
Abstract
Objectives:
This review aimed to report the estimated pooled level of prevalence, risk factors, and birth outcome of hypertensive disorder of pregnancy in Ethiopia, in 2024.
Design:
A systematic review and meta-analysis approach was utilized.
Data Sources and Methods:
PubMed/MEDLINE, Google Scholar, African Index Medicus, Web of Science, and CINHAL (EBSCO) search was carried out. The result was written according to the PRISMA-updated guidelines. To estimate the pooled prevalence and effect sizes, a random-effect model was used. Heterogeneity was assessed and investigated using I2 test statistics and meta-regression, respectively. Publication bias was assessed using funnel plot and Egger’s test statistics. Statistical tests result at p-value < 0.05 were declared as having significance.
Result:
From a total of 52 primary studies with a total sample size of 269, 158 were included in this systematic review and meta-analysis. The pooled prevalence of hypertensive disorder in pregnancy was 8%. Egger’s test statistics (p = 0.8013) showed there is no publication bias. Having a history of kidney disease (AOR: 3.47), being rural resident (AOR: 2.5), having fruit intake during pregnancy (AOR: 0.39), being overweight (AOR: 2.24), and having multiple pregnancy (AOR: 2.1) were found to have a significant association with hypertensive disorder of pregnancy.
Conclusion:
Overall, the level of prevalence of hypertensive disorders of pregnancy in Ethiopia was significantly increasing. Having a history of kidney disease was found to have a strong association with hypertensive disorders of pregnancy among factors. The most common or dominant adverse maternal and childbirth outcomes were low birth weight, preterm birth, fifth minute low APGAR score; and eclampsia, hemolysis, elevated liver enzymes, and low platelets syndrome, and acute kidney injury. The governments and other stakeholders should work to broaden and strengthen the existing maternal and child health (MCH) practice by incorporating all possible risk factors of hypertensive disorders of pregnancy in MCH guidelines. In addition, a large-scale study is required that considers those important missed variables, especially, in the eastern part of Ethiopia.
Introduction
Hypertension (HTN) during pregnancy is defined as systolic blood pressure above 140 mmHg and/or diastolic blood pressure above 90 mmHg. Severe HTN is indicated by blood pressure measurements above 170 and 110 mmHg.1,2 HTN during pregnancy is typically diagnosed at least two times, 4 h apart, in previously normotensive women and is often accompanied by new-onset conditions after 20 weeks of gestation.3,4 Hypertensive disorders of pregnancy (HDP), including preexisting and gestational HTN, preeclampsia, and eclampsia, complicate up to 10%–21% of pregnancies, causing significant maternal and perinatal morbidity and mortality.5–9
Maternal mortality globally is alarmingly high, with 810 women dying daily from preventable pregnancy and childbirth causes, with 94% of all deaths occurring in low and lower-middle-income countries.10–12 HDP are a significant global cause of preventable maternal and fetal morbidity, accounting for 15%–18% of maternal deaths and posing a critical health threat.8,9,13,14
Globally, an estimated 2.6 million stillbirths annually, approximately 16%, occur in pregnancies complicated by pregnancy HTN. 15 Also, prematurity, fetal growth restriction, and fetal overgrowth, and the HDPs are identifiable risk factors for newborn morbidity like respiratory distress and neonatal hypoglycemia.16,17 Consequences of HDP were maternal and fetal adverse outcomes which usually characterized or include placental abruption, pulmonary edema, thrombocytopenia, hemolytic anemia, stroke, recurrent seizure, kidney damage, and liver injury intrauterine growth.9,18,19
In the past half-century, the incidence of preeclampsia and maternal mortality has decreased significantly in developed countries. However, in developing countries, the incidence rates of preeclampsia and maternal mortality are still very high. 20 The incidence increased from 16.30 to 18.08 million globally, with a total increase of 10.92 % from 1990 to 2019. Preeclampsia incidence and maternal mortality rates, however, continue to be relatively high in the developing nations.20,21
In sub-Saharan African region, pregnancy-related HTN diseases accounted for 27.2% of maternal deaths in East and Central Africa, 22.7% in Southern Africa, and 17.2% in West Africa region between 2015 and 2020. 22 Similarly, other studies conducted in Ethiopia revealed that HTN disorders during pregnancy accounted for 16%–32.5% of the causes of direct maternal deaths.23–29 Furthermore, perinatal and maternal death rates were shown to be greater in pregnant women with one of the hypertensive disorders than in the majority of low- and middle-income countries and high-income countries. 24
In Ethiopia, different primary studies indicated that the prevalence of HDP ranged from 12.5% to 25.4%.30–35 Also, there are different reports from various systematic reviews conducted in Ethiopia that reported the pooled prevalence of HDP were from 6.8% to 8%.36–38
Several studies have analyzed the risk factors for HDP, and the identified risk factors include maternal age ⩾35, rural residential area, prim gravida, null parity, positive history of abortion, twin pregnancy, lack of ANC follow-up, obesity, a family history of HTN, alcohol intake, heart failure, stroke and left ventricular hypertrophy, smoking, and positive history of diabetes mellitus (DM) were risk factors for hypertensive disorders during pregnancy.39–43
Hypertensive disorder of pregnancy among pregnant women is an outstanding public health problem and an important contributing factor for maternal and prenatal morbidity and mortality in the world especially in developing countries, especially, in Ethiopia. Goal 3 of the Sustainable Development Goals (SDGs) or agenda is to bring down the rate of maternal death worldwide to less than 70 per 100,000 live births by 2030. 44 In line with this, the government of Ethiopia has a plan to reduce maternal mortality from 401 to 140 per 100,000 live births in 2030. 45 Thus, reducing the maternal mortality ratio is one of the SDGs which is a top priority of Ethiopian government health policy. Therefore, prompt detection and handling of the fundamental aspect of obstetric care in Ethiopia is the assessment of HDP and its associated variables in pregnant women attending ANC clinics.46–48
In Ethiopia, the existing systematic review published in 2017, 2018, and 2020 focused only on either of one condition (prevalence, risk factors, or fetomaternal outcome), and they included research articles published up to 2019. After 2019, there were more than 35 primary research that were published regarding burden (incidence), risk factors, and birth outcome among women with HDP in Ethiopia, and reported inconsistent results on the prevalence, incidence, and risk factors.
The inconsistent findings that were reported in these studies are inconvenient for decision-makers, planners, programmers, legislators, and other stakeholders to identify the existing situation. Developing the right interventions and tactics to enhance mother and child health may prove difficult in this regard.
This review is crucial for improving maternal and child health, survival, social capital, and sustainable economic growth in Ethiopia. It will reveal the burden, risk factors, and fetomaternal outcomes among pregnant women with HDP, aiding existing programs. This study will provide insights into obstetrics care, aid in designing a new strategy for better outcomes, detect and track pregnant women with HTN, and serve as a baseline for further research. Therefore, this review aimed to report the overall estimated pooled level of prevalence and identify risk factors and birth outcome of hypertensive disorder of pregnancy which were not reported by other reviews in Ethiopia.
Methods
Protocol approval and registration
This review has been registered with the International Prospective Register of Systematic Reviews (PROSPERO) and registered https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023482111.
Study design, setting, and period
This study uses a systematic review and meta-analysis which included only studies conducted in Ethiopia up to 12 July 2023.
Eligibility criteria
Inclusion criteria
The Condition, Context, and Population (CoCoPop) 49 format was used to define the study question to be included as follows: Condition outcomes reported “Preeclampsia, Eclampsia, Gestational HTN, pregnancy-induced HTN, HTN during pregnancy, and Chronic HTN during pregnancy.” The context was geographical area “studies conducted in Ethiopia” and the population of interest was “Pregnant women.” Also, the population, exposure, and outcome (PEO) framework was used as follows: Population “pregnant women, and pregnant mother,” exposure “hypertensive disorder of pregnancy,” outcome “adverse birth outcome or fetomaternal outcome.” Articles reported or published only in the English language up to July 2023 were eligible for this systematic review and also unpublished studies or articles were considered.
Exclusion criteria
After careful reviewing of the searched articles, primary studies that were not relevant to the topic or did not focus on the hypertensive disorder of pregnancy, those that did not report the outcome of interest, and those that were not conducted in Ethiopia were excluded from this systematic review. In addition, during the article selection process, studies that were not fully accessible (full text not available) were excluded. However, before excluding the articles, the primary author attempted to contact them at least one time through email.
Data source and search strategy
To identify articles, a comprehensive search of PubMed/MEDLINE, Google Scholar, African Index Medicus (AIM), Web of Science, and CINHAL (EBSCO) search was carried out. In general, the following searching key terms were applied during the search and to combine searching terms using the BOOLEAN operator: “OR” and “AND” designing a search strategy, to be as comprehensive as possible (Annex I), so it is necessary to include a wide range of synonyms key terms for the each of selected terms.
Data quality assessment and extraction
The database search and selection process were processed using EndNote X20 software and Covidence online web-based software and then removing duplicates, and extracting characteristics from each article. Primary studies were screened and assessed for eligibility and quality, which was done independently by two investigators. Conflicts in this process were resolved by consensus. The JBI Critical Appraisal checklist50,51 was used for quality assessment of cross-sectional, case-control, and cohort studies, articles that scored ⩾ 75% were included in the systematic review (Annex II). Data extraction was also employed by the two investigators and also quality and consistency of the review were checked by the investigators. Variables such as authors, region, study year, sample size, proportion of HDP, and effect size are extracted.
Assessment of publication bias and heterogeneity
Examination of publication bias for each meta-analysis was checked by running a funnel plot. Significance test statistics for publication bias were assessed using Egger’s regression test. Based on the regression test result, conclusion was made whether there is publication bias or not. After analyzing and running a forest plot analysis, the heterogeneity was assessed. To assess the degree of heterogeneity cut off I2.
Data synthesis
The overall process and result of this systematic review were written according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) updated guidelines. Analysis of the variable with two outcome dichotomous data were combined to get pooled prevalence and odds ratio, as well as predictors such as pooled effect and confidence interval, based on the results obtained from the included article.
All data analysis was done using Stata Crop MP v.17 software. A forest plot with an overall effect size was utilized to describe the results quantitatively for each outcome, and tabulation was employed. The strength of the statistical evidence for the relationship, as indicated by the p-value, and the consistency of the evidence across studies formed the basis of the quantitative assessment of the pooled evidence. In instances where study heterogeneity is identified, a random effect model is utilized. Additionally, a subgroup analysis was carried out according to the area or the location of the study in which the study was conducted, as well as sensitivity analysis was performed.
Results
The process of selecting studies for systematic review and meta-analysis
A comprehensive search strategy on different databases, including PubMed, CINHAL, Web of Science, AIM, and Google Scholar, was used to retrieve the published articles. A total of 3544 articles were identified. Out of a total of 3544 articles generated from different databases (CINHAL = 25, African Index Medicus = 4, Google Scholar = 3470, PubMed = 20, Web of Science = 25) (Figure 1).
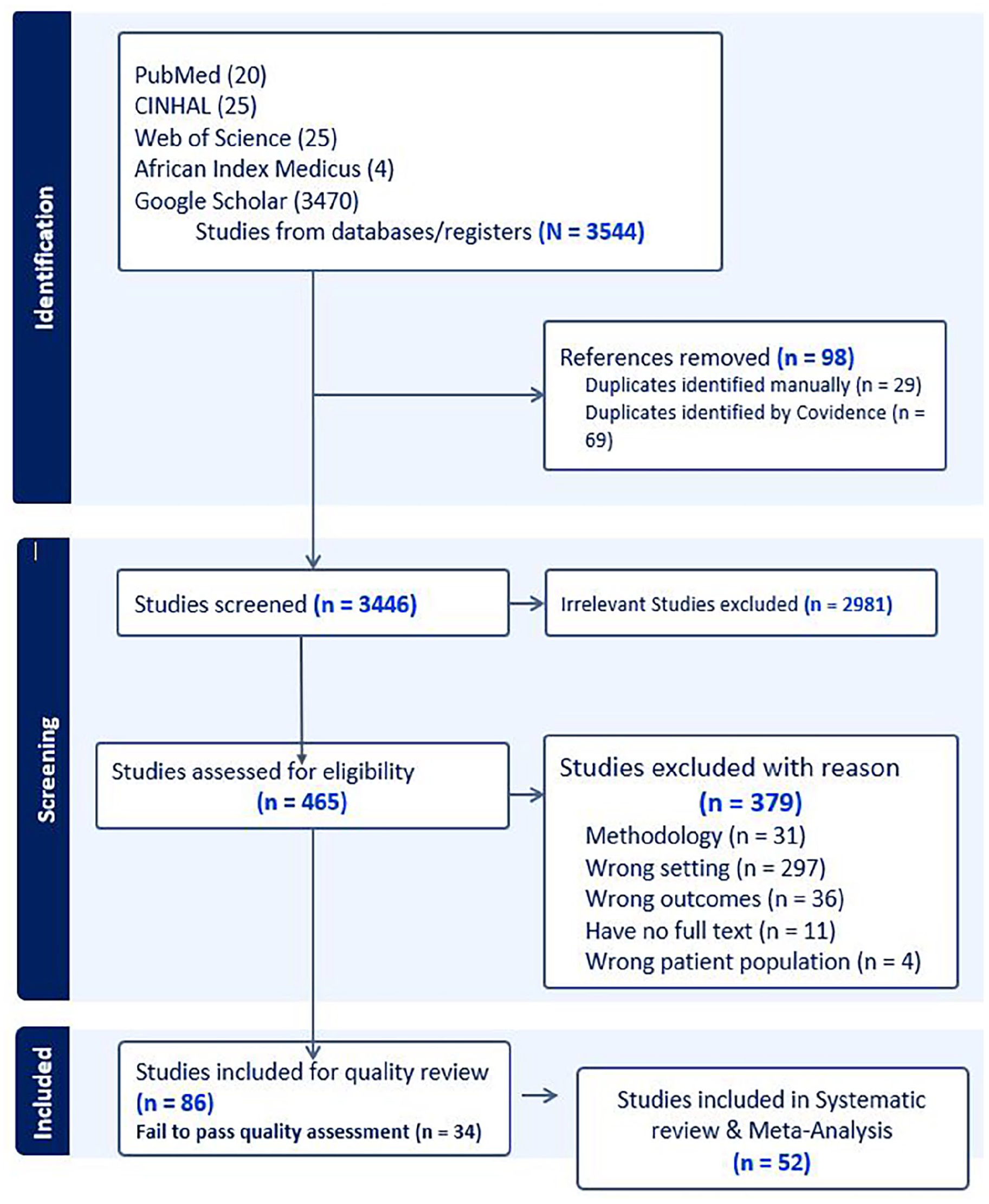
Prisma flow chart of study selection for systematic review and meta-analysis of burden, risk factors, and adverse birth outcomes of hypertensive disorder of pregnancy in Ethiopia, 2024.
Characteristics of included studies in systematic review
Finally, after quality assessment, there were a total of 52 published articles included in this systematic review that consisted of cross-sectional (28), case–control (16), and cohort (8) studies with a total sample size of 269,158. Of these, the largest sample size was 174,561 from a national survey, while the smallest sample size was 129 from the Oromia region. The majority of these studies were conducted in Amhara (17) and Southern (15) Ethiopian regions. The study included research articles published between 2011 and 2013, and 65% of these were published after 2019. The highest prevalence of HDP reported was 17.25% in Harari and the lowest rate was 1.2% reported by a multicenter survey. Among the studies included 22 that reported prevalence rates, 33 included risk factors, and 19 reported adverse birth outcomes (Table 1).
Descriptive summary of 52 studies included in the systematic review of burden, risk factor, and birth outcome of HDP in Ethiopia 2024.

Pooled prevalence of hypertensive disorder of pregnancy in Ethiopia
The pooled prevalence of hypertensive disorder of pregnancy among pregnant women in Ethiopia was 8% (95% CI: 7–9). There was high heterogeneity between the included studies which were exhibited by I2 = 98.66%, p = 0.001) (Figure 2). Therefore, to deal with and investigate the source of heterogeneity subgroup analysis, meta-regression and sensitivity analysis were done.

Pooled prevalence of hypertensive disorder of pregnancy among pregnant women in Ethiopia, 2024.
Subgroup analyses of the pooled estimated prevalence of HDP were performed according to the study region to explore the source of heterogeneity. There is high heterogeneity within studies conducted in the Amhara Region and Southern Ethiopia which is I2 = 96.7% and 93.8%, respectively (Figure 3).

Subgroup analyses of pooled estimated prevalence of hypertensive disorder of pregnancy, 2024.
Heterogeneity investigation through Galbraith plot and meta-regression
Galbraith plot shows a visual impression of the amount of heterogeneity in meta-analysis, As shown in the figure majority of the studies are out of the line of regression above and below line ±2 or 95% boundaries of the overall standardized, so this means they are a source of heterogeneity. The meta-regression r-square result indicates that around 5.3% of heterogeneity in the meta-analysis was introduced due to sample size differences in the study (Figure 4).

(a) Galbraith plot shows the source of heterogeneity, (b) meta-regression to investigate the source of heterogeneity in pooled estimate of hypertensive disorder of pregnancy among pregnant women in Ethiopia, 2024.
Sensitivity analysis on the pooled prevalence of hypertensive disorder of pregnancy
The displayed effect size for each study corresponds to an overall effect size computed from a meta-analysis excluding that study. The omission of study 13 83 or 9 74 seems to have a relatively larger influence (when compared with other studies) on the estimation of the overall prevalence. Omitting study 13 causes the overall prevalence to increase by roughly 0.3% (from 8% to 8.3%, whereas omitting studies 15 and 19 causes the overall prevalence to decrease by roughly 0.72% (8%–7.28%) (Figure 5).

Sensitivity analysis on the pooled prevalence of hypertensive disorder of pregnancy, 2024.
Assessment of publication bias in the pooled prevalence of hypertensive disorder of pregnancy
There is evidence of publication bias from the visual inspection of the funnel plot and statistical significance. Also, the nonparametric (Trim and fill method) test indicates evidence of publication bias. Based on the contour-enhanced funnel plot, it appears that a lot of studies were missing from both the significant and nonsignificant regions of the funnel plot. Under the funnel plot, more studies are missing in both regions. Therefore, the asymmetry in this meta-analysis is due to other factors such as heterogeneity (Figure 6).
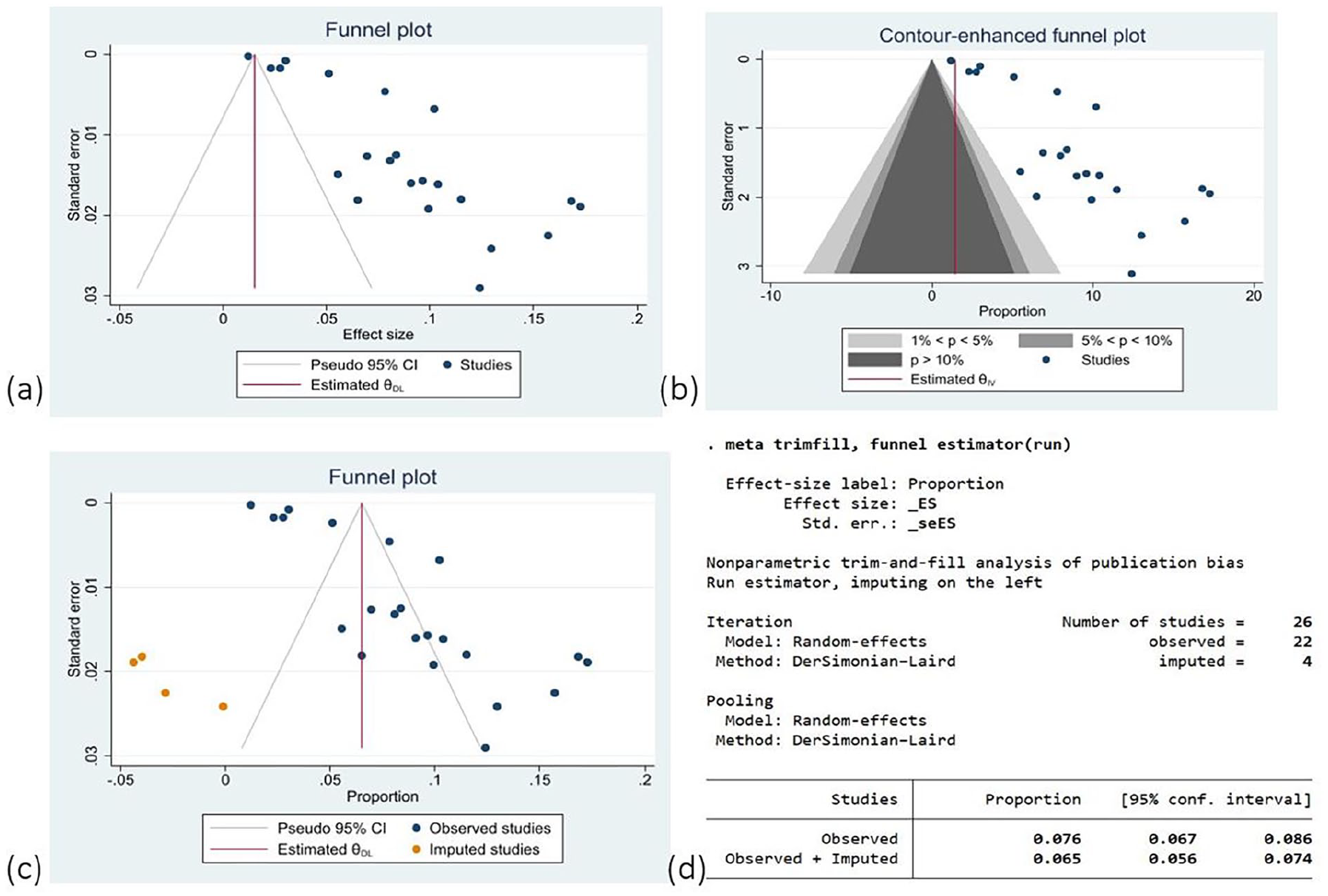
(a) Funnel plot, (b) counter-enhanced plot, (c and d) Funnel plot and trim-and-fill method for assessment of publication bias in the pooled prevalence of hypertensive disorder of pregnancy, 2024.
Cumulative meta-analysis (trend analysis) of pooled prevalence of HTN disorder of pregnancy
To explore the trend in the proportion or prevalence rate, we have used a year in which research was conducted. From year to year when more research was conducted, the overall prevalence of HTN disorder in pregnancy significantly (p-value) increases (Figure 7).

Cumulative meta-analysis (trend analysis) of pooled prevalence of HTN disorder of pregnancy, 2024.
Risk factors associated with hypertensive disorder of pregnancy and assessment of publication bias
The finding of this meta-analysis showed several significant factors associated with HDP among these factors and the following were those variables that showed a strong association with HDP. Women having a history of kidney disease were 3 (AOR: 3.47; 95% CI: 1.2–5.7) times more likely to develop HDP than women who have no history of kidney disease. Women who have a family history of HTN were 3 (AOR: 3.57; 95% CI: 2.3–4.8) times more likely to develop HDP than women who have no family history of HTN. Those women who have a history of preeclampsia were 5 (AOR: 5.5; 95% CI: 2.7–8.2) times more likely to develop HDP than women who have no history of preeclampsia (Table 2).
Determinant factors associated with hypertensive disorder of pregnancy among pregnant women in Ethiopia 2024.
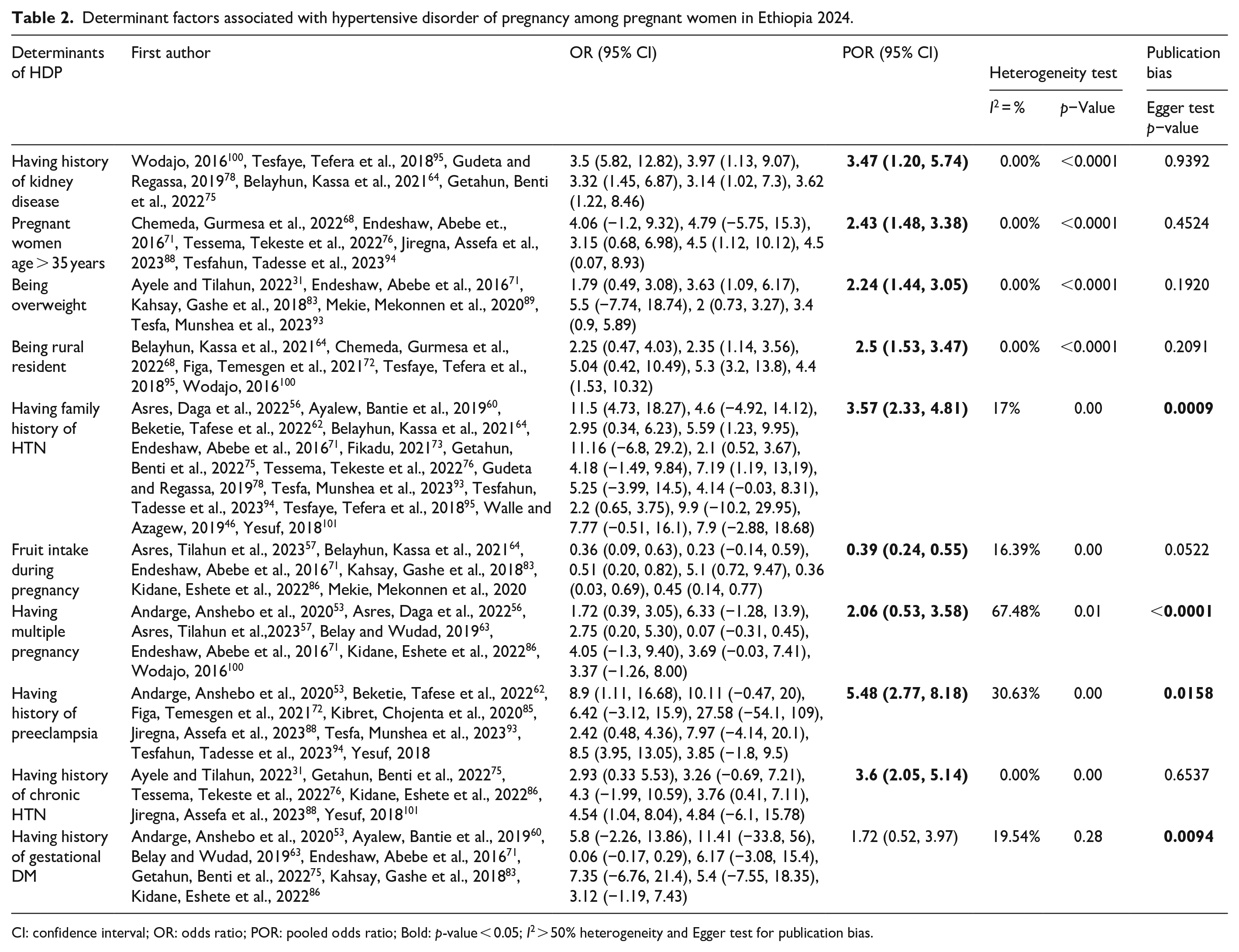
CI: confidence interval; OR: odds ratio; POR: pooled odds ratio; Bold: p-value < 0.05; I2 > 50% heterogeneity and Egger test for publication bias.
Adverse fetomaternal outcome among pregnant women with HDP in Ethiopia
In this systematic review of included studies, 19 of them reported different adverse fetomaternal outcomes among pregnant women with HDP. The most common adverse fetal outcomes were low birth weight, preterm birth, and fifth-min low Apgar score. The dominant adverse maternal outcome was eclampsia, hemolysis, elevated liver enzymes and low platelets (HELP) syndrome, acute kidney injury pulmonary edema, and disseminated intravascular coagulation (DIC) (Table 1).
Discussion
According to the results of this meta-analysis, the pooled prevalence of HDP in Ethiopia was estimated to be 8%, which is higher than a systematic review and meta-analysis published in 2018 which included 13 primary studies that pooled the prevalence of HDP in Ethiopia that was 6.07%, 38 similarly, other review published in 2020 which included 22 primary studies reported the pooled prevalence of HDP in Ethiopia was 6.82%. 37
Regional variation in HDP was observed, and the highest prevalence of HDP (17%) was reported in a study done in Harari Region. The lowest prevalence of HDP (3%) was observed in the Tigray Region. These regional variations may result from variations in lifestyle, educational attainment, and use of MCH services.
In addition, most of the studies included in this meta-analysis were conducted in the Amhara Region which shows that the prevalence of HDP was 9% with a high source of heterogeneity between studies.
The finding of this meta-analysis also showed the risk of HDP increased with increasing age. Women aged > 35 years old were 2.43 times more likely to develop HDP than women aged < 35 years old during their pregnancy. This finding is consistent with results reported from similar studies in Ethiopia, Kenya, Asia, China, and Latin America, women aged > 35 years were having a risk of developing HDP than women aged < 35 years during their pregnancy.37,102–105 This is due to the fact that there is a higher risk of cardiovascular problems in this age group compared to younger women.104,106
In this meta-analysis, women who have had a previous history of preeclampsia were five times more vulnerable to develop HDP as compared with those women who have no previous history of preeclampsia. This was consistent with the findings reported from the study conducted in Ethiopia and China.37,102
Similarly, having a family history of HTN and a family history of DM could also increase the risk of developing HDP compared with their counterparts. These findings are in line with the studies conducted in Ethiopia, China, Swedish Medical Center, and US hospitals.37,102,107,108
Limitation of the study
There is geographical and selection bias, which means there was an underrepresentation of certain areas and the included or selected studies may not be representative. Also, there was high heterogeneity reported in this review, which is reported from the result of pooled estimates of the prevalence of hypertensive disorder in pregnancy. Even if meta-regression was computed to explore sources of heterogeneity, the conclusions drawn from highly heterogeneous studies are less generalizable, specifically for the eastern part of Ethiopia because there were a low number of articles included or found from the eastern part of Ethiopia. The underrepresentation of studies from the eastern part of Ethiopia means that the pooled estimates may not accurately reflect the prevalence of hypertensive disorders in pregnancy in this region.
Conclusion and recommendation
Conclusion
This systematic review and meta-analysis revealed that the level of prevalence of HDP in Ethiopia is increasing. Having a history of kidney disease, having a family history of HTN, having a history of preeclampsia, and having a history of chronic HTN, were found to have a strong association with HDP factors.
The most common adverse fetal outcomes were low birth weight, preterm birth, and a fifth-min low APGAR score. The dominant adverse maternal outcomes were eclampsia, HELP syndrome, acute kidney injury pulmonary edema, and DIC.
In the eastern part of Ethiopia, this condition was not well studied when compared to other areas, this is a high gap. There is a lack of articles conducted at the community level, and those published studies missed some very important variables that need attention or focus such as maternal mental health status, quality of life, and some specific modifiable socioeconomic variables. The majority of the studies that failed to pass quality assessment were those published in low-quality journals.
Recommendation
The finding of this review suggests the need to strengthen the existing strategies for prevention, effective intervention, and developing policy to decrease the burden and adverse birth outcome of hypertensive disorder of pregnancy by working on identified risk factors with a collaboration of nongovernmental organizations, and other stakeholders.
The study recommends enhanced screening and monitoring for hypertensive disorders in pregnancy, particularly among high-risk groups such as kidney disease, overweight individuals, and multiple pregnancies. Rural healthcare providers should be vigilant in HDP monitoring. Increased fruit intake during pregnancy can protect against HDP, and nutritional counselling should be incorporated into prenatal care programs. Encourage further research in underrepresented regions, particularly the eastern part of Ethiopia, to gain a more comprehensive understanding of HDP prevalence and risk factors. Support longitudinal studies to track the long-term outcomes of HDP on maternal and child health, which can inform future healthcare strategies and interventions.
In addition, the Ethiopian Ministry of Health should develop and disseminate educational materials, particularly on health Information dissemination about the importance of a balanced diet during pregnancy, with a focus on the benefits of fruit intake, the importance of preconception care, antenatal care (ANC), and early detection and management of HTN during pregnancy to reduce the unwanted or negative impact of hypertensive disorder of pregnancy on the health of the mother and her child.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241274741 – Supplemental material for Burden, risk factors, and maternal postpartum and birth outcomes of hypertensive disorder of pregnancy in Ethiopia, 2024: A systematic review and meta-analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121241274741 for Burden, risk factors, and maternal postpartum and birth outcomes of hypertensive disorder of pregnancy in Ethiopia, 2024: A systematic review and meta-analysis by Astawus Alemayehu, Abebaw Demissie, Ibsa Ibrahim, Addisalem Geremew, Feysal Mohammed, Mogos Gudeta, Lamessa Oljira, Yadeta Dessie and Nega Assefa in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241274741 – Supplemental material for Burden, risk factors, and maternal postpartum and birth outcomes of hypertensive disorder of pregnancy in Ethiopia, 2024: A systematic review and meta-analysis
Supplemental material, sj-docx-2-smo-10.1177_20503121241274741 for Burden, risk factors, and maternal postpartum and birth outcomes of hypertensive disorder of pregnancy in Ethiopia, 2024: A systematic review and meta-analysis by Astawus Alemayehu, Abebaw Demissie, Ibsa Ibrahim, Addisalem Geremew, Feysal Mohammed, Mogos Gudeta, Lamessa Oljira, Yadeta Dessie and Nega Assefa in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121241274741 – Supplemental material for Burden, risk factors, and maternal postpartum and birth outcomes of hypertensive disorder of pregnancy in Ethiopia, 2024: A systematic review and meta-analysis
Supplemental material, sj-docx-3-smo-10.1177_20503121241274741 for Burden, risk factors, and maternal postpartum and birth outcomes of hypertensive disorder of pregnancy in Ethiopia, 2024: A systematic review and meta-analysis by Astawus Alemayehu, Abebaw Demissie, Ibsa Ibrahim, Addisalem Geremew, Feysal Mohammed, Mogos Gudeta, Lamessa Oljira, Yadeta Dessie and Nega Assefa in SAGE Open Medicine
Footnotes
Acknowledgements
First of all, we would like to express our thanks to the almighty God. We would also like to extend our gratitude to Haramaya University, College of Health and Medical Science for giving us this chance to conduct this study. Finally, we thank Mr. Merga Hirko for editing the language and grammatical flow.
Author contribution
All authors contributed significant work to this review: AA, NA, and LO participated in the study from inception to design, acquisition of data, analysis, and interpretation of the results. AA, AD, NA, YD, LO, AG, MG, II, and FM participated in the methods, analysis, interpretation, and writing of the manuscript of the results. Finally, all authors approved the manuscript for publication and the journal to which it has been submitted.
Availability of data and materials
At any time, the corresponding author provides an additional resource on request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.