
Abstract
Background:
The impact of pronation and sesamoid coverage on clinical outcomes following percutaneous hallux valgus surgery are not currently known. The aim of this study was to investigate if sesamoid coverage was associated with worse clinical outcomes at 12-month follow-up following percutaneous hallux valgus surgery.
Methods:
Retrospective comparative observational study of clinical and radiographic outcomes based on a previously published prospective dataset. Patients were stratified into 3 cohorts based on the degree of sesamoid coverage (normal, mild, or moderate) on 12-month weightbearing radiographs following fourth-generation percutaneous hallux valgus surgery. Primary outcome was a validated patient-reported outcome measure (PROM), the Manchester-Oxford Foot Questionnaire (MOXFQ). Secondary outcomes included Euroqol-5D, VAS Pain, and radiographic deformity correction.
Results:
Forty-seven feet underwent primary fourth-generation HV surgery and were stratified into 3 cohorts. There were 19, 16, and 12 feet in the normal, mild, and moderate cohorts respectively. There was no significant difference in either pre- or postoperative foot function (all MOXFQ domains, P > .05) or health-related quality of life (EQ-5D Index or VAS, P > .05). The MOXFQ Index preoperatively was as follows: normal cohort, 56.1 ± 26.9; mild cohort, 54.1 ± 17.9; and severe cohort, 49.6 ± 23.8; and postoperatively was as follows: normal cohort, 15.6 ± 21.5; mild cohort, 11.4 ± 15.5; and severe cohort, 11.4 ± 13.6 (P = .737-.908). There was significantly worse hallux valgus angle (HVA) and intermetatarsal angle (IMA) between the cohorts (P < .01). Although HVA and IMA were corrected to normal parameters following surgery in all cohorts, there was a significantly worse postoperative HVA in the moderate sesamoid coverage (5.3 ± 3.9 vs 7.9 ± 5.3 vs 11.4 ± 3.7, P < .01); however, IMA was not significantly different (3.4 ± 2.2 vs 4.1 ± 2.7 vs 5.2 ± 2.9, P = .168).
Conclusion:
This study found that cases where the sesamoids were not reduced had a poorer correction and had worse preoperative deformity. Clinical outcomes and foot function following fourth-generation percutaneous hallux valgus surgery were not affected by sesamoid coverage at the 12-month follow-up. The long-term implications in the difference in radiographic deformity between the 3 cohorts are not known, and further work should explore the relationship of first ray pronation and sesamoid position, particularly with regard to recurrence.
Level of evidence:
Level III, retrospective comparative study of prospectively collected data.
Keywords
Introduction
The importance of first metatarsal pronation and sesamoid coverage in etiology and pathophysiology of hallux valgus deformity is increasingly being studied (Figure 1). There are theories that residual rotational deformity or sesamoid coverage may predispose to recurrence, and the advent of weightbearing computed tomography has enabled assessment of the rotational deformity and correction that can be achieved during hallux valgus surgery.4,13,14,19,20
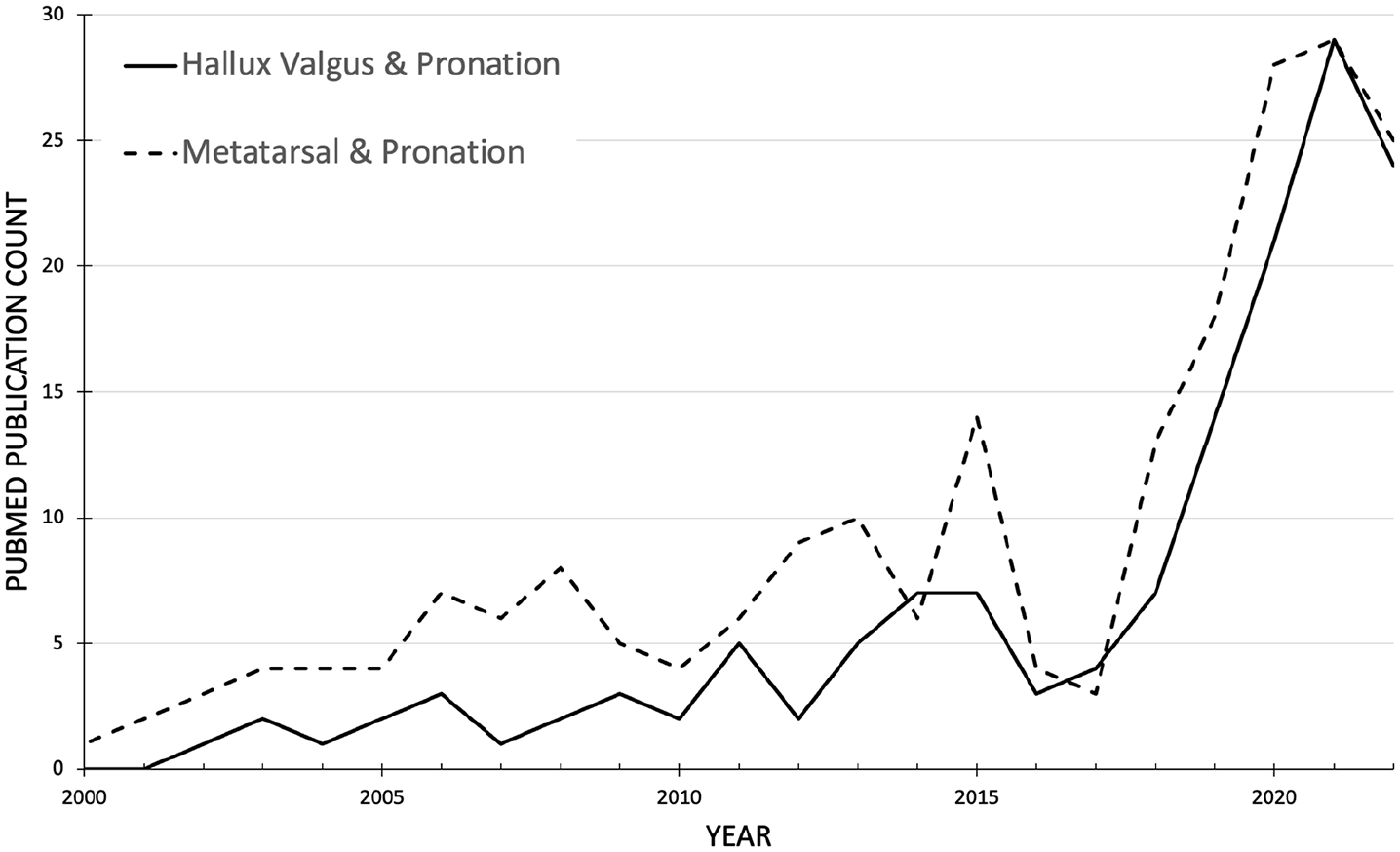
PubMed publication count by year for terms relating to hallux valgus, metatarsal, and pronation since 2000.
Fourth-generation percutaneous hallux valgus surgery potential facilitates correction of pronation and sesamoid coverage because of the unstable nature of the osteotomy allowing 3-dimensional and rotational deformity correction.5,6,10 There are, however, very few studies investigating the outcomes in patients with residual sesamoid uncoverage with either open or minimally invasive techniques.4,13
A number of studies have identified that first metatarsal pronation is an important factor in hallux valgus, particularly with regard to recurrence.12,14,15 First metatarsal pronation is linked to medial column anatomy as well as hindfoot alignment.8,19 Higher rates of recurrence have been linked to a round postoperative radiographic appearance of the metatarsal head, which is associated with improper correction of first metatarsal rotation and sesamoid reduction. 14 It is important to note there is no consensus yet as to the accuracy of measurement of this component of hallux valgus deformity and that metatarsal rotation and sesamoid coverage are distinct concepts.
The aim was to investigate if sesamoid coverage was associated with worse clinical outcomes at 12 months following percutaneous hallux valgus surgery.
Methods
This study presents subgroup analysis of a study previously published in Foot and Ankle International. 10 A detailed description of the methodology, participants, variables, and technique can be found in the original study. Lateral sesamoid position was categorized according to Agrawal et al 1 (Figures 2 and 3) and the primary outcome was a validated patient-reported outcome measure (PROM), the Manchester-Oxford Foot Questionnaire. Secondary outcomes include EuroQol-5D, visual analog scale for pain, and radiographic deformity correction.
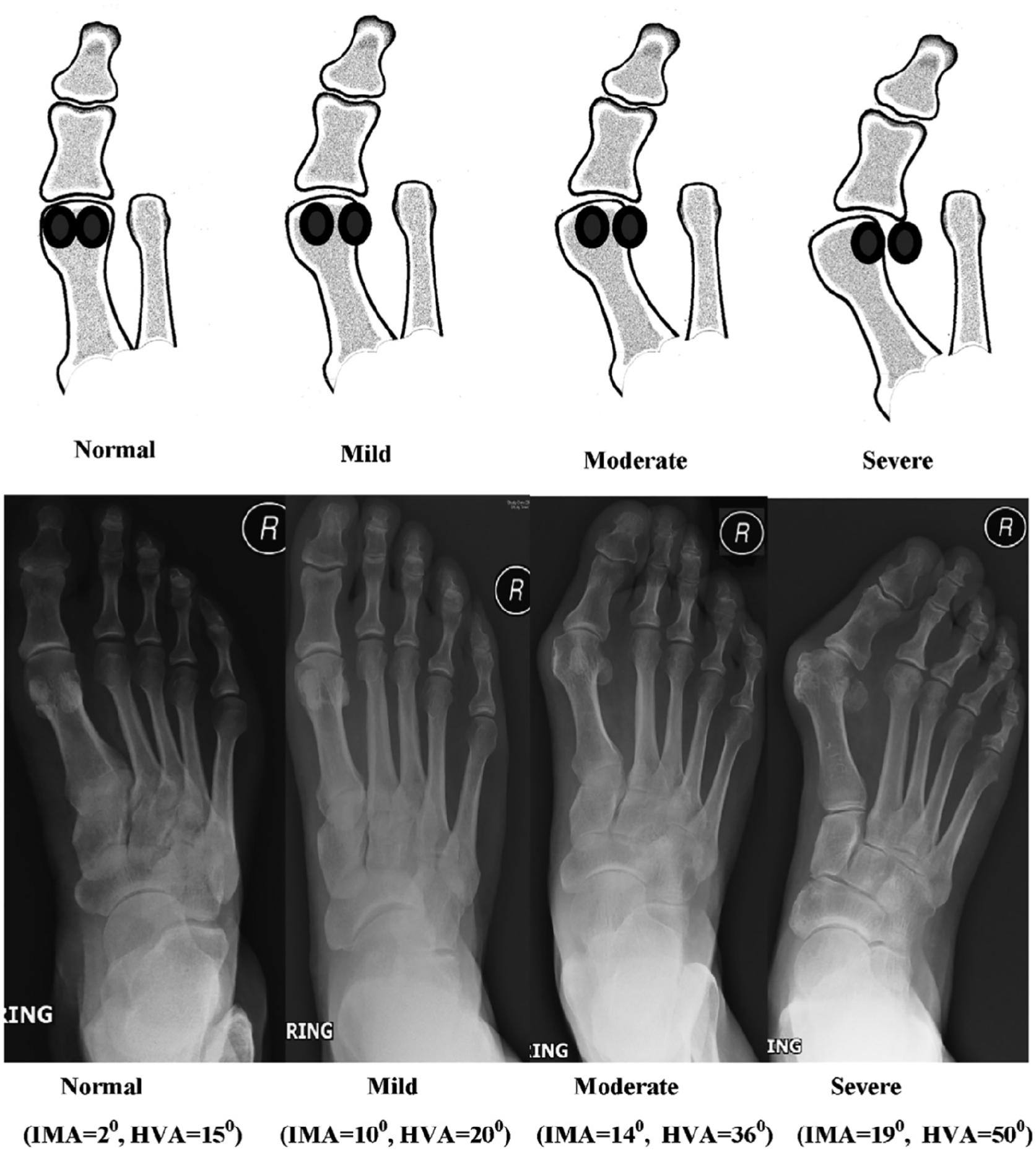
Sesamoid classification from Agrawal et al 1 (republished with permission).

Pre- and postoperative radiographs demonstrating (top) reduction to moderate sesamoid position following META and (bottom) complete sesamoid reduction following META surgery.
We sought to specifically explore whether sesamoid coverage had an impact on foot function following fourth-generation percutaneous hallux valgus surgery. This was chosen as 26% of the original cohort had residual sesamoid uncoverage following surgery.
Patients enrolled in this study were stratified into 3 cohorts based on the sesamoid coverage measured on 12-month weightbearing radiographs. Patients who had “moderate” sesamoid coverage were compared to patients with “normal” and “mild” sesamoid coverage. There were no patients in the original study who had “severe” sesamoid coverage in the postoperative radiographs.
Continuous outcomes for the 2 cohorts were compared using the paired and independent t test for parametric data and descriptive statistics used for categorical data. All analyses were performed with the Python SciPy package. A continuous outcome equivalence power analysis using independent data 11 following percutaneous hallux valgus surgery and with an alpha of 5% and a power of 80% estimated that a minimum sample size of 12 is needed in each group to be powered to detect a change in PROM.
Results
The original study recruited 50 feet with final radiographs available for 47 feet. These were divided into 3 cohorts based on the degree of sesamoid coverage on weightbearing radiographs as shown in Table 1.
Baseline Characteristics Between 3 Cohorts Based on Sesamoid Coverage on 12-Month Weightbearing Radiographs.

The primary pre- and postoperative clinical and radiographic outcomes between the 3 cohorts can be seen in Tables 1 and 2 demonstrating no significant difference in either foot-specific function, pain, or health-related quality of life. All cohorts had a statistically significant improvement in all MOXFQ domains from pre- to postoperative scores (P < .05).
Pre- and Postoperative Clinical and Radiographic Outcomes Following Fourth-Generation Percutaneous Hallux Valgus Surgery for 3 Cohorts Based on Sesamoid Coverage on Final Weightbearing Radiographs at 12 Months.

Abbreviations: HVA, hallux valgus angle; IMA, intermetatarsal angle; MOXFQ, Manchester-Oxford Foot Questionnaire; VAS, visual analog scale.
There was significantly worse preoperative deformity in terms of hallux valgus angle (HVA) and intermetatarsal angle (IMA) (P < .05, Table 2) in the moderate sesamoid coverage cohort. Although the mean HVA and IMA were corrected to normal parameters following surgery in all cohorts, there was a significantly worse postoperative HVA in the moderate sesamoid cohort (P < .05); however, IMA was not significantly different (P = .08). There was one episode of recurrence (defined as HVA > 15 degrees at final radiographic follow-up) within the study time frame that occurred in the uncovered sesamoid cohort. We noted that the uncovered sesamoid cohort was significantly older (P < .05) than the covered sesamoid cohort. There was variation in the assessment of the round sign (normal cohort: angular 100%; mild cohort: angular 77%, intermediate 23%; moderate cohort: angular 91%, intermediate 9%).
Discussion
This study found that postoperative sesamoid coverage did not impact on clinical foot function at 12 months following percutaneous surgery. This study also found greater HVA following surgery in the uncovered sesamoid cohort despite all radiographic assessments being within the normal range. There are current theories that failure to reduce the sesamoids and residual pronation of the first metatarsal may lead to increased recurrence rates, yet there are very limited studies reporting the clinical outcomes based on sesamoid coverage or residual pronation.2,4,13,14,20 Chen et al 2 found correcting the tibial sesamoid position to less than grade IV (using the Hardy and Clapham classification) led to poorer functional outcome and patient satisfaction 2 years following surgery in a large series of 250 patients.
Conti et al 4 reported the 2-year outcomes following the Lapidus procedure and found patients in the decreased first-metatarsal pronation group had statistically significantly greater improvement in the PROMIS physical function domain compared to the no change/increased first-metatarsal pronation group. This study was limited by loss to follow-up of 49% of cases. We were unable to find any studies reporting the relationship between clinical outcomes and sesamoid coverage/pronation in the context of percutaneous hallux valgus surgery. A series of 16 feet by Najefi et al 13 that investigated pronation 12 months following scarf osteotomy found poorer MOXFQ outcome scores in patients with higher postoperative pronation of the metatarsal, which is contradictory to our findings. Ferreira et al 5 evaluated the round sign post-percutaneous hallux valgus surgery in 45 feet and found the proportion of feet with mild or absent pronation increased from 29% to 55%; however, they did not evaluate if this had an impact on clinical PROMs. The relationship between the metatarso-sesamoid complex, sesamoid subluxation, and metatarsal pronation is not well understood. A number of studies utilizing weightbearing CT have observed variable relationships between metatarsosesamoid subluxation and M1 head pronation prior to surgical intervention.7,9,14,17,19 It is important to recognize that true subluxation of the sesamoids occurs when sesamoids leave their articular facets located inferior to the first metatarsal head, which can occur with or without pronation of the first metatarsal as demonstrated by Kim et al. 7 It is also important to consider the midfoot and hindfoot as an abnormal Meary angle, and hindfoot deformity have been shown to have a high likelihood of manifesting a proportionate degree of M1 rotation.8,15,18 There are a number of factors that may affect sesamoid reduction including the presence of preexisiting metatarsosesamoid osteoarthritis, intersesamoid crista underdevelopment or erosion, failure to perform a lateral release, and residual pronation deformity.3,15 We believe that failure to reduce the sesamoids at the time of surgery may lead to abnormal biomechanics of the first metatarsal and thus predispose to recurrence; however, this study did not have the length of follow-up to confirm this. Additionally, further clarity regarding the relationship of first-ray pronation and sesamoid position as measured on a weightbearing foot radiograph should be further explored.
There are important limitations of this short report, including the relatively small sample sizes and 12-month follow-up, which may not detect important outcomes such as recurrence or type 2 error. There are also baseline differences between the cohorts including age, and radiographic deformity which may lead to bias in the results and interpretation. There are multiple methods for assessing sesamoid position, and the classification we have used may not accurately represent metatarsal pronation.12,16 Finally, we only had radiographs and not formal weightbearing CT imaging so it was not possible to formally quantify the difference in metatarsal rotation between the 3 cohorts.
Conclusion
This study found cases where the sesamoids were not reduced had a poorer correction and had worse preoperative deformity. Clinical outcomes and foot function following fourth-generation percutaneous hallux valgus surgery were not affected by sesamoid coverage at 12-month follow-up. The long-term implications in the difference in radiographic deformity between the 3 cohorts are not known, and further work should explore the relationship of first-ray pronation and sesamoid position, particularly with regard to recurrence.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241230560 – Supplemental material for Impact of Sesamoid Coverage on Clinical Foot Function Following Fourth-Generation Percutaneous Hallux Valgus Surgery
Supplemental material, sj-pdf-1-fao-10.1177_24730114241230560 for Impact of Sesamoid Coverage on Clinical Foot Function Following Fourth-Generation Percutaneous Hallux Valgus Surgery by Thomas Lorchan Lewis, Gabriel Ferraz Ferreira, Gustavo Araujo Nunes, Peter Lam and Robbie Ray in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.