
Abstract
Keywords
Introduction
Modern minimally invasive forefoot surgery, especially third- and fourth-generation percutaneous hallux valgus corrections using MICA (minimally invasive chevron and Akin) and META (metaphyseal extraarticular and transverse Akin) techniques, has shown excellent correction potential, safety, and clinical outcomes.1,2 These approaches minimize soft-tissue morbidity and postoperative pain without compromising correctional results, 3 and similar benefits are reported for percutaneous correction of lesser toe deformities, including bunionette deformities. 4
Although literature focuses primarily on outcomes and complications, detailed postoperative care, particularly dressing and taping methods, remains underreported. 5 Because internal fixation is often not required for percutaneous correction of lesser toes, external fixation with taping is essential to maintain alignment and correction. 6 This technical note outlines practical methods for elastic taping after percutaneous forefoot surgery.
Elastic tapes are preferable to nonelastic ones because of their lower risk of medical adhesive–related skin injury (MARSI) and improved handling.7,8 They stretch as needed, conform to anatomy, and are less likely to roll, constrict, or cut into the skin. Precut elastic tapes in different sizes, such as Mecron ReadyDressment Strips (Darco), simplify and standardize application. Alternatively, Kinesio-style elastic tapes sold by the meter can be custom cut (Figure 1).

Elastic tape cut from the meter (left), precut “long” 13.5 × 1.8 cm (middle), and precut “short” 10 × 1.4 cm (right) (Mecron Ready Dressement Strips; Raisting).
Indications
Taping of the First Ray
The key to success in third- and fourth-generation percutaneous hallux valgus surgery is a sufficient osseous correction. Large shifts and multidirectional correction require fixation, typically using one or two bevel-headed screws at the metatarsal osteotomy site. The Akin osteotomy may be left unfixed, relying on external taping for stability. 9 When the metatarsophalangeal joint (MTPJ) remains incongruent, or sesamoids are subluxed after osseous correction, a lateral soft tissue release can be performed. 10 Then, supporting MTPJ position during early healing with elastic tape is recommended to maintain alignment and allow positional adjustments until consolidation. For isolated first-ray surgery, spica dressings with gauze, off-the-shelf silicone spacers, or moldable putty forefoot splints may be used. However, interdigital spacers in the first web space can compromise alignment after correction of adjacent lesser toes, often resulting in valgus displacement. By contrast, elastic taping offers a slimmer, more compact alternative and can be self-applied by patients following proper instruction. In the outpatient setting, we recommend that patients record a video (supplemental video) of the hallux tape application for future reference and instructional use.
Taping should begin immediately in the operating room following wound closure. Percutaneous portals for osteotomies and tenotomies are closed with interrupted sutures and covered with sterile SteriStrips. In the operating room, the skin can be degreased with wound alcohol (benzinum medicinale/petroleum ether) to improve tape adhesion prior to application. In the outpatient setting, we use a dedicated adhesive spray to ensure more durable skin contact (Tenospray; BSN Medical). The nonsterile elastic tapes are then applied on top (Figure 2). The tape supports realignment of the first ray, applied in a charity-ribbon fashion with gentle medial retraction of the proximal phalanx (Figure 3). Care must be taken to avoid covering the sensitive, proximal screw insertion sites and to prevent overtensioning or hypervarization. A second overlapping tape may be added for reinforcement. The risk of adverse skin reactions, including blistering or tearing, is minimal and has been reported to be lower than with traditional nonelastic tape.7,8

Severe hallux valgus deformity preoperatively (A) and intraoperatively after fourth-generation multidirectional percutaneous hallux valgus correction and elastic taping (B). The arrow marks the small portal for the percutaneous lateral release.

The tape is applied centrally on the lateral aspect around the base of the proximal phalanx, then crossed medially in a manner similar to a charity ribbon. Rotational control can be adjusted by varying the tension of the 2 straps. Lateral (A), oblique (B), and dorsal-plantar view (C). Depending on the desired level of retention, 2 parallel overlapping strips may be applied (D).
If a dorsomedial bony prominence has been resected with the wedge burr, compression taping perpendicular to the metatarsal axis reduces capsule laxity and prevents postoperative hematoma forming between the metatarsal head and the flaccid capsula (Figure 4). The forefoot is then dressed with gauze bandages, as minor wound discharge from osteotomies is not uncommon. Tapes are renewed after suture removal, typically 2 weeks postoperatively. Patients are instructed to replace the hallux tapes whenever they come off or get wet, for a minimum period of 6 weeks.

Following resection of the bony eminence with a wedge burr, a lax joint capsule frequently can be observed. (A) Flaccid soft tissues (arrows) and the bone paste being manually expressed and subsequently thoroughly rinsed out. (B, C) Overlapping U-shaped tapes (white) used to press the capsule back onto the bone and reduce the risk of hematoma formation.
Taping of the Second to Fourth Rays
For lesser toes, where internal fixation is usually not required, postoperative stability is achieved using external taping or bandaging. 6 Compared with the alternatives of traditional nonelastic tapes or Steri-Strips, elastic tapes offer the advantage of fewer adverse skin reactions, are easier to handle, and substantially reduce the risk of cutting into the skin or causing constriction. 8
In percutaneous lesser toe correction, the goal is to obtain a flexible, straight toe without spontaneous tendency to malalignment. For the exact indications and techniques, please refer to the referenced literature.4,11
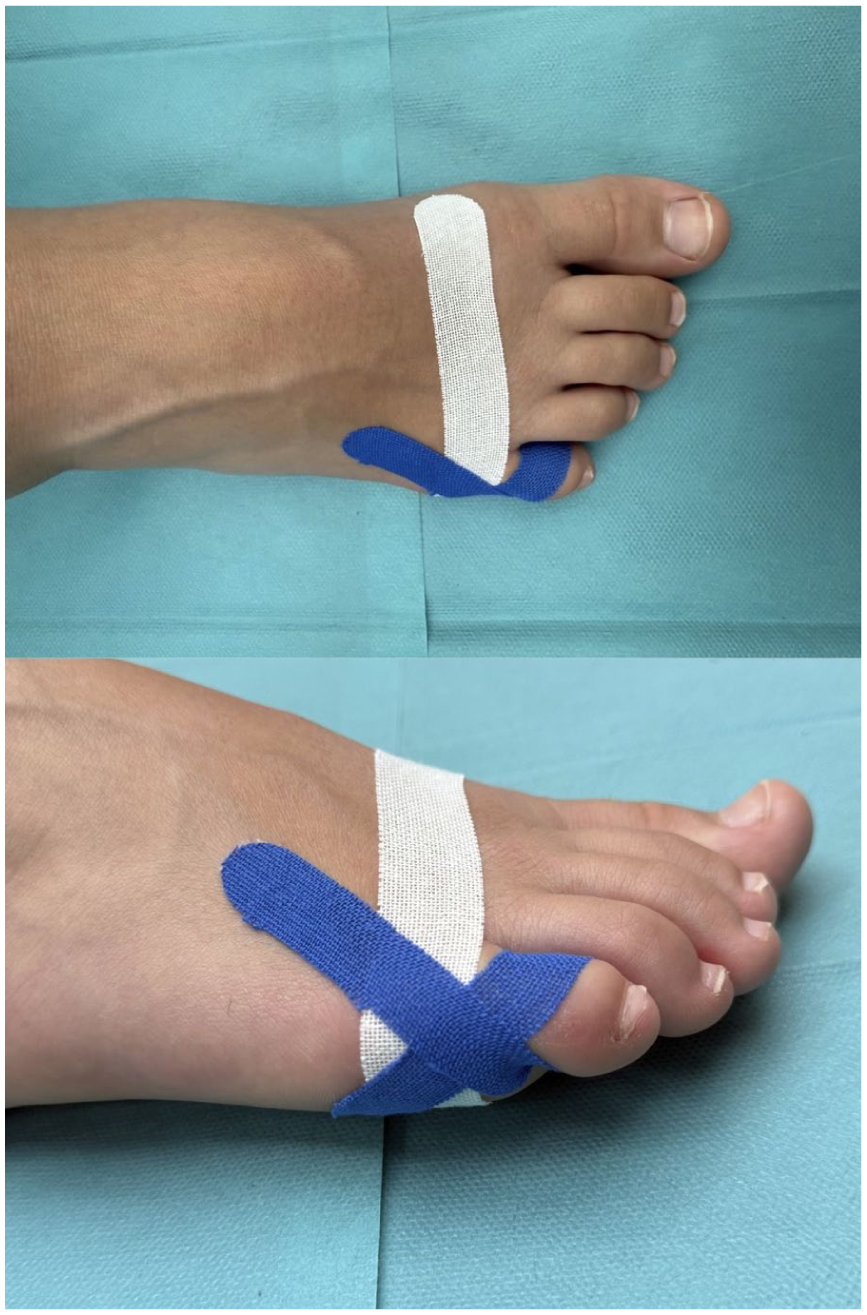
Because implants are usually not required for percutaneous correction of lesser toe deformities, temporary stabilization is achieved after the surgical procedure with external tapes and/or bandages. Taping techniques depend on deformity patterns and must be tailored to suit individual deformities. In general, tapes can be applied in a semicircumferential fashion (like a charity ribbon; Figure 5), in a crossing fashion (Figure 6), or longitudinally (Figure 7). In common claw toe deformities (MTPJ hyperextension with proximal [PIP) and distal interphalangeal [DIP] flexion), a ribbon-style tape is applied dorsally at the base of the proximal phalanx, crossing plantarly (Figure 5). Independent tensioning of the medial and lateral branches allows rotational adjustment. Slight plantarflexion overcorrection at the MTPJ is recommended to ensure maintained correction after tape removal.

With a charity-ribbon–style tape applied dorsally at the base of P1, the toe can be retained in slight plantarflexion. Rotational alignment can be adjusted by applying differential tension to the 2 reins. Dorsoplantar view (A) and plantar view (B).

The crossing tapes (blue) can control valgus/varus alignment in particular and also influence sagittal alignment (plantarflexion) and the coronal plane (rotation). Dorsoplantar view (A) and plantar view (B).

Additional longitudinal tapes (white) are recommended after selective Flexor digitorum brevis (FDB) tenotomy and/or dorsal closing P2 osteotomy, both intended to correct a flexion deformity in the proximal (PIP) and/or distal interphalangeal (DIP) joint.
A second, dorsal-crossing pair of tapes can further influence valgus/varus alignment while reinforcing plantar flexion (Figure 6). To stabilize the PIP and DIP joints, a short tape is applied distally around the toe tip, crossing from plantar to dorsal and preloaded over the distal joints (Figure 7). No tension should be applied when crossing the MTPJ to avoid dorsiflexion of the toe.
Although no uniform definition of a hammertoe deformity exists, it is commonly characterized by flexible or fixed hyperflexion of the proximal interphalangeal joint and by a flexion or extension deformity of the distal interphalangeal joint, with the tip of the toe remaining in contact with the ground. For a reproducible classification of lesser toe deformities, we recommend using the AFCP classification.12,13 In this type of deformity, a ribbon-style tape can be applied with its base on the plantar aspect of P2, with the branches crossing dorsally and proximally. An additional tape may be placed distally at the tip of the toe, crossing and stabilizing the DIP and PIP joints dorsally (Figure 7). The principles of 3-dimensional external stabilization and retention can likewise be applied to other types of lesser toe deformities, tailored to the specific deformity pattern present.
Taping of the Fifth Ray
Taping principles for the fifth ray, including bunionette correction and digitus quintus varus, are similar to those for the central lesser toes. Percutaneous bunionette correction can involve proximal, diaphyseal, or distal osteotomies, often without implants. 14 When necessary, extensor tendon tenotomy and medial MTPJ capsulotomy can be added to address deforming forces. Elastic tape is applied laterally in a U-shape around the fifth metatarsal head, pushing it medially to retain fragment displacement (Figure 8, white tape). If more retention is needed, additional overlapping tapes can be used. After a lateral closing base osteotomy of the proximal phalanx for digitus quintus varus, a ribbon-style tape centered medially on P1 is applied, crossing laterally and proximally to maintain alignment (Figure 8, blue tape). Overcorrection must be avoided to prevent valgus malalignment.
Correction of MT5 is maintained using 1 or 2 overlapping U-shaped tapes that stabilize and retain the distal osteotomy fragment medially (white tape). In cases of a lateral closing osteotomy at the base of P1, a charity-ribbon–style tape is applied, crossing on the lateral aspect of the fifth ray (blue tape).
Discussion
External fixation is considered indispensable in several percutaneous techniques, such as screwless Akin, lesser toe corrections, and bunionette deformities, despite limited evidence regarding the impact of postoperative taping on radiologic or clinical outcomes.9,11,14 Proper taping provides reliable 3-dimensional stabilization when internal fixation is omitted, supporting healing and correction retention. Whereas elastic taping can be widely purchased and easily applied, off-the-shelf orthotics or moldable splints often fail to provide continuous 3-dimensional retention, are not readily available in all settings, and are generally not considered suitable for retention and correction after percutaneous lesser toe correction. Elastic taping is a safe, cost-effective, and time-efficient external fixation method. It allows surgeons to fine-tune alignment and adapt to individual deformities. The use of precut elastic tapes allows the taping process to be standardized and accelerated, simplifying postoperative care while enhancing patient comfort and clinical efficiency. Patients can usually be instructed to reapply taping for the first ray themselves, whereas taping for lesser toes is more complex and typically performed by the attending physician or trained medical personnel. Before indicating the above-mentioned percutaneous surgeries without using internal fixation, surgeons must consider that repeated retaping visits can be time-consuming and may exceed the surgical time. The authors recommend exchanging the tapes on a 2-week basis for 6-8 weeks.
Conclusion
Ultimately, elastic taping as external fixation after percutaneous forefoot surgery is not merely an adjunct but a key component of the surgical strategy; when properly applied, it maintains correction and contributes to optimal functional outcomes in modern minimally invasive forefoot surgery.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261433593 – Supplemental material for Elastic Taping of the Toes after Percutaneous Forefoot Surgery: A Technical Tip
Supplemental material, sj-pdf-1-fao-10.1177_24730114261433593 for Elastic Taping of the Toes after Percutaneous Forefoot Surgery: A Technical Tip by Andreas Toepfer, Primoz Potocnik, Jan Farei-Campagna, Gabriel Ferraz Ferreira, Gustavo Araujo Nunes, Thomas L. Lewis, Peter Lam, Nasef Mohamed N. Abdelatif and Jorge Javier Del Vecchio in Foot & Ankle Orthopaedics
Footnotes
ORCID iDs
Ethical Considerations
Ethical approval was not required.
Consent to Participate
Not applicable.
Consent for Publication
Informed consent for publication was provided by the participant or a legally authorized representative.
Author Contributions
The authors A.T. and P.P. have contributed equally to the conception and preparation of the manuscript and share first authorship.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thomas L. Lewis, MBChB, BSc, MFSTEd, FRCS(Tr&Orth), reports general disclosures of PhD tuition fees supported by MIFAS, and consulting fees from Vilex. Disclosure forms for all authors are available online.
Supplemental Material
A supplemental video for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.