor (VIF) value is less than 10.00. It indicated there are no multicollinearity symptoms in the regression model.
Results for the co-linearity test of husband’s involvement in ANC (n = 14,319). Indonesia, 2017.

Note: Dependent variable: husband’s involvement in ANC.
The binary logistic regression test results were employed to determine variables influencing the husband’s ANC involvement in Indonesia. Table 3 shows that husbands who lived in urban areas have odds of being involved in ANC visits 1.188 times (95% CI 1.078–1.308) more likely than those in rural areas. Meanwhile, the study found husband’s age did not correlate with the wife’s ANC in Indonesia.
Binary logistic regression of husband’s involvement in ANC (n = 14,319). Indonesia, 2017.

*p < 0.05; **p < 0.01; ***p < 0.001.
Results found husbands who had primary education have odds of being involved in ANC visits 1.357 times (95% CI 1.004–1.834) more likely than husbands with no education. Husbands with secondary education have odds of being involved in ANC visits 1.967 times (95% CI 1.456–2.657), more likely than those with no education. Husbands with higher education have odds of being involved in ANC visits 3.264 times (95% CI 2.320–4.593) more likely than husbands with no education.
Based on occupation type, professional/technical workers have odds of being involved in ANC visits 1.914 times (95% CI 1.217–3.010) more likely than unemployed husbands. Husbands who worked as managers and administrators have odds of being involved in ANC visits 2.023 times (95% CI 1.151–3.554), a higher chance than unemployed husbands. Clericals have odds of being engaged in ANC visits 2.142 times (95% CI 1.346–3.408), more likely than husbands who did not work. Husbands who worked as a salesman have odds of being involved in ANC visits 2.227 times (95% CI 1.468–3.532) more likely than those who did not work. Service providers have odds of being engaged in ANC visits 2.196 times (95% CI 1.424–3.385) more chances than unemployed husbands. Husbands who worked in agriculture have odds of being involved in ANC visits 1.887 times (95% CI 1.229–2.899) more likely than husbands who did not work. Besides, husbands who were industrial workers have odds of being involved in ANC visits 2.139 times (95% CI 1.393–3.285) more likely than husbands who had no job. These findings showed that husbands with employment types listed in the table were more likely to be involved in ANC. However, husbands who had other jobs did not differ from husbands who did not work. Based on the analysis results, husbands who work as salesmen have the highest probability of being involved in ANC visits.
Based on wealth status, Table 3 further illustrates that husbands in lower wealth status have odds of being involved in ANC visits 2.003 times (95% CI 1.789–2.243) more likely than the weakest groups of husbands. Those with median wealth status have odds of being involved in ANC visits 2.840 times (95% CI 2.499–3.229) more chances than the lowest groups of husbands. Wealthier husbands have odds of being engaged in ANC visits 3.242 times (95% CI 2.811–3.740), more likely than the lowest groups of husbands. Husbands with the most prosperous wealth status have odds of being involved in ANC visits 5.424 times (95% CI 4.516–6.514) the chances than the lowest groups of husbands. It shows that the more prosperous the husbands’ wealth status is, the more they get involved in ANC.
Table 3 informs that husbands who had multiparous wives have odds of being involved in ANC visits 0.641 times (95% CI 0.575–0.714) less likely than those who had primiparous wives. Husbands with grand multiparous wives have odds of being involved in ANC visits 0.341 times (95% CI 0.284–0.408) fewer chances than husbands who had primiparous wives. It suggests that the more children wives had ever been born, the more passive husbands’ involvement in ANC was.
Discussion
Husbands’ support for their partners is a good practice during married life. During pregnancy and childbirth, husbands who support their partners are considered modern men at home and handle tasks apart from their usual duties. It allows their wives to have enough rest during pregnancy. 25 Husbands’ active involvement was strongly correlated with alertness and increased wives’ knowledge of newborn danger signs. 26 However, a literature review with a narrative approach to husbands’ feelings found a different condition. Although husbands want to get involved, support their wives, and learn about fetal health, they often feel excluded from making perinatal screening decisions. 27 It signals that awareness of husbands’ involvement and maternal care providers need to be improved.
Husbands’ involvement in ANC in Indonesia is more concentrated in Java as the government center. This situation indicates that the implementation of the “Suami Siaga” (Alert Husband) policy which seeks to increase husbands’ involvement in the ANC, has not been spread evenly across all regions in Indonesia. The government still has to work harder to disseminate the policy.
Furthermore, the study finds five variables associated with husbands’ involvement in ANC in Indonesia: (1) the type of residence, (2) education level, (3) types of work, (4) wealth status, (5) parity.
(1) Husbands who lived in urban areas were more likely to be involved in ANC visits than rural areas. The Indonesian community tends to have more open access in urban areas, including information and health services.28–30 Regions with dominant urban regions have better ANC utilization.8,31,32
(2) The better husbands’ education level was, the more they got involved in ANC. This finding is similar to Lao PDR and Pakistan’s research conclusion, informing that husbands with higher education levels correspond to their involvement in the maternal process and newborn and child health services.19,33 In line with these findings, another study found husbands who had no formal education were 0.02 times more likely to decide maternal services for wives than those who attended formal education. 34 A study in Nigeria discovered that husbands’ involvement in maternity and delivery processes was minimal. In addition to the low educational level, this was also due to prevailing social norms. Nigerian husbands assumed that pregnancy and childbirth were under women’s business. 16 Several previous studies that took other health fields’ themes found education a positive determinant,35–39 while poor education hinders achieving better output.40–42 A slightly different finding was informed in a study in the Oromia Region-Ethiopia, telling that many husbands know obstetric danger signs. On the other hand, the study found that the husband had low participation. The situation indicates their low willingness to donate blood during their wife’s antenatal, delivery, and postpartum. 17
(3) Husbands who were employed in jobs listed were more likely to be involved in ANC, while those who had no job and more time are not a determinant of their involvement in the maternal process. Other studies in Northern Nigeria also found husbands’ occupation proves one of the determinants of women’s participation in maternal services. Husbands’ work determines the affordability to pay healthcare costs. 43
(4) The better husband’s wealth status was, the more involvement in ANC was. Previous studies in Pakistan, Eritrea, and Ethiopia similarly revealed that the better husbands’ wealth status was, the more they got involved in ANC.33,34,44 Encouraging husbands with good wealth status could reduce delayed ANC visits. 44 Several previous studies have informed that wealth status is a positive determinant of better health sector outcomes. Conversely, poor wealth status is often associated with lower effects.45,46
(5) Husbands who had wives with more births participated less in ANC. Husbands got involved more actively when their wives gave birth to their first child. In short, parity becomes one of the determinants in husbands’ involvement in maternal care services. These findings were similar to the previous study in Yangon, Myanmar. Husbands with high parity wives tend to have low participation in the ANC. In addition to parity, some other variables as determinants were educational level, marriage status, decision-making level in the family, exposure to maternal health education, and perception of risk during pregnancy and childbirth. 14
Policymakers in Indonesia should consider the findings of this research while planning their policies; they may help accelerate the husband’s involvement in antenatal care visits.
Strength and limitation
The study’s strength is the use of big data as material for analysis. However, this study also has limitations. The study was conducted with a quantitative approach not to cover the phenomena of local Indonesian values and culture that could potentially influence husbands’ involvement in their wives’ ANC, for example, concerning the patriarchal social system, the value of children, the value of family, and the value of pregnancy.22,47
Footnotes
Acknowledgements
The author would like to thank the Inner City Fund for allowing the use of the 2017 IDHS.
Contributions
ADL designed study concepts, prepared data, conducted data analysis and wrote manuscript drafts. RDW analyzed results, wrote manuscript drafts, and finalized manuscripts. NEWS and SS conducted data analysis, wrote draft manuscripts, and finalized the manuscripts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Significance for public health
In the early 2000s, the Indonesian government launched a national campaign (Suami Siaga) to encourage husbands to participate in maternal and child health programs in order to reduce maternal morbidity and mortality. The findings of this study could be used to send specific messages to the 25% of Indonesian husbands who are not yet actively participating in pregnancy by highlighting the socio-demographic predictors of husbands’ involvement in antenatal care.