
Abstract
Background:
There has been increasing interest in the percutaneous dorsal closing-wedge Zadek calcaneal osteotomy (PDCWZO) for the treatment of insertional Achilles tendinopathy (IAT). This study aims to investigate the clinical efficacy and radiographic outcomes of the percutaneous dorsal closing-wedge Zadek calcaneal osteotomy in patients with and without pes cavus foot morphology.
Methods:
A multicentre observational study of patients undergoing PDCWZO for IAT. Patients were stratified into cavus (calcaneal pitch angle > 20 degrees) and non-cavus (calcaneal pitch angle ≤ 20 degrees) groups. The primary outcome was the X/Y ratio and calcaneal pitch angle. Clinical outcomes were assessed using the Manchester-Oxford Foot Questionnaire (MOXFQ), visual analogue scale (VAS) for pain, and EuroQol–5 dimensions (EQ-5D). Between-group analyses were performed to identify differences in outcomes based on foot morphology.
Results:
Between April 2022 and December 2024, 67 feet (61 patients; 25 male, 36 female) with mean age 55.0 ± 12.7 years (range: 20.9-77.6) underwent percutaneous Zadek osteotomy with a median clinical follow-up of 0.56 years (IQR: 0.48-0.99) and median radiographic follow-up of 0.36 years (IQR: 0.13-0.49). The cohort included 50 cavus feet and 17 non-cavus feet. Radiographic analysis showed a significant increase in the X/Y ratio in both groups (cavus: 2.44 ± 0.27 to 3.08 ± 0.45, P < .001; non-cavus: 2.43 ± 0.28 to 3.05 ± 0.56, P < .001). Calcaneal pitch angle remained unchanged in both the cavus group (27.1 ± 4.2 degrees to 27.1 ± 4.6 degrees, P = .917) and non-cavus group (17.7 ± 1.7 degrees to 18.8 ± 4.8 degrees, P = .270). Clinical outcomes in all groups demonstrated significant improvement in all MOXFQ domains, VAS Pain and EQ-5D (P < .05). The complication rate was 6.0%.
Conclusion:
At short-term follow-up (median 6.7 months), percutaneous Zadek calcaneal osteotomy demonstrated a low complication rate and was associated with improvements in foot function and pain relief for patients with both cavus and non-cavus feet.
Level of Evidence:
Level III, retrospective comparative study.
Keywords
Introduction
Background/rationale
Insertional Achilles tendinopathy (IAT) is a chronic degenerative condition characterized by pain, swelling, and limited function, particularly during weight-bearing or exercise activities.1,2 Non-operative treatment approaches include physical therapy, orthotics, shockwave therapy, and anti-inflammatory medications.3,4 However, surgical intervention is considered when conservative measures fail, with procedures ranging from open debridement and tendon repair to calcaneal osteotomies, aimed at altering tendon tension and improving biomechanics.1,5 -7
Recent advances in minimally invasive surgery techniques offer the potential for reducing soft tissue disruption, minimizing post-operative complications, and promoting quicker recovery.8,9 One such technique, the percutaneous dorsal closing-wedge or Zadek calcaneal osteotomy (ZO; Figure 1), aims to offload the Achilles tendon to anteriorize the calcaneal tuber, thereby decompressing the Achilles tendon and thus altering hindfoot biomechanics leading to pain relief and improved function, while preserving the integrity of surrounding structures.1,10 -15 However, there is limited literature on the outcomes of this procedure for the treatment of IAT, many of which are single-center or surgeon studies with methodologic limitations such as small sample sizes and risk of bias.6,13,16,17

Pre- and post-operative weight-bearing radiographs demonstrating the percutaneous dorsal closing-wedge calcaneal osteotomy.
Foot morphology, particularly the presence of pes cavus, may influence the biomechanical stress at the Achilles insertion and potentially affect surgical outcomes following ZO. Alterations in foot morphology significantly influence lower limb kinematic patterns and force distribution during gait. The elevated calcaneal pitch in cavus feet modifies the ankle-foot complex mechanics, potentially increasing tensile stress at the Achilles insertion through altered lever arm dynamics and ground reaction force vectors.18,19 These biomechanical alterations may have implications for surgical outcomes following calcaneal osteotomy, although this relationship remains incompletely characterized in the literature. Despite the theoretical importance of foot architecture in IAT pathology and treatment outcomes, there is a paucity of research examining the efficacy of ZO specifically in relation to different foot morphologies.
Aims
This study aims to investigate the clinical efficacy and radiographic outcomes of the percutaneous dorsal closing-wedge Zadek calcaneal osteotomy in patients with and without pes cavus foot morphology.
Methods
Study Design and Setting
An observational multicenter case series of consecutive patients performed by 4 surgeons across different institutions. This study was reported in line with the STROBE guidelines for observational studies. 20
Participants
Consecutive patients aged 18 years and older who had exhausted conservative treatment and subsequently underwent primary dorsal closing-wedge Zadek osteotomy for the treatment of insertional Achilles tendinopathy were included. Patients who had previously had surgery for IAT were excluded.
Group Allocation
Patients were stratified into 2 groups based on their pre-operative calcaneal pitch angle (PAR): cavus foot (PAR > 20 degrees) and non-cavus foot (PAR ≤ 20 degrees). This classification was determined from standardized weight-bearing lateral radiographs, with the pitch angle measured as the angle between the horizontal axis and a line drawn along the plantar aspect of the calcaneus.
Variables
The primary outcome was change in radiographic parameters following surgery, compared between cavus and non-cavus groups. Radiographic deformity parameters included the X/Y ratio and calcaneal pitch angle as per Tourné et al. 13 Secondary outcomes included clinical function and complication profile. Clinical outcomes were assessed using the Manchester-Oxford Foot Questionnaire (MOXFQ), visual analogue scale for pain (VAS Pain), and EuroQol–5 dimensions (EQ-5D). Complications were graded using a modified Clavien-Dindo classification. 21
Data Sources and Measurement
All patients underwent pre-operative and minimum-6-week weight-bearing radiographs. Radiographic measurements were performed by one trained observer at each contributing centre using standardised anatomical landmarks as defined by Tourne et al. PROMs were collected at regular time points following surgery. Missing PROM data were handled using complete case analysis. PROMs were only collected by 2 of the 4 contributing surgeons as part of their routine clinical practice, resulting in systematic rather than random missing data patterns.
Bias
We attempted to reduce bias by including all patients who underwent Zadek osteotomy and recruited patients from a number of centres. All outcome data were analysed independently of the operating surgeons who were blinded to these clinical outcomes.
Sample Size
We included all consecutive eligible cases without a priori sample size calculation.
Statistical Methods
Between-group comparisons for continuous variables were performed using independent t tests for normally distributed data and Mann-Whitney U tests for non-normally distributed data. Within-group comparisons (pre- vs post-operative) used paired t tests for parametric data and Wilcoxon signed rank tests for non-parametric data. The Shapiro-Wilk test was used to assess data normality. Given the small sample and significant baseline differences in follow-up duration, these comparisons are presented for descriptive purposes only. In addition, 95% CIs were calculated. All analyses were performed with Python SciPy package. 22 Statistical significance was defined as P < .05.
Operative Technique
All patients included in this study underwent a percutaneous dorsal closing-wedge Zadek osteotomy (Figure 2). Each surgeon performed the operation according to the following principles. The operation is performed with the patient in the lateral position, using a bolster to ensure that the hindfoot is parallel to the floor. A tourniquet is applied, along with tranexamic acid and intravenous antibiotics. The osteotomy site, typically 1-2 cm posterior to the subtalar joint line, is marked, with fluoroscopy used to confirm the optimal placement of the dorsal closing-wedge apex. A small, 3- to 4-mm incision is made on the lateral aspect of the heel, posterior to the peroneal tendons and above the sural nerve. The soft tissues are bluntly dissected down to the bone, and an elevator is used to free the tissues over the osteotomy site.

A series of intra-operative images demonstrating the steps of the operation. From top left: Initial marking of the osteotomy, entrance at the inferiormost aspect of the osteotomy to prevent plantar fracture, initial calcaneal osteotomy subsequently widened with larger diameter burr, osteotomy closure by placing foot in dorsiflexion and fixation with 2 screws.
Guidewires are inserted under fluoroscopic guidance at the desired angle for the osteotomy, creating space for the dorsal closing wedge. A 3.0 × 30.0-mm low-speed, high-torque Shannon burr (or in some cases, increasing burr diameter as shown in Figure 2) is then used to perform the calcaneal osteotomy along the guidewires. Care is taken to preserve the plantar cortex as fracture here can lead to loss of position (Figure 3). Multiple bone passes are needed to remove enough bone, aiming for approximately 1 cm width at the dorsal aspect of the wedge. Fluoroscopy confirms the completion of the osteotomy, and irrigation is performed to remove bone debris.

Radiographs demonstrating failure of the plantar hinge leading to failure and loss of position. Case supplied with permission from Dr Andreas Toepfer.
To mobilize the calcaneus and close the dorsal closing-wedge osteotomy, the foot is dorsiflexed, with the tension of the Achilles tendon assisting in the closure. Fluoroscopy confirms the appropriate closure of the osteotomy. Once the desired position is achieved, 2 K-wires are temporarily inserted across the osteotomy for stabilization. Using fluoroscopy, 2 cannulated screws (diameter 6.5-8 mm depending on surgeon preference) are inserted from posterior to anterior, below the Achilles tendon insertion, with screw placement and alignment confirmed through lateral and axial fluoroscopy. Patients were restricted to non-weight-bearing in a backslab for 2 weeks followed by full weight-bearing in a boot from week 2-6 post surgery. Physiotherapy commenced at 6 weeks focusing on regaining range of motion and strength.
Ethical Approval and Funding
This study was conducted in line with the declaration of Helsinki. Local institutional review board approval was gained. Informed consent was obtained from all participants. There was no funding to support this study. P.L., T.L., G.F., R.R., and T.G. report fees from industry beyond the scope of this study. None of the authors have any financial conflicts of interest to declare.
Results
Participants
Between April 2022 and December 2024, a total of 61 patients (67 feet) underwent percutaneous dorsal closing-wedge Zadek calcaneal osteotomy. The mean age was 55.0 ± 12.7 years (range: 20.9-77.6 years). The cohort comprised 25 males (41.0%) and 36 females (59.0%). Based on pre-operative calcaneal pitch angle, 50 feet (74.6%) were classified as cavus (PAR > 20 degrees) and 17 feet (25.4%) as non-cavus (PAR ≤ 20 degrees). The median clinical follow-up was 0.56 years (IQR: 0.48-0.99), with significantly longer follow-up in the cavus group compared with the non-cavus group (0.77 years [IQR: 0.50-1.05] vs 0.49 years [IQR: 0.44-0.61], P = .025). The median radiographic follow-up was 0.36 years (IQR: 0.13-0.49), with significantly longer follow-up in the cavus group (0.45 years [IQR: 0.14-0.53]) compared with the non-cavus group (0.23 years [IQR: 0.12-0.28]), P = .017.
The cavus and non-cavus groups were comparable in terms of age (P = .442) and gender distribution (P = .695). Demographic characteristics are summarised in Table 1. Radiographic data were available for all cases, with PROMs available for 61.2% of cases (only 2 of the 4 contributing surgeons routinely collect PROMs as part of their standard clinical practice (the percentage completion rate for surgeons who collect PROMS was 77.3%).
Demographic Characteristics of the Study Population.

Primary Outcome
In the overall cohort, there was a significant increase in the X/Y ratio from 2.44 ± 0.27 pre-operatively to 3.07 ± 0.47 post-operatively (mean change: 0.63, 95% CI: 0.54-0.74, P < .001) as shown in Table 2. When stratified by foot type, both groups showed a significant increase in X/Y ratio (cavus: 2.44 ± 0.27 to 3.08 ± 0.45, P < .001; non-cavus: 2.43 ± 0.28 to 3.05 ± 0.56, P < .001), with no significant between-group difference in the magnitude of radiographic correction (P = .75, Cohen d = 0.05). This geometric correction across foot morphologies was associated with clinically meaningful improvements in patient-reported outcomes, with 70.7% of patients (29/41) achieving the minimal clinically important difference (MCID) threshold for MOXFQ Index. The proportion of patients exceeding MCID thresholds was equivalent (not statistically significant) between the cavus and non-cavus groups (MOXFQ Index: 67.7% vs 80.0%, P = .733), demonstrating that the radiographic correction translated to comparable clinical benefit regardless of baseline foot anatomy.
Radiographic Parameters Pre- and Post-operatively Following Percutaneous Zadek Osteotomy.

The mean pre-operative calcaneal pitch angle was significantly higher in the cavus group (27.1 ± 4.2 degrees) compared with the non-cavus group (17.7 ± 1.7 degrees), as expected by definition (P < .001). Post-operatively, there was no significant change in pitch angle in the cavus group (27.1 ± 4.2 degrees to 27.1 ± 4.6 degrees, P = .917), whereas the non-cavus group showed a non-significant increase (17.7 ± 1.7 degrees to 18.8 ± 4.8 degrees, P = .270).
Correlation analysis revealed no significant association between the magnitude of radiographic correction (change in X/Y ratio) and clinical improvement for most PROMs (MOXFQ Index: r = −0.18, P = .265; MOXFQ Pain: r = −0.28, P = .075; MOXFQ Walking: r = −0.09, P = .581; MOXFQ Social: r = −0.16, P = .308; VAS Pain: r = −0.02, P = .872; EQ-5D Index: r = 0.12, P = .422). EQ-5D VAS showed a weak positive correlation (r = 0.37, P = .012), although this was not observed with other outcome measures.
Secondary Outcomes
Clinical outcome measures showed significant improvements in the overall cohort and cavus group as shown in Table 3. In the overall cohort, there were statistically significant improvements in all MOXFQ domains, VAS Pain scores, and EQ-5D measures (P < .05 for all). The cavus group (n = 31) demonstrated consistent significant improvements across all outcome measures. The non-cavus group showed improvement trends but did not reach statistical significance, likely because of the limited sample size (n = 10). Comparison of baseline characteristics between patients with and without complete PROM data found significant differences in age (51.8 ± 12.1 vs 60.2 ± 13.0 years, P = .012) and sex distribution (53.7% vs 15.0% male, P = .009). However, there were no significant differences in foot type (P = .583), baseline calcaneal pitch angle (24.3 ± 5.3 degrees vs 25.6 ± 6.2 degrees, P = .383), or baseline X/Y ratio (2.43 ± 0.27 vs 2.46 ± 0.26, P = .688), suggesting that radiographic disease characteristics were similar between groups despite demographic differences.
Pre- and Post-operative Clinical Patient-Reported Outcome Measures.
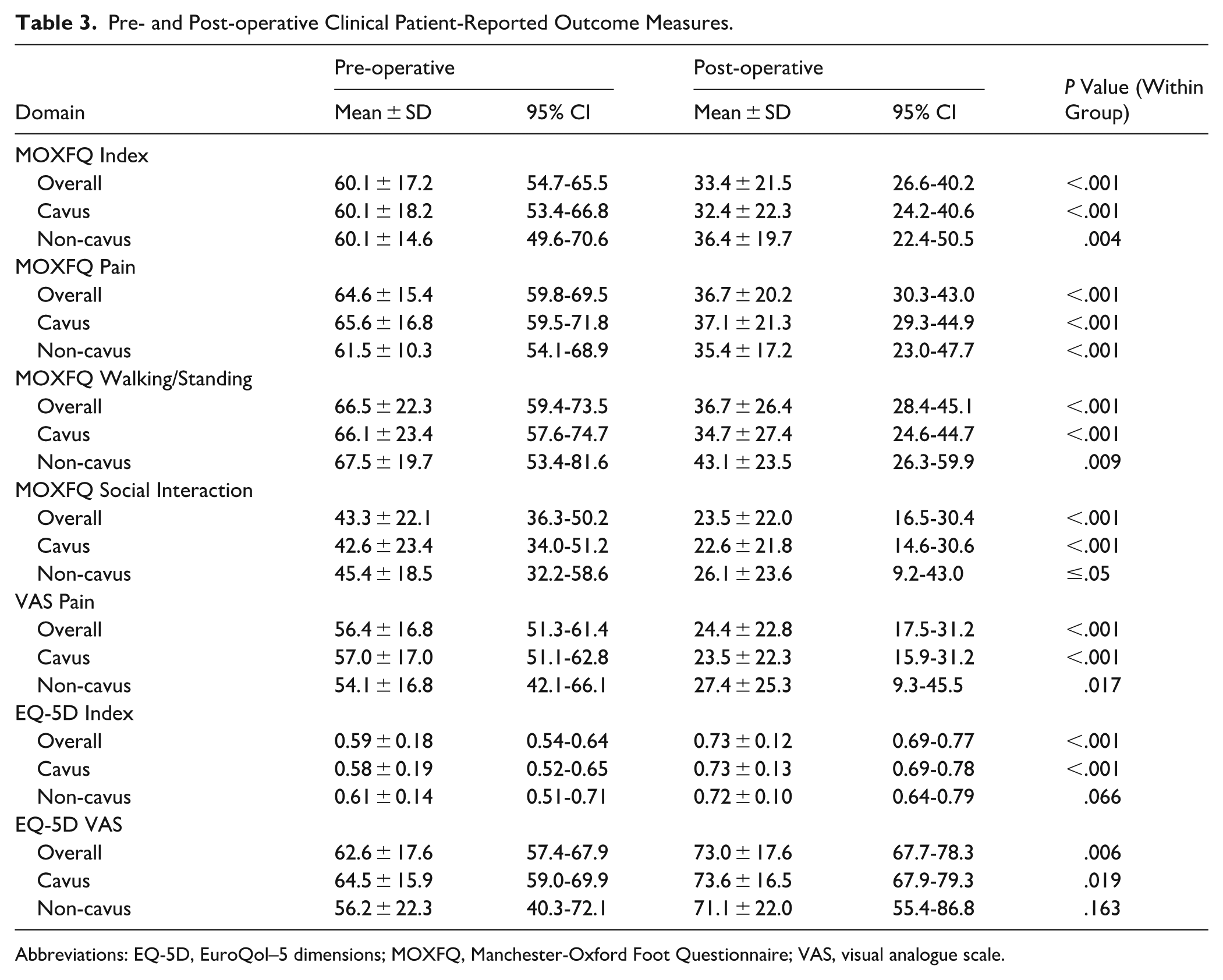
Abbreviations: EQ-5D, EuroQol–5 dimensions; MOXFQ, Manchester-Oxford Foot Questionnaire; VAS, visual analogue scale.
When comparing the magnitude of clinical improvement between cavus and non-cavus groups using between-group analysis, no statistically significant differences were observed in radiographic parameter or clinical PROMs (P = .309-.864), suggesting that foot type did not significantly influence the outcomes of the procedure. Between-group comparisons should be interpreted with caution because of the small non-cavus sample size (n = 17) and significantly longer follow-up in the cavus group (0.77 years [IQR: 0.50-1.05] vs 0.49 years [IQR: 0.44-0.61], P = .025). Both groups demonstrated significant improvement trends in clinical outcomes when considering within-group changes (P < .05, Table 3).
The majority of patients achieved clinically meaningful improvement as defined by established MCID thresholds. For MOXFQ Index, 29 of 41 patients (70.7%) achieved the MCID threshold of 12 points. Similarly, high proportions of patients exceeded MCID thresholds for other patient-reported outcomes: MOXFQ Pain (78.0%, 32/41), MOXFQ Walking (70.7%, 29/41), MOXFQ Social Interaction (73.2%, 30/41), and VAS Pain (75.6%, 34/45). The EQ-5D Index demonstrated a more moderate proportion of responders at 51.1% (23/45) using the MCID threshold of 0.08. Comparison between cavus and non-cavus groups revealed no statistically significant differences in the proportion of patients achieving MCID thresholds for any outcome measure (MOXFQ Index: 67.7% vs 80.0%, P = .733; VAS Pain: 77.1% vs 70.0%, P = .963; EQ-5D Index: 48.6% vs 60.0%, P = .780). These findings demonstrate that the percutaneous Zadek osteotomy produces clinically meaningful improvements in the majority of patients, with equivalent clinical benefit regardless of foot morphology.
Complications
The overall complication rate was 6.0%. There was 1 grade 2B complication of recalcitrant plantar fasciitis, 1 grade 3A case of prominent screws requiring removal, and 2 grade 3B cases requiring revision surgery—one where symptoms failed to completely resolve and a second that had non-union.
Discussion
Key Results
This multi-centre study has found that percutaneous dorsal closing-wedge Zadek calcaneal osteotomy is associated with a favorable safety profile and significant improvement in clinical foot function in both cavus and non-cavus foot types. However, we did not find a statistically significant change in the calcaneal pitch, which is in contrast to expected findings and the results of other studies. We believe that anteriorization of the tuberosity (reflected by X/Y ratio change) is the primary therapeutic mechanism, rather than pitch angle reduction for clinical improvement. The Zadek dorsal closing-wedge osteotomy moves the posterior prominence anteriorly without necessarily rotating the entire calcaneus facilitating offloading of the Achilles tendon. The absence of consistent correlation between radiographic correction and clinical outcomes suggests that the therapeutic benefit may result from multiple mechanisms beyond geometric correction alone, including retrocalcaneal decompression and altered tendon biomechanics rather than a simple dose-response relationship between bone resection and clinical improvement. Tourné et al 13 found a significant increase in X/Y ratio after surgery (similar to us) and a significant reduction in calcaneal pitch angle from 28.95 to 19.77 which is a much larger change than we found. This contrasts with studies by Ge et al 23 and López-Capdevila et al 24 that reported no change in pitch angle in cavus feet following calcaneal closing-wedge osteotomy. This could be related to the size of the osteotomy given this group utilised an open approach that may have facilitated removal of a larger wedge. 17 A biomechanical cadaveric study also found a significant increase in X/Y ratio and corresponding reduction in retrocalcaneal pressure as well as shifting the Achilles tendon insertion proximally. 14 This consistent increase in X/Y ratio irrespective of foot type suggests that the primary geometric effect of the Zadek osteotomy, shortening the calcaneal tuberosity relative to its overall length, is achieved reliably across different foot morphologies. Although formal inter-rater reliability assessment was not performed for this multi-centre study, the use of standardised measurement techniques based on validated anatomical landmarks and the consistency of findings across centres (with all centres demonstrating significant improvements in X/Y ratio) supports the validity and reproducibility of our radiographic outcomes.
There are increasing studies investigating the clinical outcomes of the percutaneous dorsal closing-wedge calcaneal Zadek osteotomy leads to positive clinical outcomes and improvements in foot function, and reduced pain as shown in Table 4.6,16,25,26 Systematic reviews with meta-analyses have shown statistically significant improvements in AOFAS scores and pain levels after dorsal closing-wedge calcaneal Zadek osteotomy although a number of these pre-date the introduction of modern minimally invasive techniques using a high-torque, low-speed burr to perform the osteotomy, which we believe is important. 12
Studies Reporting the Clinical Outcomes of Percutaneous Dorsal Closing-Wedge Calcaneal Osteotomy.

There are limited comparative studies investigating open vs percutaneous approaches to IAT. A systematic review by Bakaes et al 12 compared open and percutaneous Zadek osteotomy for treating insertional Achilles tendinopathy. This review, covering 17 studies and 625 procedures, found that although both techniques improved patient outcomes, percutaneous ZO was associated with significantly fewer complications. Hall et al 7 also explored this comparison in a contemporary review and noted that while traditional open procedures for Haglund deformity (often associated with insertional Achilles tendinopathy) generally produce good outcomes, the extended recovery time and potential complications led to increased interest in minimally invasive techniques. Although not directly comparable to percutaneous techniques, Yuen et al 27 found a reduction in post-operative complications (from 12.3% to 5.3%) when employing an endoscopic approach for Haglund deformity compared with open surgery. Choi and Suh 28 directly compared a modified percutaneous ZO to open Haglund resection in 25 cases and found that the modified percutaneous ZO led to faster clinical improvement than open Haglund resection, although both groups experienced significant improvement in pain and function. Hall et al also compared open Haglund resection vs percutaneous ZO and found both the open midline Achilles tendon splitting Haglund resection and percutaneous ZO led to significant improvement in patient-reported outcomes. However, their study demonstrated a statistically significant lower minor wound complication rate in the percutaneous ZO group. Hall et al 7 (in a separate study) reviewed outcomes after Zadek osteotomy and observed that early studies, although demonstrating positive results, often employed a large lateral incision, increasing the risk of complications. Nordio et al16,29 found that percutaneous ZO led to significant improvement in pain scores, improved function, and shorter recovery times. The growing evidence for minimally invasive techniques in foot and ankle surgery have documented superior outcomes with minimally invasive techniques across various pathologies, particularly regarding complication rates, recovery time, and short-term outcomes.30 -33 The percutaneous Zadek osteotomy offers the theoretical advantages of reduced soft tissue trauma, preserved vascularity, and expedited rehabilitation while potentially maintaining surgical effectiveness. However, the technical demands and learning curve associated with percutaneous techniques warrant consideration, as surgical proficiency significantly influences outcomes. 34
Although promising, the existing literature primarily comprises Level IV retrospective case series, highlighting the need for higher-level evidence, particularly randomised controlled trials. Future research should focus on long-term outcomes, comparisons with other surgical techniques (such as open debridement), and the identification of ideal candidates for ZO based on clinical, radiographic, and advanced imaging studies.
Despite its effectiveness, ZO is associated with potential complications, although these are generally considered minor.10,12 The reported complication rate for percutaneous ZO is around 5.8%, significantly lower than the 10.2% reported for the open approach. 12 This difference is likely attributable to the minimally invasive nature of the percutaneous technique, which minimises soft tissue disruption and the risk of wound-related issues. The most frequently reported complications include symptomatic hardware and sural nerve paresthesia.10 -12,29,35 Violation of the plantar hinge during surgery is a significant risk factor for nonunion. 35 Careful surgical technique, particularly in preserving the plantar hinge during percutaneous ZO, is crucial to mitigate these risks.
The Zadek osteotomy is believed to relieve pain in IAT through a combination of biomechanical and biological mechanisms. Biomechanical studies on percutaneous ZO are limited but provide insights into its mechanism of action.13,15 Studies suggest that ZO alters calcaneal morphology, increasing calcaneal tuberosity height, reducing calcaneal inclination, and anteriorly tilting the heel prominence, which may reduce strain on the degenerated inflamed Achilles tendon as well as decrease pressure on the retrocalcaneal bursa, thereby alleviating pain and improving function. The change in calcaneal shape alters the lever arm of the Achilles tendon, potentially reducing strain during ankle motion. Clinical studies suggest that it is not necessary to remove the prominent posterior heel spur.6,16 The reduction in Achilles tendon strain at the insertion may decrease inflammatory mediators and allow tissue remodeling. Recent evidence suggests that chronic tendon pathology involves complex interactions between mechanical loading, cellular responses, and extracellular matrix degradation. The biomechanical offloading achieved through calcaneal osteotomy may modulate these pathophysiological processes, although the specific cellular and molecular mechanisms remain to be fully understood. 36
The presence of Haglund deformity was not systematically documented across the cohort. Although this condition commonly coexists with insertional Achilles tendinopathy and may influence treatment outcomes, the geometric changes achieved by Zadek osteotomy (increased X/Y ratio and posterior tuberosity shortening) would theoretically address both pathologies through retrocalcaneal decompression and reduction of the posterosuperior heel prominence. Future prospective studies should systematically document Haglund deformity to enable specific analysis of its influence on surgical outcomes and to identify whether patients with or without this anatomical variant respond differently to the procedure.
Strengths
The strengths of this study are the use of validated clinical and radiographic outcome measures including the MOXFQ, as well as minimal loss to follow-up of the included patients. The multi-centre nature of this study increases the validity and generalisability of this procedure and the results.
Limitations
This study has several limitations that may impact the generalisability and interpretation of its findings. The sample size is relatively small, particularly for the non-cavus group (n = 17), which may not adequately represent the broader population affected by insertional Achilles tendinopathy and likely contributed to the lack of statistical significance in clinical outcomes for this subgroup. The imbalance in group sizes (50 cavus vs 17 non-cavus feet) and follow-up duration limits comparison between foot types and conclusions about differential treatment effects. The follow-up period was relatively short, with median clinical follow-up of 0.56 years and radiographic follow-up of 0.36 years. Although adequate for assessing early radiographic consolidation and initial functional recovery, this duration is insufficient to evaluate long-term durability of clinical improvements, late complications, or definitive treatment success. We did not systematically assess for the presence or severity of Haglund deformity in our cohort, which limits our ability to determine whether this procedure’s effectiveness varies based on the presence of concurrent Haglund deformity. The study’s observational design, which lacked comparisons to open surgery, although suitable for evaluating associations, does not establish causation, and the lack of a control group makes it challenging to compare the effectiveness of the percutaneous Zadek osteotomy against other treatment modalities. As an observational case series, this study is inherently susceptible to various biases including selection bias, measurement bias, and confounding by indication. The absence of a control group prevents direct comparison with alternative treatments or natural history. Furthermore, the retrospective nature limits data completeness and introduces potential information bias and selection bias, particularly given the significant age and sex differences observed between patients with and without complete PROM data. Although we attempted to minimize these limitations through standardized measurement protocols and validated outcome instruments, residual confounding likely influences our findings. Furthermore, the reliance on patient-reported outcome measures introduces the possibility of response bias, as patients may overestimate or underestimate their symptoms and functional improvements. The presence of complete PROM data was associated with younger age and male sex, which may introduce selection bias. However, the similarity in baseline radiographic parameters between groups suggests that disease severity was comparable, and the systematic rather than random nature of missing data (related to which surgeon performed the procedure) reduces the likelihood of outcome-dependent missing data. The limited PROM data availability because of differing clinical practice protocols between centres restricts the generalisability of the clinical outcome findings, although the available data provide valuable preliminary evidence of functional improvement. Post hoc power analysis for the primary outcome (X/Y ratio change) with the observed effect size of 0.63 and sample size of 67 demonstrated power exceeding 0.99 for detecting the within-group change. However, for between-group comparisons (cavus vs non-cavus), the study was underpowered to detect small-to-moderate effect sizes (Cohen d = 0.05), which should be considered when interpreting comparative findings, and conclusions regarding equivalence between foot types should be regarded as preliminary.
These limitations suggest that although the findings are promising, they should be interpreted with caution, and future prospective studies with larger samples, longer follow-up, and ideally randomized controlled designs are essential to establish definitive treatment efficacy and identify optimal patient selection criteria and validate these results.
Conclusion
Percutaneous dorsal closing-wedge Zadek calcaneal osteotomy was associated with a relatively low complication rate and initial patient-reported improvement in foot function across multiple surgeons and centers. The retrospective design and short follow-up period limit causal inference and do not allow assessment of long-term durability.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261427474 – Supplemental material for Short-term Outcomes of Percutaneous Zadek Osteotomy for Insertional Achilles Tendinopathy in Cavus vs Non-Cavus Feet: A Comparative Multi-Center Study
Supplemental material, sj-pdf-1-fao-10.1177_24730114261427474 for Short-term Outcomes of Percutaneous Zadek Osteotomy for Insertional Achilles Tendinopathy in Cavus vs Non-Cavus Feet: A Comparative Multi-Center Study by Thomas L. Lewis, Lily Fletcher, Clare Watt, Robbie Ray, Togay Koç, Ayla Claire Newton, Gabriel Ferraz Ferreira, Tyler A. Gonzalez and Peter Lam in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
We would like to thank Dr Andreas Toepfer for kindly sharing a case demonstrating plantar hinge fracture.
ORCID iDs
Ethical Considerations
This study was conducted in line with the declaration of Helsinki. Local institutional review board approval was gained.
Consent to Participate
Informed consent was obtained from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thomas L. Lewis, MBChB, BSc, FRCS(Tr&Orth), MFSTEd, PhD, reports royalties and consulting fees from Vilex beyond the scope of this study and PhD tuition fees supported by MIFAS. Robbie Ray, MBChB, ChM(T&O), FRCSed(Tr&Orth), FEBOT, reports consulting fees from Enovis/Novastep, Marquardt UK, Medartis, and Arthrex UK. Togay Koç, MBBS, MSc, FRCS (Tr & Orth), reports teaching for Arthrex Ltd. Gabriel Ferraz Ferreira, MD, MSc, PhD, reports consulting from Arthrex and Techimport. Tyler A. Gonzalez, MD, MBA, reports royalties and consulting fees from Vilex. Peter Lam, MBBS, FRACS, reports consulting fees from Enovis/Novastep, and Paragon 28; as well as AOFAS Ken Johnson Lecture 2024. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.