
Abstract
Background:
Hypertensive disorders of pregnancy disproportionately impact Black women, contributing to higher morbidity and mortality. Neighborhood deprivation provides insights, as Black families often face hindered access to health care. This study examines the link between neighborhood deprivation and access to prenatal services for high-risk pregnant individuals in North Carolina’s Medicaid-managed Pregnancy Medicaid Homes (PMH).
Methods:
Dataset included Medicaid claims, birth certificate, risk screening, care management, and American Community Survey data from January 2017 to February 2020. We used multivariate logistic regression models to estimate the relationship between timely prenatal care entry, risk screening, and face-to-face care management and Indices of Concentration of the Extremes for race and income, categorized into quintiles from 1 (most deprived) to 5 (most privileged). Analysis included 53,000 pregnant individuals with ≥1 preeclampsia risk factor.
Results:
We found that those from the most deprived neighborhoods had an 11.1 (standard error [SE]: 0.023; 0.0000), 4.1 (SE: 0.014; 0.000), and 8.0 (SE: 0.013; 0.000) percentage points lower likelihood of timely prenatal care entry, risk screening, and care management, respectively, compared with those from the most privileged neighborhoods. Conversely, non-Hispanic Black (NHB) individuals in the least privileged neighborhoods demonstrated a higher likelihood of timely prenatal care entry and care management compared with their non-Hispanic White peers.
Conclusions:
This study reveals that neighborhood deprivation limits access to prenatal care, risk screening, and care management. Although NHB pregnant individuals have slightly better access, likely due to initiatives such as the PMH, deprivation remains a significant barrier. Addressing these disparities requires equity-focused interventions to ensure that all pregnant individuals receive timely prenatal services.
Keywords
Background
Stark disparities 1 exist in hypertensive disorders of pregnancy (HDoPs) in the United States,2–5 particularly among low-income, non-Hispanic Black (NHB) birthing people, who account for 24.2% of births. 5 Studies have shown that Black birthing individuals have a 21–31 percentage point higher probability of developing HDoPs, greater than any other racial/ethnic group, even after adjusting for microlevel factors such as comorbidities, socioeconomic status, and education.4–8 Until recently, it was common to assume race as a risk factor for HDoPs, particularly preeclampsia, an assumption premised on “inherent racial biological differences.”9,10 Now, it is more widely understood that racism has biological effects, and significant research has shown that Black birthing people’s experiences of and exposures to systemic racism drive disparities in HDoPs.11–18 One of the most salient and long-standing manifestations of place-based structural racism in the United States is residential segregation,19,20 which, despite being illegal since the passage of the Civil Rights Act of 1964, remains a key context in the lives of Black and non-Black people of color in the United States.21,22 Research has shown that racialized residential segregation, especially when compounded with concentrated poverty, underlies Black residents’ disproportionate exposures to chronic and psychosocial stressors,19,20 police brutality,23,24 and fewer opportunities, limiting opportunities for upward social mobility and negatively impacting timely entry into prenatal care.15,25,26 This evidence reinforces a recent conceptual framework describing how segregation concentrates disinvestment in neighborhoods, creating feedback loops of poor infrastructure, limited access to health care providers, inadequate transportation, environmental hazards, and psychosocial stress during pregnancy. 27 Although existing studies explore the effects of residential segregation on maternal and neonatal health, less focus has been placed on its impact on prenatal service accessibility.
Several state and federal initiatives aim to enhance timely entry into prenatal care and access to services, improving maternal and newborn outcomes.28–34 For instance, North Carolina’s Baby Love program increased the likelihood of first-trimester prenatal care by 4.8 percentage points. 32 However, studies highlight stark racial disparities; one study found Black–White differences in timely care entry (74.81% vs. 89.63%). 35 These studies often focus on individual socioeconomic status, such as income and education, and rarely consider the role of residential segregation in shaping these factors. Delayed entry hampers risk assessment and early identification of high-risk pregnancies for preeclampsia. According to the American College of Obstetrics and Gynecology and the US Preventive Services Task Force, early screening for preeclampsia risk factors is vital for timely interventions (e.g., monitoring, low-dose aspirin, care management) that may reduce morbidity and mortality.36,37 Evidence suggests that segregation-related stressors and resource gaps persist beyond initial entry, potentially reducing adherence to recommended screenings and continuity of in-person management for high-risk pregnancies.38,39 Theoretical models of implicit bias further explain how provider attitudes and stereotypes can shape clinical decision-making during risk screening and care management, leading to underestimation of symptoms, delayed interventions, and diminished trust among Black patients. 40 A 2022 systematic review and meta-analysis involving 24 studies found that self-reported racial discrimination was significantly associated with increased odds of preterm birth (OR 1.40, 95% CI 1.17–1.68) and low birth weight. 41 However, the link between residential segregation and care processes, such as risk screening and face-to-face care management, remains less understood. This gap underscores the need for research that examines structural determinants that influence access to care across the pregnancy continuum.
This study aims to examine the association of residential segregation with timely entry into prenatal care, subsequent risk screening, and care management among Medicaid enrollees at a high risk of developing preeclampsia. The potential benefits of this research are significant, as it could lead to improved maternal health care for high-risk populations. Hereafter, we use the term neighborhood deprivation for residential segregation, which is consistent with the literature.17,19,42,43 We pose the following hypotheses: High-risk pregnant individuals living in the most deprived neighborhoods will have a lower likelihood of timely entry into prenatal care, risk screening, and receipt of care management compared with those living in the most privileged neighborhoods. Black birthing individuals living in the most deprived neighborhoods would have a lower likelihood of timely entry into prenatal care, risk screening, and receipt of care management compared with White birthing individuals in the most deprived neighborhoods.
Methods
Setting
In collaboration with the Community Care of North Carolina (CCNC), the North Carolina Medicaid program launched a voluntary Pregnancy Medical Home (PMH) program in 2011 to improve the quality of care for pregnant Medicaid beneficiaries. 44 Under this program, pregnant individuals and providers complete a standardized risk screening at the first prenatal visit, were given a risk score called the Maternal–Infant Compatibility Score, and were referred to the Care Management for High-Risk Pregnancies program at the local health departments if the score was ≥200, and those with a score of >500 received more intensive care management. 45 The care manager provided additional touch points and referred for higher levels of care and social support when needed (e.g., transportation, housing). By 2020, 95% of providers were participating in the PMH program. On July 1, 2021, North Carolina Medicaid transitioned from a single-payer fee-for-service model to a capitated model through five prepaid health plans, replacing the PMH program with a mandatory Pregnancy Management Program. This program maintained universal risk screening and care management services through local health departments. 46
Data Sources
This study uses North Carolina Medicaid claims data linked with birth certificate and CCNC’s pregnancy risk screen and care management data from January 1, 2017, to February 28, 2020, approved for reuse 45 by CCNC and the NC Department of Health, and was made available by the Cecil G. Sheps Center at UNC Chapel Hill. We also linked the US Census Bureau’s 5-year American Community Survey (ACS) estimates (2016–2020), which are publicly available. The pregnancy risk screen comprises 30 items covering obstetric (e.g., gestational hypertension), medical (e.g., autoimmune disorders), and psychosocial factors (e.g., food insecurity), which are partly self-reported and assessed clinically. 44 Medicaid claims, birth certificate, pregnancy risk screen, and care management data were linked using the birth key, resulting in a 97% match rate. The ACS is a comprehensive nationwide survey that provides communities with social, economic, housing, and demographic data, 47 offering a representative sample of the noninstitutionalized US population. It was linked to the analytic file using the maternal county of residence.
The sample included 53,000 individuals aged 15–45, identified as NHB or non-Hispanic White (NHW), who had ≥1 preeclampsia risk factor. Participants had their last menstrual period between December 15, 2016, and March 31, 2019, to capture their prenatal and postpartum periods, and had prenatal Medicaid coverage for ≥6 months. Individuals with emergency Medicaid were excluded because of the limited window of observability. Table 1 lists the preeclampsia risk factors used in this study. Figure 1 illustrates sample selection and distribution.

Sample selection criteria and distribution. ICE = Index of Concentration of the Extremes.
Preeclampsia Risk Factors Identified by the US Preventive Task Force and the American College of Obstetrics and Gynecology

Variables included in the analysis. Other variables were either unavailable or had high levels of missingness.
These variables were available for only those who had completed risk screening and hence were included only in the statistical models for face-to-face care management.
Race was not included as a risk factor; instead, it was included as a separate variable in the models.
The income variable was not available. However, the study included only Medicaid enrollees who were under 138% of the federal poverty level, hence a homogenous group.
Dependent and Independent Variables
The outcomes include timely entry into prenatal care, risk screener completion, and face-to-face care management services. All outcome variables were coded as binary. Timely entry was defined as starting prenatal care at or before 13 weeks of gestation, consistent with the literature and clinical guidelines.34,35,48
The Index of Concentration of the Extremes (ICE) is a parsimonious measure of area-level segregation49–51
that captures spatial and social polarization by quantifying extremes of deprived and privileged social groups and thus proxies area-level racialized and economic segregation,49,52–55 and has been commonly examined for the association with maternal and infant outcomes,42,43,52–54,56 including HDoPs.16–18
We used the US Census ACS 5-year estimates (2016–2020) to generate three ICE measures for county-level distribution of racial segregation and economic deprivation: ICErace, ICEincome, and ICErace+income. The ICE measures were computed using the following formula:51,52,16,58,59

Covariates
We included several covariates in the analysis based on preeclampsia risk factors (Table 1), other conditions complicating pregnancy (e.g., gestational diabetes), demographic factors (e.g., race and ethnicity), and Medicaid coverage (e.g., number of months of Medicaid coverage) (Table 2). The ICD-10 for diagnoses, as determined and identified using Medicaid claims data, is available in Supplementary File 2.
Participant Characteristics by Race/Ethnicity for the Study Sample from 2017 to 2019

Data are presented as mean (standard deviation) for continuous measures and % (n) for categorical measures.
If the Maternal–Infant Compatibility Score was more than 200, women were referred for care management.
Kidney disorders include chronic nephritic syndrome, chronic renal failure, and other chronic kidney diseases.
Maternal county of residence as rural or urban based on rural–urban commuting area codes.67
ICE = Index of Concentration of the Extremes.
Analysis
First, we computed the distributions of all variables and tested differences across NHW and NHB using the chi-square test for categorical and t-test for continuous variables. We then used separate logistic regression models to estimate the association of ICE variables with timely entry into prenatal care, risk screen completion, and receipt of face-to-face care management services. Each ICE variable was modeled separately due to collinearity. To evaluate the relationship between ICE variables and risk screening, we included timely entry into prenatal care as a covariate in the models because of its association with risk screening and care management. To assess the association between ICE variables and receipt of face-to-face care management, we restricted the sample to those who completed risk screening.
We conducted postestimation tests (Link test) to assess model specification. All models showed nonsignificant results when prediction was squared, indicating that additional interactions or squared terms may not improve fit. Theory and literature suggest that all covariates could cause heteroskedasticity. For example, differences in timely entry, risk screening, or management between the urban and rural populations can lead to variances and unequal scatter of residuals. The likelihood ratio tests were significant for each model, confirming that the included variables contributed to heteroskedasticity. We compared the fit of the heteroskedastic probit model with the logit and probit models. Detailed model comparisons are in Supplementary File 3. We present results from heteroskedasticity-adjusted models and include year-fixed effects to account for unobserved, time-specific factors that affect outcomes across years. To estimate differential effects by race, we examined whether there are statistically significant differences in the average marginal effects of ICE indices on timely prenatal care, risk screening, and management between NHB and NHW high-risk pregnant individuals. We computed average marginal effects of NHW and NHB from the main models and then tested the null hypothesis
Results
Our sample comprised 53,000 pregnant individuals: 27,024 NHB and 25,976 NHW. NHB individuals had lower rates of timely prenatal care (59.98% vs. 70.13%) but slightly higher risk screening completion (78.68% vs. 77.68%). Among those who had completed risk screening, NHB individuals received more face-to-face care management (64.07% vs. 57.42%) compared with NHW. (Table 2). Table 3 presents participant characteristics further stratified by completion of risk screening. Individuals who completed risk screening had more preeclampsia risk factors (NHW mean 1.53 vs. 1.32; NHB 1.63 vs. 1.38) and a higher prevalence of prepregnancy type 1/2 diabetes, kidney disorders, and gestational hypertension but were less often primiparous and less often had BMI >30; they also had longer prenatal member months, consistent with greater continuity in coverage and care. Furthermore, substance use and smoking were more common among those who completed risk screening. Additional stratification of participant characteristics by ICE variables is available in Supplementary File 4.
Participant Characteristics by Race/Ethnicity, Further Stratified by Completion of Risk Study for the Study Sample from 2017 to 2019

Data are presented as mean (SD) for continuous measures, and % (N) for categorical measures.
These variables were only available for those who completed risk screening; hence, the obstetric history of preeclampsia was not included as a risk factor in the statistical models.
Kidney disorders include chronic nephritic syndrome, other chronic kidney diseases, and acute and chronic renal failure.
ICE, Index of Concentration of the Extremes.
We hypothesized that high-risk pregnant individuals in the most deprived neighborhoods, based on race and income, would have a lower likelihood of timely entry into prenatal care, risk screening, and care management compared with those in the most privileged neighborhoods. We found a significantly lower likelihood of timely entry, risk screening, and care management among individuals in deprived neighborhoods, assessed by race (ICErace) and combined race and income (ICEincome+race). However, a positive association was found between ICEincome and timely entry into prenatal care and risk screening, indicating that individuals in economically deprived neighborhoods were more likely to enter prenatal care during the first trimester and complete risk screening.
Timely Entry into Prenatal Care
The adjusted multivariate logistic regression model revealed that pregnant individuals in the most deprived neighborhoods based on race (ICErace) were 11.1 percentage points less likely to enter prenatal care during the first trimester (standard deviation [SE]: 0.8; p value: 0.000) than those in the most privileged neighborhoods, all else constant (Table 4). This trend persisted in the second (8.5 percentage points, SE: 0.8; p value: 0.000), third (9.0 percentage points, SE: 0.7; p value: 0.000), and fourth (8.5 percentage points, SE: 2.4; p value: 0.000) ICErace quintiles. We found that those in the most deprived neighborhoods based on combined race and income (ICEincome+race) had a 9.5 percentage point (SE: 0.7; p value: 0.000) lower likelihood of entering prenatal care in the first trimester compared with those in the privileged neighborhoods, all else constant. Similar patterns were observed for the second (11.2 percentage points, SE: 0.8; p value: 0.000), third (8.9 percentage points, SE: 0.8; p value: 0.000), and fourth (8.6 percentage points, SE: 0.7; p value: 0.000) quintiles, all else constant. No statistically significant differences were found in the average marginal effect of ICErace or ICEincome+race on timely access by race/ethnicity (Table 5). Our estimates showed a significant positive average marginal effect of ICEincome on timely prenatal care, with pregnant individuals living in the most deprived neighborhoods based on income having a 5.4 percentage point (SE: 2.4; p value: 0.002) higher likelihood of entering prenatal care during the first trimester compared with those in the most privileged neighborhoods, all else constant. We also found a statistically significant difference in the average marginal effect of ICEincome on timely entry into care by race; NHW individuals in deprived counties had a lower likelihood of entering prenatal care (6.8 percentage points; SE: 1.4) compared with NHB individuals (4.3 percentage points; SE: 1.4).
Average Marginal Effect of Index of Concentration of the Extremes-Race, Index of Concentration of the Extremes-Income, and Index of Concentration of the Extremes-Race plus Income on Timely Entry into Prenatal Care, Risk Screening, and Receipt of Care Management Services

Results are presented as marginal effects (confidence interval); p value. The Index of Concentration of the Extremes (ICE) variables are in quintiles, ranging from 1 to 5, with 1 indicating the least privileged and 5 the most privileged. The reference categories are the most privileged (i.e., the ICE quintile 5).
Missing observations of timely entry into care were dropped from the analysis.
Health-related social needs are not included in timely entry into care and risk screening models because of perfect prediction.
Conditional on completing risk screening.
Differential Effects of Index of Concentration of the Extremes on Timely Entry into Prenatal Care, Risk Screening, and Receipt of Face-to-Face Care Management by Race (non-Hispanic Black vs. non-Hispanic White): Average Marginal Effects and Wald Tests
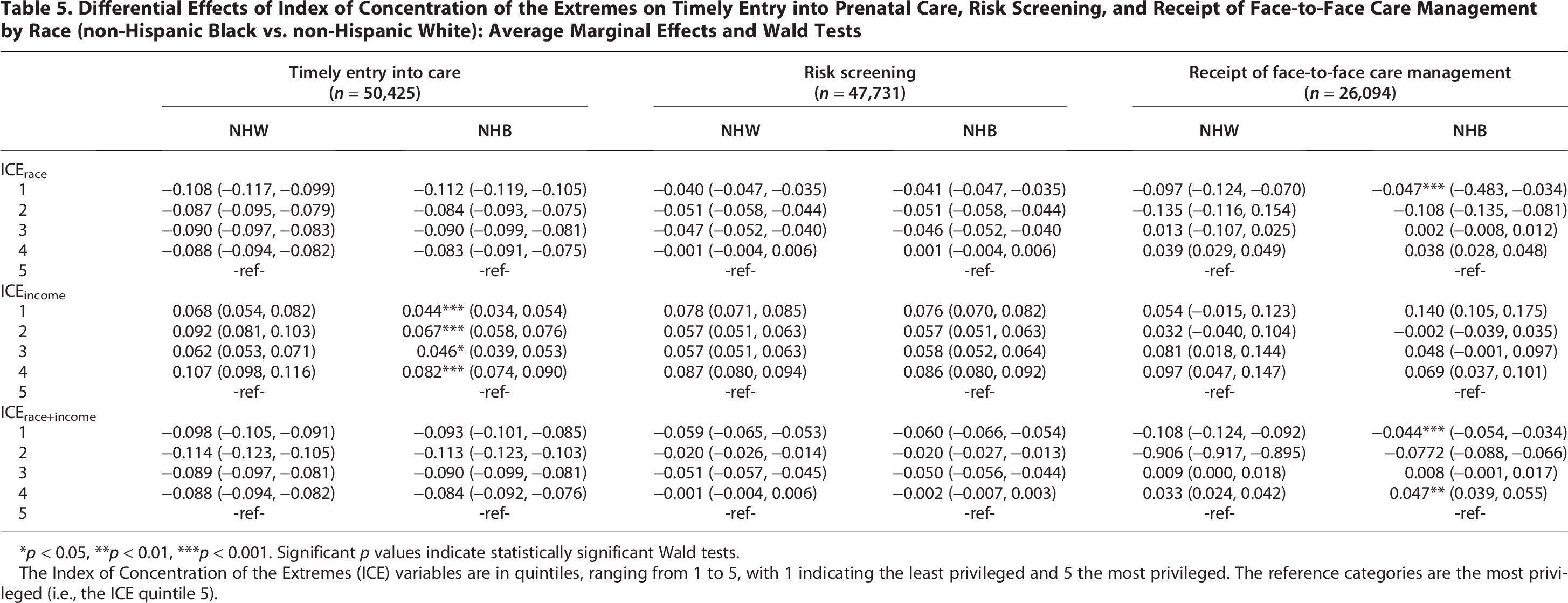
*p < 0.05, **p < 0.01, ***p < 0.001. Significant p values indicate statistically significant Wald tests.
The Index of Concentration of the Extremes (ICE) variables are in quintiles, ranging from 1 to 5, with 1 indicating the least privileged and 5 the most privileged. The reference categories are the most privileged (i.e., the ICE quintile 5).
Completion of Risk Screening
The adjusted logistic regression indicated that pregnant individuals in the most deprived counties, based on race (ICErace), had a 4.1 percentage points lower likelihood of completing risk screening (SE: 0.6; p value: 0.000) than those in the most privileged counties, all else being constant (Table 4). The effect remained consistent for the second and third quintiles, while the fourth was not statistically significant. For ICEincome+race, individuals in the most deprived neighborhoods showed a 6.0 percentage point lower likelihood of completing risk screening (SE: 0.6; p value: 0.000) compared with those in privileged neighborhoods. The effect for ICEincome+race decreased for the second and third quintiles. Similar to timely entry into care, ICEincome had a statistically significant positive effect on risk screening, with individuals in the most deprived income neighborhoods having a 7.7 percentage point higher likelihood of completing screening (SE: 0.7; p value: 0.000) than those in privileged neighborhoods, consistent across the second, third, and fourth quintiles. We found no statistically significant difference in the average marginal effect of ICErace, ICEincome+race, and ICEincome on risk screening completion by race/ethnicity (Table 5).
Receipt of Face-to-Face Care Management
Among those who completed risk screening, pregnant individuals in the most deprived counties based on race had an 8.0 percentage point (SE: 1.1; p value: 0.000) lower likelihood of receiving face-to-face care management compared with those in the most privileged neighborhoods. The average marginal effect of ICEincome+race indicated that pregnant individuals in the most deprived counties had a 7.1 percentage point (SE: 1.0; p value: 0.000) lower likelihood, while those in the second most deprived counties had an 8.3 percentage point lower likelihood (SE: 0.9; p value: 0.000) of receiving face-to-face care compared with their counterparts in the most privileged counties (Table 4). There is a significant difference in average marginal effects of ICErace and ICEincome+race on receipt of face-to-face care management by race/ethnicity, with NHW individuals in the least privileged neighborhoods having a lower likelihood of receiving face-to-face care management than NHB individuals (ICErace: −9.7; SE: 2.7 vs. −4.7; SE: 1.3; ICEincome+race: −10.8; SE: 1.6 vs. −4.4; SE: 1.0) in the least privileged neighborhoods. Furthermore, NHB individuals in the fourth quintile had a higher likelihood of receiving face-to-face care management services compared with NHW individuals in the same quintile (0.047; SE: 0.011 versus 0.033; SE: 0.09). No statistically significant effect of ICEincome on receiving face-to-face care management was found (Table 5). Average marginal effects of covariates on prenatal care entry, completion of risk screening, and receipt of care management services are available in Supplementary File 3.
Discussion
Our findings highlight the association of neighborhood deprivation, particularly ICErace and ICErace+income, with timely prenatal care entry, risk screening completion, and face-to-face care management. The association with ICErace+income weakened, showing that race-based neighborhood deprivation (ICErace) is the strongest predictor of these services. Pregnant individuals in the most racially and economically deprived neighborhoods were less likely to access essential prenatal services than those in privileged areas. These disparities likely stem from structural barriers such as limited health care access, transportation issues, financial hardship, and systemic racism. Conversely, income-based neighborhood deprivation (ICEincome) was associated with a slightly higher likelihood of timely care entry and risk screening in economically deprived neighborhoods, likely due to the Medicaid-managed PMH program, a public health initiative aimed at improving access and screening rates among low-income individuals. 61 Next, we discuss these findings in detail.
Our study also showed a negative association of neighborhood deprivation based on race (ICErace) and race and income combined (ICErace+income) on timely access to prenatal care, risk screening, and receiving face-to-face care management with pregnant individuals in the most racially and economically deprived counties with a lower likelihood of accessing these resources compared with those living in the most racially and economically privileged counties. The negative association highlights the added challenges faced by individuals living in these communities. Our results align with existing evidence that racially marginalized populations often encounter significant barriers to accessing first-trimester prenatal care, including geographic isolation, financial hardship, limited availability of care, and distrust in the health care system,15,55,56,64,65 as individuals fear mistreatment or worry that their concerns will not be taken seriously.62,65 These factors may contribute to delayed or foregone care and may undermine well-intentioned efforts to improve maternal health outcomes, such as HDoPs. Targeted strategies could include community-based care models that expand identification and outreach in underserved neighborhoods and risk screening through interventions such as mobile health clinics and community health workers. In addition, health care systems must continue to strengthen patient-centered models that build trust and validate the lived experiences of Black patients in racially and economically deprived areas. Future studies can focus on designing and testing targeted community-based interventions to close racial gaps in health care access and improve maternal health equity.
Our study showed that neighborhood deprivation based on income (ICEincome) was associated with a slightly higher likelihood of timely entry into care and risk screening in the most economically deprived neighborhoods. This may be attributed to the Medicaid-managed PMH program 61 based on several factors. Medicaid eligibility is primarily based on income, so interventions target economic barriers such as access to providers, transportation, or scheduling. Improvements may be more evident among income groups due to alignment with financial constraints. However, it is crucial to note that pregnant individuals in economically privileged neighborhoods have lower access to face-to-face care management services, suggesting that economic deprivation alone does not fully explain racial inequities in prenatal care access. Prior research shows that racial discrimination and implicit bias persist across socioeconomic strata, influencing clinical decision-making and patient experiences even among higher income Black women.40,66 These patterns underscore that factors, such as provider bias, differential treatment, and systemic racism, may operate independently of neighborhood privilege and may contribute to disparities in risk screening and care management uptake. These structural inequities may not be fully addressed by the PMH, which aims to enhance service delivery but not address inequities from structural racism. Future studies may focus on disentangling the effects of structural racism from socioeconomic disadvantage and ensuring that interventions address racial inequities beyond neighborhood deprivation, as well as exploring policy levers for racial equity-centered program design.
Our study further highlights that upon entry into care, NHB individuals demonstrate a greater likelihood of receiving face-to-face care management compared with NHW individuals, particularly in neighborhoods marked by racial (ICErace) and racial-economic deprivation (ICErace+income). This pattern may result from several intersecting factors. NHB individuals residing in these areas exhibit greater clinical and social needs, prompting more intensive care management efforts. In addition, public health initiatives, such as PMHs, may prioritize NHB communities for targeted interventions to reduce disparities, thereby enhancing access to in-person care management services. These findings suggest that efforts to mitigate inequities may be more actively implemented in racially and economically marginalized communities once access is established.
This study has several limitations. First, selection bias may be present because timely entry into care, risk screening, and receipt of face-to-face care management services are not randomly distributed. Our data are drawn from the PMH program, which limits the ability to compare associations among Medicaid enrollees who are not part of the program. It is possible that PMH participation mitigates the association between ICE variables and outcomes; without this program, these associations may be stronger. Future research could apply methods such as propensity score matching, instrument variable, or synthetic control approaches to better address this bias.
Second, omitted variable bias is possible; unmeasured factors such as patient preferences may correlate with covariates such as maternal education, potentially biasing estimates toward the null. Third, neighborhood-level analysis was limited to the county level due to data constraints and sample size limitations, which may not capture within-county variability. However, given that the PMH program operates at the county level, these findings remain relevant for informing county-level interventions. Future studies should explore census-track-level analysis to assess whether these findings persist at finer geographic scales. Fourth, Black individuals may receive higher risk scores within the PMH program due to higher prevalence among them, which could explain their greater likelihood of receiving care management. We addressed this by including fixed effects of overall risk burden in the models using a count variable. Finally, generalizability is limited, as the analysis includes only Medicaid beneficiaries receiving care through PMHs in North Carolina. Future studies should consider broader populations, including those with other insurance types and care models. Despite these limitations, this study leverages a robust, state-level dataset to examine the impact of neighborhood deprivation on prenatal care access, offering valuable insights into Medicaid policy in North Carolina.
Conclusion
In conclusion, this study demonstrates that neighborhood deprivation based on race and income is significantly associated with reduced access to timely prenatal care, risk screening, and face-to-face care management. While income-based deprivation alone was linked to slightly improved access, likely due to targeted programs such as the PMH, racial deprivation continues to pose substantial barriers. Addressing these disparities will require equity-focused interventions and targeted outreach to ensure that all pregnant individuals receive timely and appropriate prenatal care.
Authors’ Contributions
M.A.: Conceptualization (lead), investigation (lead), formal analysis (lead), and writing—original draft (lead). C.M.S.: Conceptualization (supporting), supervision (supporting), investigation (supporting), formal analysis (supporting), and writing—review and editing (supporting). M.K.M.: Conceptualization (supporting), writing—review and editing (supporting), and writing—review and editing (equal). L.K.: Data curation (supporting) and writing—review and editing (supporting). M.E.D.: Formal analysis (supporting) and writing—original draft (supporting). V.A.L.: Conceptualization (supporting), formal analysis (supporting), and writing—original draft (supporting). A.M.P.: Conceptualization (supporting), supervision (lead), investigation (supporting), formal analysis (supporting), and writing—review and editing (supporting).
Footnotes
Acknowledgments
The authors extend their sincere gratitude to the Community Care of North Carolina and the North Carolina Department of Health and Human Services for allowing the reuse of the dataset and the Cecil G. Sheps Center for Health Services Research for providing access to the dataset.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This article is part of doctoral dissertation and did not have any funding support.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.