
Abstract
Background:
Continuum of care (CoC) for Maternal Health Care (MHC) is a key strategy aimed at saving lives and promoting the well-being of women and newborns. To achieve the global targets for reducing maternal and newborn mortality, it is preferable to ensure the completion of key care stages (Antenatal, Institutional Delivery, and Postnatal) rather than fragmented care. Therefore, investigating the determinants of CoC completion for MHC is imperative for recommending schemes and designing strategies.
Objective:
To assess the determinants influencing completion of the maternal healthcare continuum among pregnant women in Jimma Zone, Southwest Ethiopia.
Methods and Materials:
A community-based prospective study was conducted from July 2020 to June 2021 among 1065 pregnant women from randomly selected woredas in Jimma Zone. The data were collected, entered using Epi-data and analyzed with SPSS software. Binary logistic regression was used to select candidate variables for multivariate analysis. Multivariate analysis was performed to identify associations between the dependent and independent factors. Principal Component Analysis (PCA) was used to determine the socioeconomic index.
Results:
The overall completion rate was 16.1% (CI, 13.8%–18.5%), with significant dropouts observed between the first and the fourth ANC.
Factors associated with the completion of MHC included the women’s residence (AOR: 1.73 95% CI: 1.07, 2.81), educational status of their partners (AOR: 5.60 95% CI: 2.40, 13.08), women’s occupation (AOR: 2.57 95% CI: 1.28, 5.16), knowledge of ANC (AOR: 7.64 95% CI: 4.03, 14.48), knowledge of PNC (AOR: 4.88 95% CI: 3.21, 7.42), service provided during ANC contacts (AOR: 3.39 95% CI: 1.94, 5.93), parity (AOR: 1.86 95% CI: 1.11, 3.12), time of booking for ANC (AOR: 2.10 95% CI: 1.45, 3.03), and nature of care (AOR: 2.03 95% CI: 1.07, 3.82). Additionally, factors such as topography, distance, lack of transportation, facility closeness, and indirect costs were associated with the completion for MHC.
Conclusion and Recommendations:
The completion rate of CoC for MHC remains low. Factors influencing completion include women’s residence, partners’ educational status, women’s occupation, services provided during ANC, history of PNC use, parity, time of booking for ANC, knowledge of ANC and PNC, and nature of care. To address this, strategies should focus on empowering women economically, improving knowledge of ANC and PNC, enhancing the capacity of health facilities to provide comprehensive ANC services, and making the service delivery more supportive. Further research is recommended to explore the impact of CoC for MHC on birth outcomes.
Introduction
Maternal health care (MHC) is globally recognized as an essential component of healthcare programs, in both high- and low-income countries (HLICs), aimed at reducing maternal mortality. 1 Antenatal Care (ANC), Institutional Delivery (ID), and Postnatal Care (PNC) are crucial components of MHC designed to prevent maternal and newborn complications and deaths worldwide. 2
The continuum of care is a framework for providing of maternal health care 3 that has become a core principle of programs for maternal, newborn, and child health (MNCH) which aim to reduce maternal, neonatal, and child deaths.4,5
To achieve the global targets of ending preventable maternal and under-5 mortality, a complete maternal health care continuum including ANC, skilled birth attendance (SBA), and PNC) is essential. 6
A meta-analysis on the effectiveness of antenatal to postnatal care in reducing neonatal, perinatal, and maternal mortality in low- and middle-income countries found that receiving care from antenatal to postnatal periods reduces the risk of combined neonatal, perinatal, and maternal mortality by 15%. 7
However, studies conducted in various parts of the world found that dropouts across the continuum of maternal health care are a significant challenge. For example, a study conducted in Cambodia found that only 5% of mothers completed the continuum of care, with the highest discontinuation rate (73.6%) occurring during postnatal care. 8
In contrast to what should be the case, a study conducted in Tanzania found that 96.5% of pregnant women received at least 1 Antenatal Care (ANC) contact, 66.5% had 4 or more ANC contacts, 65% gave birth at a health facility, 22.5% attended Postnatal care (PNC), and only 10% received all the recommended components of care. 9
A cross-sectional study carried out in Ghana to assess the continuum of care in the MNCH program found that only 8.0% of participants had completed CoC for MNCH. The greatest dropout was found between delivery and PNC within 48 hours postpartum. 10
According to a study in Nigeria to assess the determinants of maternity care dropout, 60.6% of women received ANC, but 38.1% dropped out and never received skilled birth attendance (SBA). Furthermore; 50.8% of those who received skilled delivery care did not attend postnatal appointments. 11
A study conducted in Egypt demonstrated that 50.4% of the participants had achieved a continuum of care. Specifically, 90% had undertaken at least 4 or more ANC visits; 85% delivered their babies with a SBA; and 53.2% received PNC. 12
Demographic and Health Survey data from 9 countries (Bangladesh, Nepal, Pakistan, Ethiopia, Malawi, Rwanda, Senegal, Tanzania, and Uganda) were analyzed to assess the continuum of care pathway for maternal health in South Asia and Sub-Saharan Africa. The study revealed a significant dropout (more than 50%) occurring early in the continuum of care, between the first ANC visit and 4 or more ANC visits. 13
Furthermore, cross-sectional studies conducted in various regions of Ethiopia on the completion of the continuum of maternal healthcare continuum yielded varying results: 9.7% completion in Arbaminch Zuria woredas, 6 12.1% in the West Gojam Zone of the Amhara region, 14 9.1% and 6.56% according to the different studies using data from Ethiopia Demographic and Health Survey (EDHS) 2016,15,16 Motta town and Hulet Eji Enese district, Northwest, 47%, 17 Enemay District, Northwest, 45%, 3 Gondar Zuria and Dabat districts, Northwest, 21.6%, 18 Debre Berhan Town, Amhara, 37.2%. 19 These findings underscore significant disparities within results obtained from the same data set (EDHS 2016).
Numerous strategies have been devised and implemented to address these challenges, including bringing healthcare services closer to the community, community mobilization, improving service quality, preventing and treating complications, promoting safer pregnancies and enhancing PNC.1,20-23
Despite all these efforts, completion rates for MHC remain low, particularly in Oromia, where this study was conducted. Specifically, 4 or more ANC attendance was 40.6%, institutional delivery was 41%, and PNC within the first 2 days was just 26.1%. It is also worth noting that the country uses a non-standard definition of SBA, and so 5.8% of the work of SBAs is performed by Health Extension Works (HEWs).20,24,25
All these studies highlight a need to investigate the motivations for completing MHC as well as the factors that contribute to non-completion. Research in this area can provide valuable information for policymakers, healthcare providers, and those designing strategies to improve completion of MHC.
Methods and Materials
A community-based prospective study was conducted in Jimma Zone from July 2020 to June 2021. Jimma Zone is one of the 21 zones that make up the Oromia Regional State, located 350 km southwest of Addis Ababa. It comprises 21 districts and 2 town administrations. According to the 2021 Jimma Zonal annual report of the Zonal Health Desk, the Zone has a total population of 3 599 836. There are 562 Kebeles (local administrative units) served by 1 tertiary hospital, 3 general hospitals, 5 primary hospitals, 122 health centers, and 512 health posts. There are 3327 health professionals of all types (excluding those working at hospitals), and 1136 health extension workers.26,27
The study population comprised pregnant women in the randomly selected woredas of the zone who fulfilled the inclusion criteria. Pregnant women with a gestational age of less than or equal to 26 weeks, with at least 1 birth history, residing in the selected woredas, who received their first ANC during enrollment were included in the study.
The minimum required sample size for this study was calculated using Epi-Info V.7.2.4.0 statCalc and 2 sample proportion comparisons based on several assumptions: Alpha of 0.05 (95% CI), power of 0.8, a ratio of unexposed (incomplete CoC) to exposed (complete CoC for MHC) groups of 23.44, a probability of the event (birth outcomes) in the non-exposed group at 25.78%, and the probability of the event (birth outcomes) in the exposed group at 1.1%, with a design effect of 2. Finally, to account for non-responses and loss to follow-up, a 10% buffer was added, resulting in a final sample size of 1065 participants.
The cohort of pregnant women enrolled for the follow-up study was identified using a multistage cluster sampling technique. To begin with, the zone’s 21 districts were identified and stratified based on population. Two districts were randomly selected from the 21. Subsequently, the 2 districts were stratified into semi-urban and rural kebeles. Then, using a simple random sampling method (lottery), 45 kebeles were selected from a total of 67 kebeles. Pregnant women were then enrolled in the follow-up study through house-to-house visits and were subsequently tracked for their ANC, facility delivery, and PNC experiences (Figure 1).

Schematic display of the sampling procedure, 2020.
For this study, the dependent variable was the completion status of the continuum of care for MHC. It was categorized as “complete” when a woman had at least 4 ANC appointments, assistance from a SBA, and at least 1 PNC visit after discharge or home delivery. The independent variables were categorized into 3 groups:
Data collection tools were adapted from various sources. Wealth index indicators were adapted from the Ethiopian Demographic and Health Survey (EDHS). 28 Indicator measures for Person-Centered Maternity Care (PCMC) were adapted from a validated tool to measure person-centered maternity care in developing settings. 29 Maternal care practices were adapted from World Health Organization (WHO) guidelines. 30 Data on determinants of MHC utilization were collected using structured questionnaires adapted from various sources.29,31-35 Questionnaires were prepared in English, then translated into “Afan Oromo” to collect the data. Since this was a follow-up study, data were collected at 3 time points (Phase I, Phase II, and Phase III) using pre-tested interviewer-administered structured questionnaires.
During phase I, home visits was used to count pregnant women. All identified pregnant women in the 45 Kebeles were enrolled as a cohort for the study. Data collected in this phase include basic socio-demographic information, economic status, previous obstetric history, MHC utilization experience, knowledge of MHC, services and advice received during previous pregnancy, and services and advice received during the first ANC visit of the current pregnancy.
Phase II was at 3 months post baseline (fourth ANC contact, gestation 36–38 weeks). During this phase mothers were followed to assess the completion of their ANC. Phase III took place 10 weeks after Phase II. The purpose of this phase was to assess maternal healthcare practices, birth outcomes, access to maternal health services, women-centered maternity care, decision-making autonomy, and social support. The data collectors were informed about the relevance and objectives of the study and were trained on the study instrument and data collection procedure including handling confidential information, informed consent, and interview technique.
The data collectors worked under close supervision and debriefing sessions were held with principal investigator, supervisors, and data collectors to address the challenges promptly and take corrective measures. Data were meticulously entered and cleaned before analysis.
Supervisors ensure data completeness and consistency. Collected data were coded and entered into Epidata V.4.6.0.2 to minimize logical errors and maintain skip patterns. Data were then exported to SPSS version 20.0 for cleaning, editing, and analysis. Descriptive analysis was performed to summarize the variables, by computing proportions and statistics. The wealth index was calculated using Principal Component Analysis (PCA). Knowledge of ANC, ID, and PNC, decision-making autonomy, information and advice given at or during ANC, ID, and PNC, social support, and women-centered maternity care were computed using operational definitions.
Bivariate analysis was used to examine the relationships between the dependent and independent variables and the selection of candidate variables for multivariate logistic regression by taking just 1 dependent and 1 independent variable at a time, which is equivalent to univariate logistic analysis. All variables with P-values less than 0.25 were included as candidate variables for the final model. 36 A P-value less than .05 was considered statistically significant in multivariate logistic regression to determine factors associated with the continuum of care completion and an adjusted odds ratio with a 95% confidence interval.
Ethical approval was obtained from Jimma University, Health Institute, Institutional Review Board (IRB) Ref. No IHRPGD/433/2019 (27th November 2019). Administrative clearance was obtained from the zone and selected woredas health offices. Information sheets addressing the objectives of the study, and the benefits and harms were given to the study participants. Each respondent provided written informed consent before data collection. Participation in the study was entirely voluntary. Consent was obtained for those participants unable to read by having the data collectors read it to them line by line. The participant’s right to leave the interview at any moment was safeguarded. Data collectors were instructed to ensure confidentiality, give pertinent health information based on participant needs, and arrange referrals to medical facilities for mothers who had problems.
Results
A total of 1065 pregnant women were initially planned to be included in the study. However, after excluding cases with incomplete data, instances of abortion, loss to follow-up, and maternal deaths the analysis ultimately included 987 pregnant women, resulting in a response rate of 92.68%.
Socio-demographic and economic characteristics
Of the 987 pregnant women included in the analysis, 527 (53.4%) were aged between 25 and 29, with a mean age of 26.63 (SD ± 3.89). The majority 788 (79.8%) resided in rural area. The predominant ethnic group was Oromo (89.7%), and Muslim was the dominant religion (84.3%). Approximately one-third of the mothers (35.8%) had no formal education. While two-thirds were housewives (68.3%). In terms of their current marital status, nearly all participants (98.6%) were married. More than two thirds of husbands (69.2%) were farmers. One-third (321/32.5%) of the study group came from small families with similar economic status (Table 1).
Distribution of the study participants by their socio-demographic and economic characteristics, July 2020 to June 2021, Jimma Zone, Ethiopia.

Other*, Gurage, Yemi, Kefa; Other**, has no regular occupation, student, self-employee; Other***, deriver, no regular occupation, Sheki, self-employee; Other****, divorced, widowed, single.
History of maternal health care usage
A significant proportion of the women (25.7%) had no history of ANC contacts during their index pregnancy. Of those who utilized ANC, (65.1%) received incomplete care; only (18.7%) received complete advice. Approximately 10% of patients (102 individuals) experienced complications during pregnancy. Of those who gave birth in a health facility, 613 (79.8%) of them stayed in the facility for less than 24 hours following delivery. In total, 219 participants (22.2%) gave birth at home. From the total cohort only (15.3%) received PNC after being discharged or having a home birth (Table 2).
Distribution of the study participants by their past history maternal health care utilization, July 2020 to June 2021, Jimma Zone, Ethiopia.
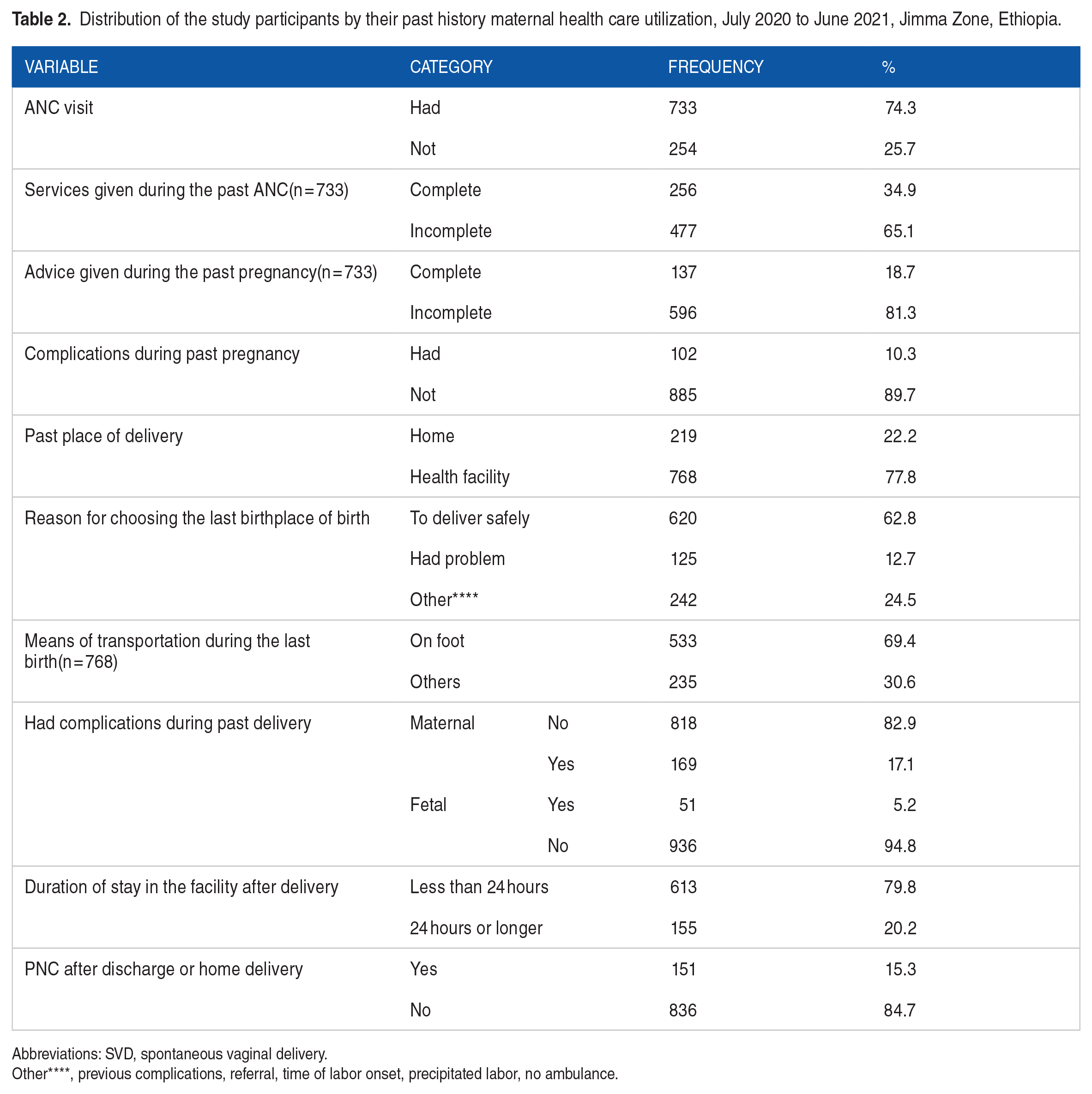
Abbreviations: SVD, spontaneous vaginal delivery.
Other****, previous complications, referral, time of labor onset, precipitated labor, no ambulance.
Current use of maternal healthcare
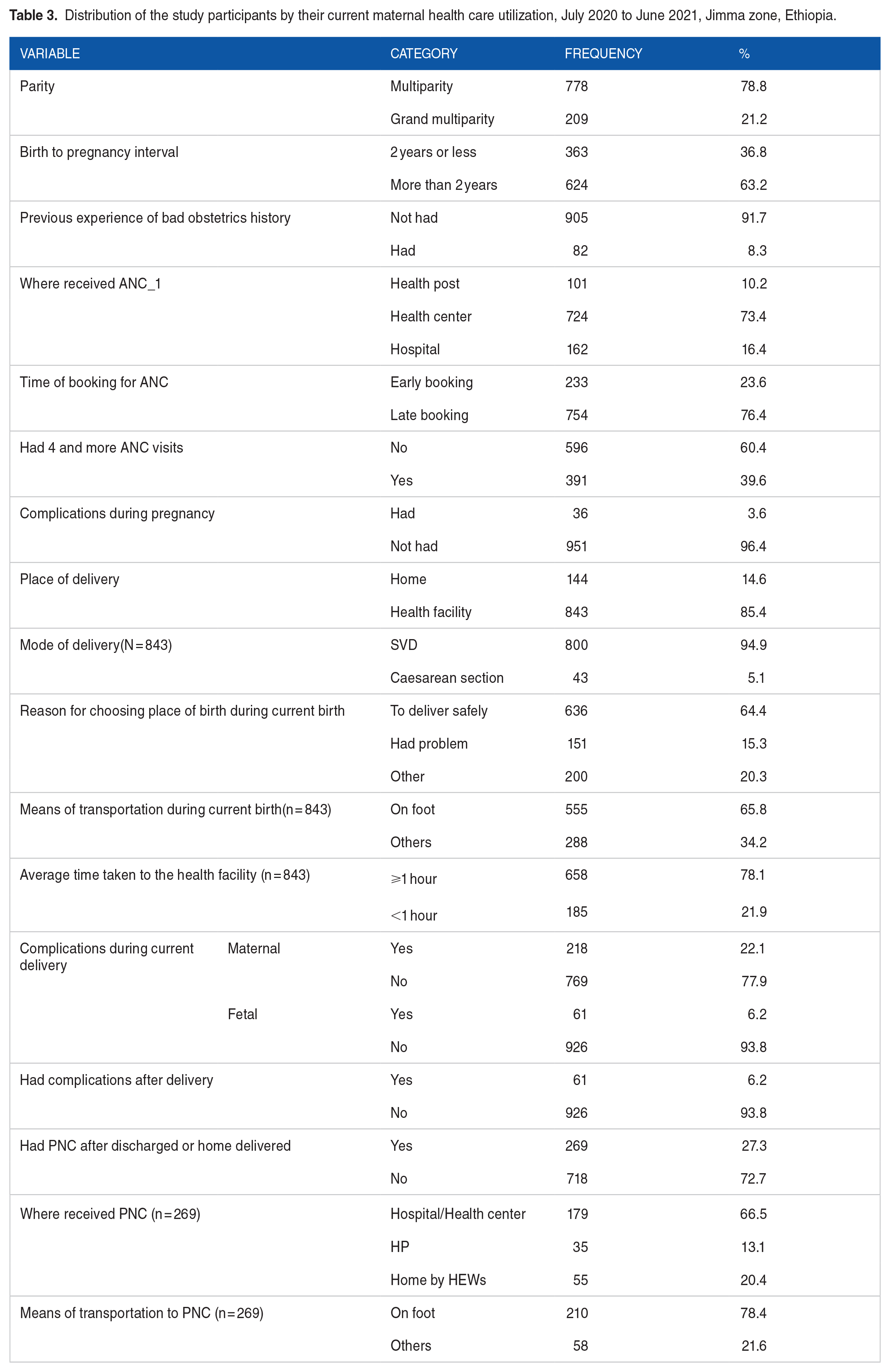
The majority (78.8%) of women were multiparous, and 36.8% had a birth-to-pregnancy interval of 2 years or less, 82 (8.3%) had previous experience of bad obstetric history, 724 (73.4%) had their first ANC at health centers, 754 (76.4%) made a late booking for ANC, and 391 (39.6%) of them had 4 or more ANC. Regarding the place of delivery, 144 (14.6%) gave birth at home, and 151 (15.3%) chose the place of birth because of a health issue. In all, 218 (22.1%) had maternal complications during current delivery, and only 269 (27.3%) of them had PNC after being discharged or having a home birth. Overall only 23 (2.3%) of the women included in this study had the recommended 4 PNC appointments within 6 weeks of giving birth (Table 3).
Distribution of the study participants by their current maternal health care utilization, July 2020 to June 2021, Jimma zone, Ethiopia.
Knowledge of maternal health care and given services
The majority of participants (63.3%) were aware of ANC, while 91.6% were knowledgeable about SBA. However, 83.7% had no knowledge of PNC (Table 4).
Distribution of the study participants by their knowledge of maternal health care and given services, July 2020 to June 2021, Jimma zone, Ethiopia.

Person-centered maternity care, social support, and decision making
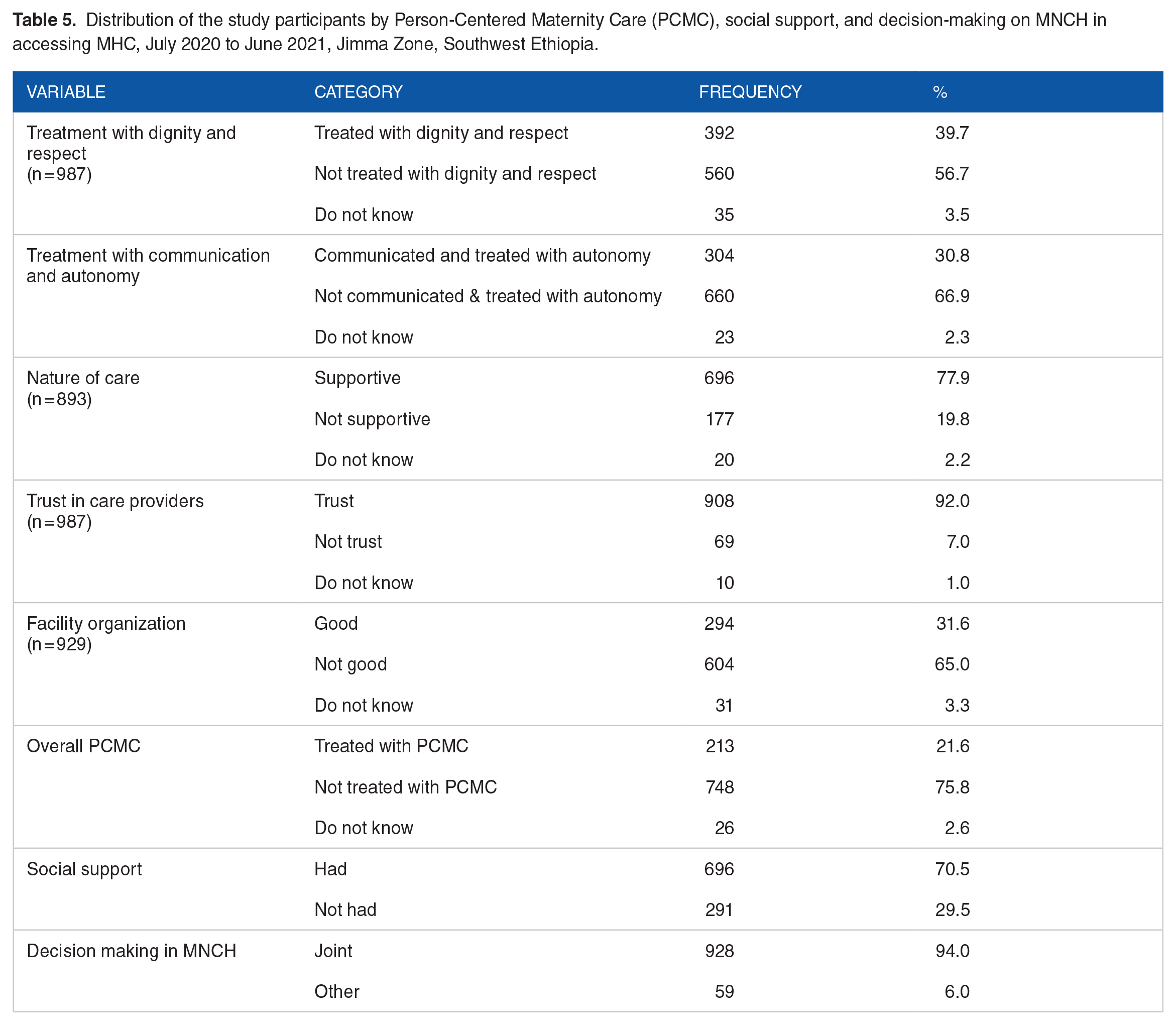
In all, 560 (56.7%) of women reported that they were not treated with respect and dignity, and 660 (66.9%) reported that they were not communicated and treated with autonomy. Six hundred ninety-six (77.9%) perceived that they received supportive care, 696 (70.5%) said they had social support, and almost all of them made a joint decision on access to MHC. Additionally, the overall PCMC was determined, and only 213 (21.6%) of them felt they received PCMC (Table 5).
Distribution of the study participants by Person-Centered Maternity Care (PCMC), social support, and decision-making on MNCH in accessing MHC, July 2020 to June 2021, Jimma Zone, Southwest Ethiopia.
Completion of the maternal health care continuum
Of those women who started ANC 391 (39.6%) had 4 or more ANC contacts, 36.7% (362/987) had 4 or more ANC contacts and gave birth at health facility, but of those who had 4 or more ANC contacts 43.9% (159/391) received PNC The overall completion of CoC for MHC for this study cohort was 159/987 (16.1%) (Figure 2).

Overall completion status of the maternal continuum of care for MHC, July 2020 to June 2021, Jimma zone, Ethiopia.
Perceived reasons for dropping out of maternal health care
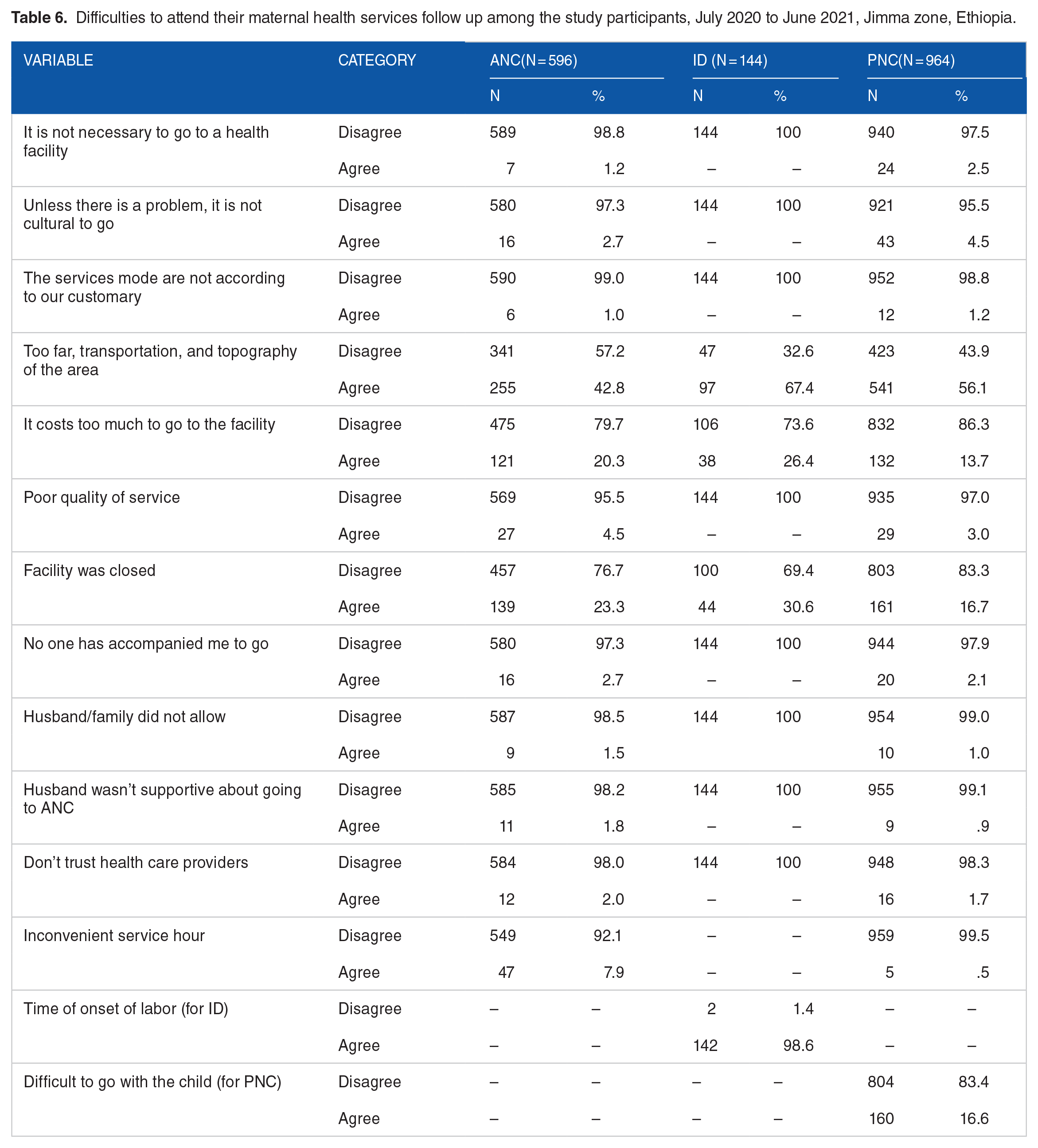
Women were asked about the reasons for dropping out of MHC. The most frequently reported barriers to care were lack of transportation, landscape and geography of the area, distance from facilities, lengthy wait times for services, inconvenience of service time, time of onset of labor, difficulty attending with a child, and high travel costs (Table 6).
Difficulties to attend their maternal health services follow up among the study participants, July 2020 to June 2021, Jimma zone, Ethiopia.
Variables associated with the completion of the maternal health care continuum
On bivariate analysis, several socio-demographic and economic variables, as well as obstetric and MHC utilization factors were significantly associated with the completion of CoC for MHC (P < .25). These factors included place residence, educational status of both partners, occupational status of partners, family size, and household wealth, history of ANC contacts, time of booking for ANC, knowledge about ANC and PNC, access to person-centered maternity care, and social support (Table 7).
Binary and multivariable logistic regression of factors associated with completion of the CoC for MHC, July 2020 to June 2021, Jimma zone, Ethiopia.
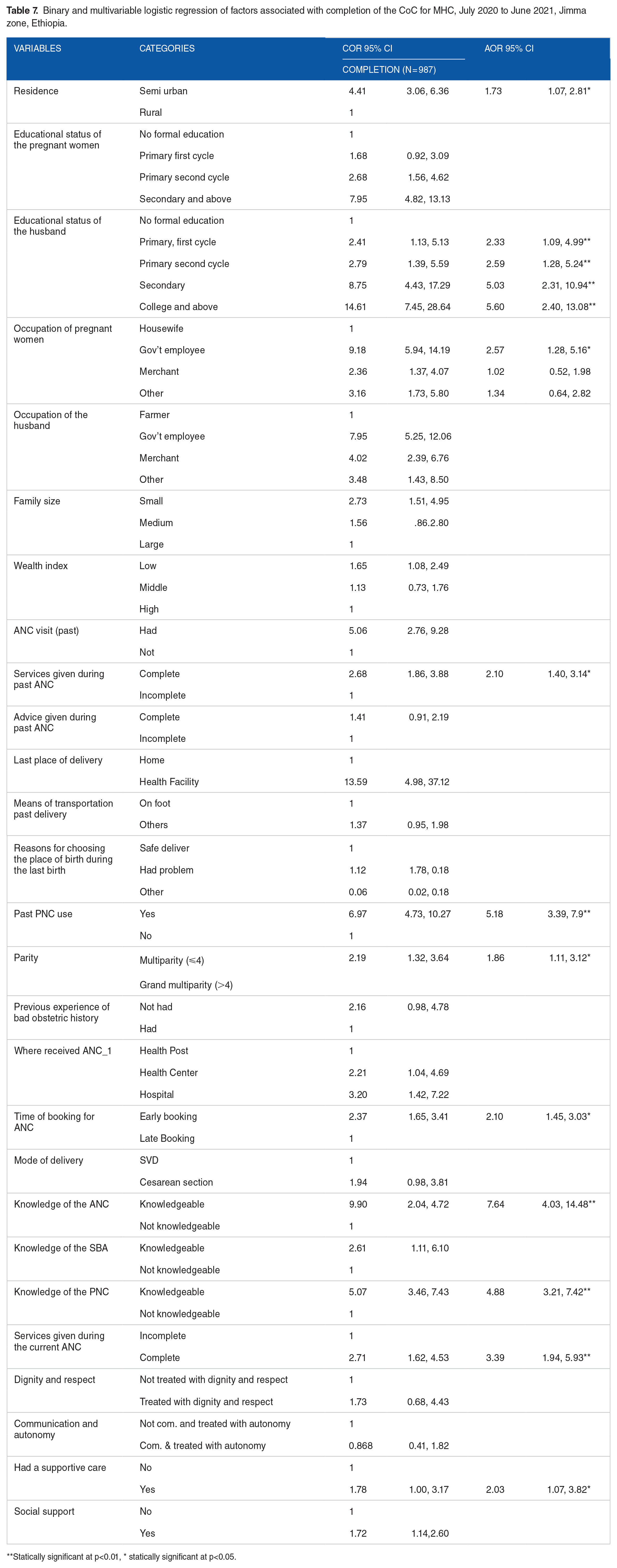
Statically significant at p<0.01, * statically significant at p<0.05.
In multivariate logistic regression analysis, several factors remained significant predictors of completing CoC for MHC: residency, educational status of partners, woman’s occupation, service provided during previous ANC, history of PNC use, parity, time of booking for ANC, knowledge about ANC and PNC, service provided during the current ANC, and nature of care.
Women’s residence was a significant predictor of completion of CoC for MHC. Semi-urban residents nearly twice more likely to complete CoC than rural residents (AOR: 1.73, 95% CI: 1.07, 2.81). Additionally, women whose partners had a college or above were nearly 6 times more likely to complete the CoC compared to those whose partners had no formal education (AOR: 5.60, 95% CI: 2.40, 13.08). Government employees were almost 3 times more likely to complete CoC than other groups (AOR: 2.57, 95% CI: 1.28, 5.16). Knowledge of ANC, PNC, and services rendered during ANC were also associated with completing MHC. Women who were knowledgeable about ANC and PNC were almost 8 and 5 times (AOR: 7.64 95% CI: 4.03, 14.48), (AOR: 4.88 95% CI: 3.21, 7.42), more likely to complete the CoC compared to their counterparts, respectively, and those who had completed recommended ANC service packages during the current ANC contacts were nearly 2 times (AOR: 3.39 95% CI: 1.94, 5.93) more likely to complete the CoC (Table 7).
Discussion
The continuum of care has gained increasing attention in the context of maternal, newborn, and child health, with the aim of ensuring every woman and child receives timely and appropriate services throughout the continuum. 37 Completion of the continuum is a crucial intervention to maintain maternal health during pregnancy, childbirth, and the postpartum period.
According to this study, only 16.1% (CI, 13.8%–18.5%) of women completed the continuum of care for MHC. Significant dropouts were observed between the first and fourth or more ANC contacts, followed by institutional delivery and postnatal care.
This completion rate is higher than findings from studies evaluating the continuum of care for MHC in Cambodia, 5%, 8 Tanzania, 10%, 9 Ghana, 8 %, 10 and Southern Ethiopia, Arbaminch Zuria woredas, 9.7%, 6 West Gojam Zone of the Amhara region, 12.1%, 14 as well as the evidence generated from EDHS 2016, which reported 9.1% and 6.56% completion rates.15,16
The variation in completion rates across studies can be attributed to several factors including differences in geographical scope, study setting and design, sample sizes, the proportion of mothers receiving a service, and the criteria used for defining completion of MHC. Additionally, the time gap between studies and the expansion in the number of health facilities and skilled professionals may contribute to varying results.
For example, studies from Cambodia, Tanzania, Ghana, and some from Ethiopia used data from Demographic and Health Surveys, which are susceptible to recall bias due to their retrospective nature. These cross-sectional studies rely on participants’ memory of past events potentially leading to under-reporting or over-reporting of service utilization to please the researcher. Furthermore, this study was undertaken during the COVID-19 pandemic, during which time the government paid increased attention to the demand for provision of maternal health services. This contemporaneous change may have influenced the results.
However the completion rate in this study is still lower than findings of the studies from various parts of Ethiopia, where completion rates ranged from 21.6% to 47%.3,17-19
Even though the government paid attention to MHC during COVID-19, the pandemic has been recognized as one of the barriers to MHC use, with disrupted community mobilization efforts and changes to the cost and regulation of transportation. 38 This could have influenced changes in completion rates. Additionally, the follow-up nature of this study may have reduced the likelihood of dropouts exaggerating their service utilization, a phenomenon that can occur in cross-sectional studies. These findings highlight the need for further efforts to reduce dropout rates and achieve intended targets.
This study identified predictors for completing CoC for MHC. These predictors includes: residence, partners’ educational status, women’s occupations, services provided during ANC contacts, history of PNC, parity, time of booking for ANC, knowledge of ANC and PNC, and the nature of care.
Partners’ educational status emerged as a significant predictor of completion of the continuum of care for MHC. A woman whose partners had college education or higher being nearly 6 times more likely to complete the continuum of MHC compared to those whose partners had no formal education.
This suggests the importance of education to both women and their partners, as educated husbands are more likely to support their wives in seeking healthcare.
Residence in a semi-urban area increased the likelihood of receiving MHC, possibility due to better access to health facilities, higher education status, increased income, greater awareness of maternal health, access to media, and higher health-seeking behavior being higher than those from rural areas.
Women’s occupation was a significant predictor of completion of the continuum of MHC. This might be because mothers with an income are more likely to make autonomous decisions. These women also have the financial capacity to cover indirect costs associated with MHC.
In this study, grandparental multiparous mothers were less likely to complete the CoC for MHC. An explanation for this may be previous favorable birth outcomes without any MHC. Also, having a large family could impact socioeconomic status and the ability to cover indirect expenses of MHC.
The services provided during ANC contacts were strongly associated with CoC completion for MHC. This finding was supported by a systematic review and meta-analysis from Sub-Saharan African countries, which reported that mothers who attended at least 4 ANC contacts were more likely to give birth in a health facility.4,39 Results such as these give weight to the current thinking that pregnancy is a window of opportunity to improving women’s health in general. ANC contacts increase the quality of information women receive about MHC and allow patients to become familiar with medical personnel and health facilities.40,41
The nature of the care provided (supportive care) emerged as another predictor of completing CoC for MHC. This is in line with findings of a study conducted in Egypt, which showed that patients who had blood pressure checks, urine, and blood tests at ANC visits were more likely to use SBA and PNC. 12 A positive correlation was also found when patients had counseling, interactions with health workers.9,37,42
The study limitations
This study made possible to assess the actual state of maternal healthcare practices. Additionally, a large sample size was used, resulting in great analytical power and precision. Despite the high sample size, due to the logistical complexities of the follow-up study, this study was based on limited districts. The dichotomization or classification of the composite variables at various cut-off points may have its own limits when referring to proportion. Also, all the possible efforts were made to use standards and as many variables as possible to make them more objective.
Conclusion and Recommendations
This study demonstrated that less than 1 in every 5 women completes the recommended continuum of care for MHC. Women’s residence and occupation, their partners’ educational status, the services provided during ANC contacts, history of PNC use, parity, and time of booking for ANC, knowledge of ANC and PNC, and nature of care were found to be the predictors of completion of CoC for MHC.
Hence, this study results highlight that the dropout in MHC and detail the predictors for completion of CoC for MHC must be made known to those who determine health policy. It is vital that increasing the quality of healthcare delivery, reduce complications related to childbirth, and improving health outcomes.
Additionally, efforts should focus on empowering women economically, enhancing knowledge of maternal health services, strengthening health facilities’ capacity to provide quality, supportive ANC
Furthermore, follow-up studies are recommended to fully understand the effect of completion of CoC for MHC on birth outcomes.
List of abbreviations
Antenatal care [ANC ], Continuum for care [CoC]; Ethiopia Demographic Health Survey [EDHS], Facility Delivery[FD], Institutional Delivery [ID], Institutional Review Board [IRB], Maternal Health Care [MHC], Health Extension Works [HEWs] Maternal Mortality Ratio [MMR], Maternal, Neonatal and Child Health [MNCH], Principal Components Analysis [PCA], Postnatal care [PNC], Skill birth attendance [SBA] Spontaneous vaginal delivery [SVD], World Health Organization [WHO], Weeks [Wks]
Operational definitions
Footnotes
Acknowledgements
I would like to express my very great appreciation to my supervisors for their commitment and valuable contribution from the planning to the finalization of this work. Second, my appreciation extends to Jimma University for funding the study. Also, my thanks go to the KOFIH-JU-JZHO collaborative MCH project for their transportation assistance and to friends and family for their backing during this work. Thanks should also go to the study participants and data collectors.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The source of funds for this study is Jimma University, Institute of Health.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SB, GT, and MA, protocol development. SB, methodology, formal analysis, manuscript preparation, and all authors read, commented on the method, analysis, and approved the final manuscript.
Ethics Approval and Consent to Participate
The manuscript has adhered to the ethical standards. Ethical approval was obtained from the IRB of the Health Institute, Jimma University. Informed consent was obtained from each respondent before actual data collection, and participation in the study was totally voluntary.
Availability of Data and Materials
Data are available from the corresponding author on request.