
Abstract
Background:
The percutaneous dorsal closing wedge calcaneal Zadek osteotomy (ZO) is an effective treatment for patients with insertional Achilles tendinopathy (IAT), although consensus is lacking on ideal patient selection. Tourné et al proposed that a preoperative calcaneal X/Y ratio <2.5 defines surgical candidacy, but this criterion remains controversial. This study evaluated whether patients with IAT benefit from percutaneous ZO regardless of preoperative X/Y ratio.
Methods:
A retrospective comparative study of 27 patients undergoing percutaneous ZO was performed. Patients were stratified into 2 cohorts based on preoperative X/Y ratio (<2.5 vs ≥2.5). Primary outcomes were PROMIS scores for pain, function, and mobility at 3, 6, and 12 months. Secondary outcomes included complication rates and radiographic parameters. Minimal clinically important differences were used to assess clinical significance.
Results:
Between May 2022 and May 2024, 27 cases were included in the current analyses. Seventeen cases had an X/Y <2.5; 10 had an X/Y ≥2.5. Both cohorts demonstrated significant improvement in PROMIS pain, function, mobility scores (P < .05). Patients with X/Y ≥2.5 demonstrated statistically greater improvement in pain scores than patients with X/Y <2.5 (P = .049) at 1-year follow-up. Ninety-eight percent of patients were satisfied following ZO intervention.
Conclusion:
Percutaneous ZO demonstrated meaningful improvement in patients’ function, pain, and mobility regardless of preoperative X/Y ratio. These findings challenge the use of the <2.5 X/Y threshold as a strict selection criterion. Percutaneous ZO may be a viable option for a broader population of IAT patients than previously considered.
This is a visual representation of the abstract.
Keywords
Introduction
There are multiple surgical options for patients with insertional Achilles tendinopathy (IAT). The Zadek osteotomy (ZO) addresses IAT pathology without directly operating on the Achilles tendon and can be performed open or percutaneously.4,15 For patients with IAT, percutaneous ZO has shown significant improvement in functional outcomes and low complication rates.1,4,12,14
Tourné et al 13 previously proposed a X/Y ratio <2.5 as a way of defining the ideal candidate for ZO. In the initial study by Tourné et al, patients with Haglund deformity were observed to have a significantly lower X/Y ratio (mean, 2.1; range, 1.6-2.4) in comparison to a control (no pathology) group (mean, 2.7; range 2.3-3.2). They found that an X/Y ratio of 2.5 allowed for sensitive (1.0) and specific (0.95) differentiation between patients with and without a Haglund deformity. At this point, it was extrapolated that patients with an X/Y <2.5 had a “long” calcaneus that was responsible for much of their posterior heel pain; Tourné proposed this was the subset of patients who should undergo a subtraction osteotomy of the calcaneus, such as ZO. 13
Importantly, not all patients with IAT have a significant Haglund deformity. Although it has been suggested that an X/Y ratio <2.5 may predict successful outcomes with ZO, 13 this has not been reproduced in the literature. Current literature lacks direct comparisons of ZO outcomes in patients with preoperative X/Y above and below Tourné’s criteria. The purpose of this study was to test the hypothesis that patients with IAT, regardless of X/Y ratio, would improve in pain and function after percutaneous ZO. Evaluation of this hypothesis may help to better identify indication for percutaneous ZO.
Methods
Study Design
This was a retrospective, comparative study conducted following institutional review board approval at one academic medical center. All procedures were performed by one of 2 fellowship-trained orthopaedic foot and ankle surgeons. Patients underwent the percutaneous ZO as previously described by Kaplan et al. 7 The intratendinous calcific spur was not debrided as part of the procedure. Patients with IAT, with or without a Haglund deformity, who failed 3-6 months of nonoperative management were included in this study. All patients were >18 years of age at the time of surgery and were followed for >12 months after their operation. Patients were excluded if they had a history of previous ipsilateral surgery to the Achilles or calcaneus. Between May 2022 and May 2024, 27 consecutive cases met our inclusion criteria. Patients completed a mean follow-up of 21.4 ± 7.3 months (range, 12-36). X/Y measurements were taken on standard, preoperative weightbearing radiographs. Measurements were taken by a single author, masked to the remainder of data collection. Included patients were stratified into 2 cohorts (X/Y <2.5 or X/Y ≥2.5) based on Tourné’s criteria. 13
Data Collection and Analysis
The primary outcome measure was Patient-Reported Outcome Measurement Information System (PROMIS) scores for function, pain, and mobility. PROMIS scores are routinely collected prospectively at each clinic appointment; on retrospective review for the current study, scores at 3, 6, and 12 months were recorded. To determine if postoperative PROMIS scores represented a clinically significant difference from preoperative scores, the minimal clinically important difference was conservatively considered to be 5, as previously described.6,8
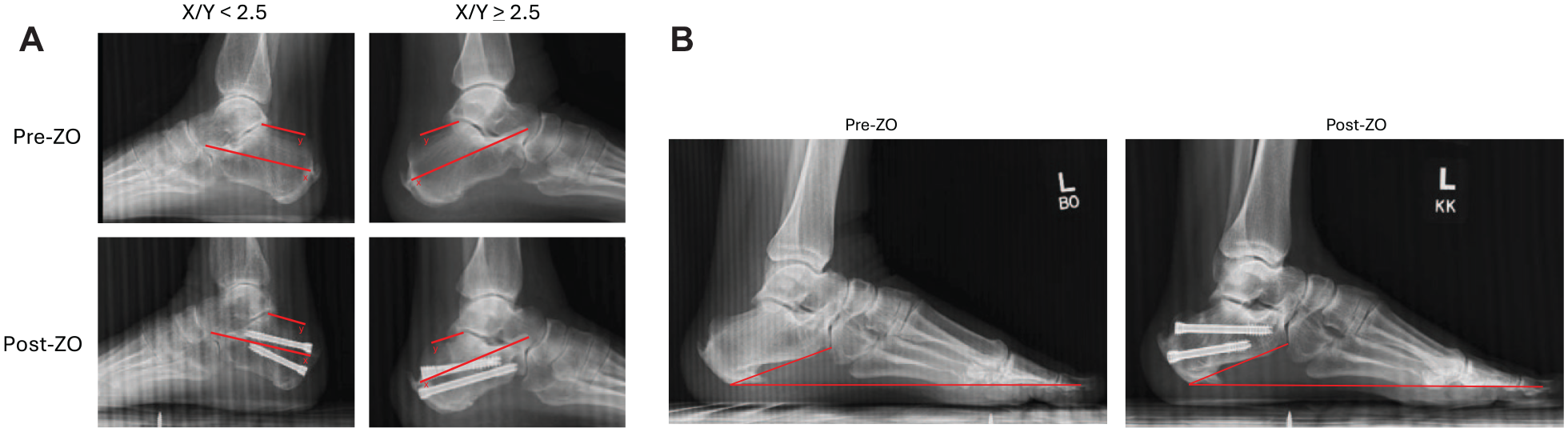
Secondary outcomes included complications, nonunion rates, and reoperation rates. Patient demographics (age, sex, body mass index) were recorded. Radiographic measurements included X/Y ratio (Figure 1A) and calcaneal pitch angle (Figure 1B). Measurements were taken on lateral, weightbearing radiographs from preoperative and final follow-up. The X/Y ratio was calculated as a proportion of calcaneus measurements, where X represents the length from the posterior-most aspect of the calcaneus to the anterior-most aspect of the anterior process, and Y represents the length from the posterosuperior prominence to the posterior-most aspect of the posterior subtalar joint facet. 12 Magnetic resonance imaging (MRI) was not routinely performed preoperatively, so it was not possible to quantitatively determine the degree of IAT in this study. A short report by Hall et al found no difference in patient outcomes between cohorts of patients with various grades of Achilles pathology on MRI, following percutaneous ZO for IAT. 3
(
Given the limited sample size included in the current study, a Shapiro-Wilks test was used to assess for normality; all P values were >.05, indicating that the distribution of our data was normal. Paired t tests were used for within-cohort comparisons, and independent t tests for between-cohort comparisons of continuous variables. Chi-squared analysis was used for comparisons of categorical data between cohorts. Cohen d analysis was used to evaluate the effect sizes of each comparison, and 95% CIs were identified.
Results
Participants and Demographics
On preoperative lateral weightbearing radiographs, 17 cases had X/Y <2.5 and 10 cases had X/Y ≥2.5. Included patients had a mean age of 56.7 ± 11.1 years (range, 33-79) and were not significantly different in age (P = .101), follow-up durations (P = .062), sex distribution (P = .401), body mass index (P = .701), or laterality (P = .722) between cohorts. Eight patients in the X/Y <2.5 cohort had diabetes, whereas only 2 patients in the X/Y ≥2.5 cohort had diabetes (P = .160, Table 1). Additionally, 1 patient in the X/Y <2.5 group was a smoker; there were no smokers in the X/Y ≥2.5 group (P = .434).
Demographic Summary of Patients Included in Each Cohort.
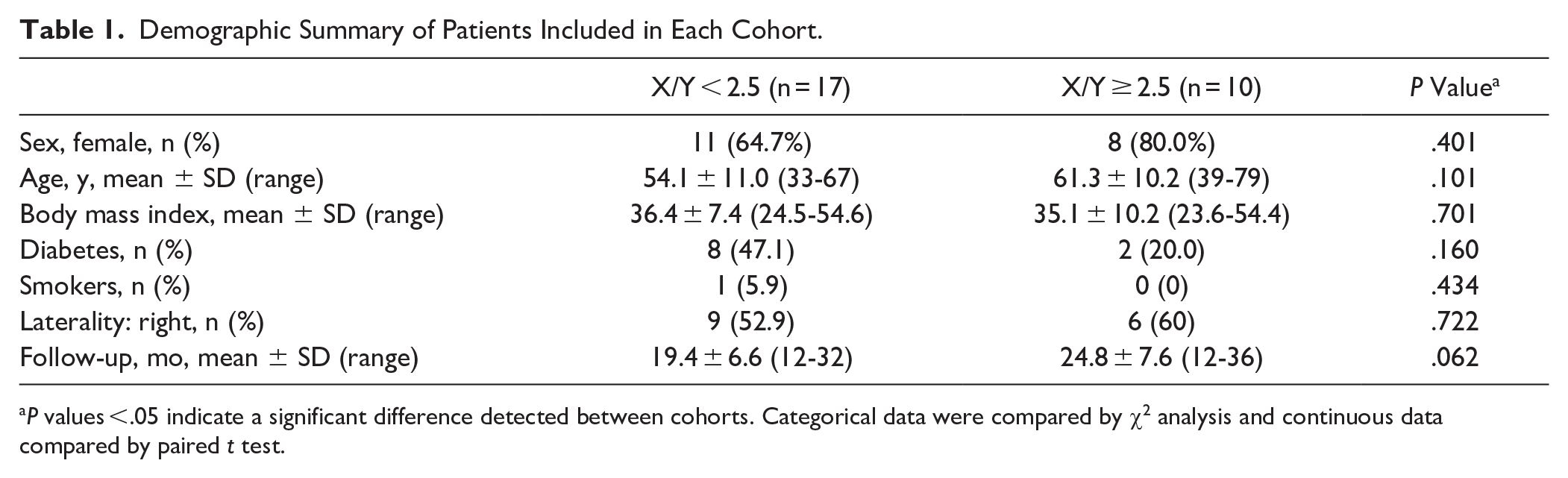
P values <.05 indicate a significant difference detected between cohorts. Categorical data were compared by χ2 analysis and continuous data compared by paired t test.
Primary Outcome
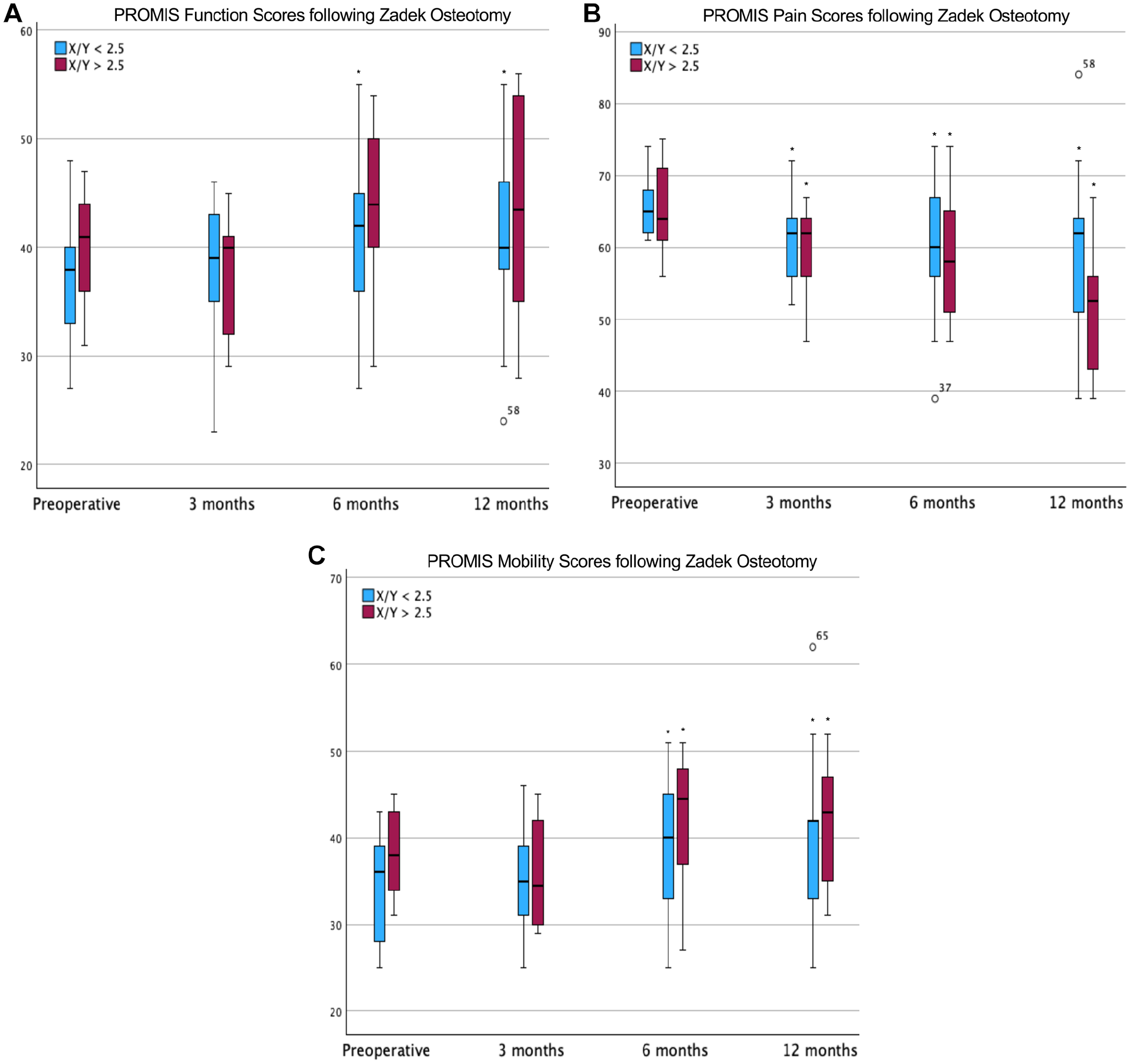
In patients with X/Y <2.5, PROMIS function scores were 37.0 ± 5.3 (range, 33-67) before intervention with percutaneous ZO. At 3 months postoperation, function scores were a mean 38.1 ± 6.4 (range, 23-48; P = .175). By 6 months, function scores had significantly improved to a mean of 40.8 ± 7.8 (range, 27-55; P = .007); similarly, at 12 months, scores were a mean 40.6 ± 8.8 (range, 24-55; P = .005). PROMIS pain scores in this cohort were 65.8 ± 4.0 (range, 61-74) before the intervention. By 3 months, scores had significantly improved (P = .001) to a mean 60.8 ± 5.7 (range, 52-72); similarly, pain scores at 6 and 12 months postoperatively improved to a mean 59.5 ± 9.3 (range, 39-74; P = .003) and 58.6 ± 12.0 (range, 39-84; P = .007), respectively. In this group, PROMIS mobility scores were 34.4 ± 6.3 (range, 25-43) at the preoperative evaluation. Following percutaneous ZO, mean mobility scores improved to 35.5 ± 6.8 (range, 25-46; P = .198), 39.1 ± 7.7 (range, 25-51; P = .008), and 39.4 ± 10.0 (range, 25-62; P = .006) at 3 months, 6 months, and 12 months, respectively (Table 2a).
Summary of Pre- and Postoperative PROMIS Scores at 3, 6, and 12 Months postoperation: X/Y < 2.5 (n = 17).
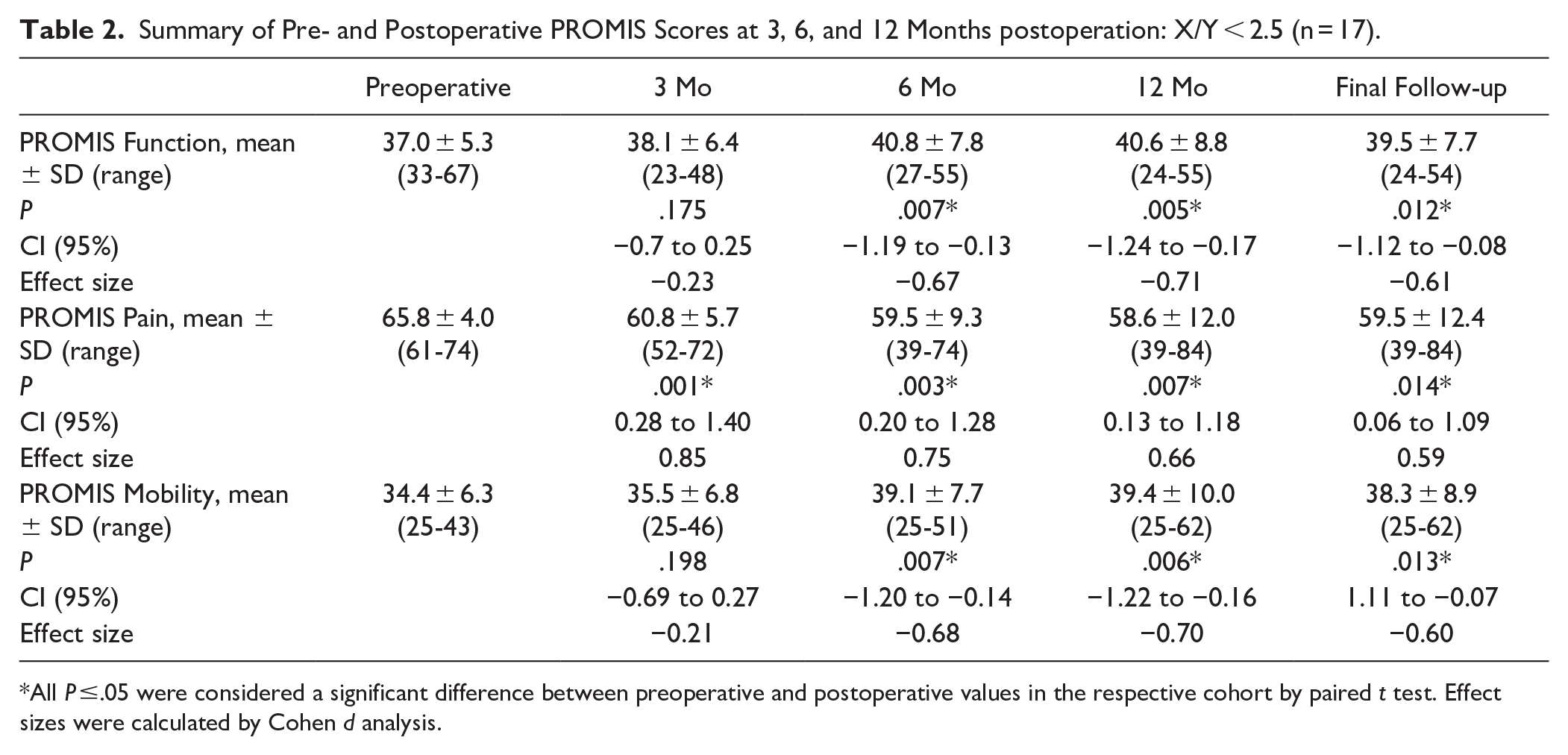
All P ≤.05 were considered a significant difference between preoperative and postoperative values in the respective cohort by paired t test. Effect sizes were calculated by Cohen d analysis.
Meanwhile, in patients with a preoperative X/Y ≥2.5, PROMIS function scores were 40.1 ± 5.4 (range, 31-47) before intervention. Three months following ZO, function scores were a mean of 37.1 ± 5.8 (range, 29-45; P = .136). The function scores improved to a mean 44.0 ± 7.6 (range, 29-54; P = .059) and 43.6 ± 10.1 (range, 28-56; P = .105) at 6 months and 12 months postoperation, respectively. However, these improvements were not significant until the final follow-up of 24.8 ± 7.6 months (range, 12-36); the mean function scores were then 45.0 ± 9.4 (range, 28-54; P = .050). Before intervention, PROMIS pain scores were a mean 65.1 ± 6.7 (range, 56-75). Following percutaneous ZO, scores improved to 59.8 ± 6.5 (range, 47-67; P = .029), 58.7 ± 9.8 (range, 47-74; P = .023), and 51.2 ± 9.2 (range, 39-67; P < .001) at 3, 6, and 12 months, respectively. PROMIS mobility scores were 38.2 ± 4.9 (range, 31-45) prior to intervention and 36.1 ± 6.3 (range, 29-45; P = .211) at 3 months postoperation. Mobility scores significantly improved at 6 and 12 months postoperatively to a mean of 42.6 ± 7.7 (range, 27-51; P = .031) and 41.8 ± 7.1 (range, 31-52); P = .027), respectively (Figure 2; Table 3).
PROMIS (
Summary of Pre- and Postoperative PROMIS Scores at 3, 6, and 12 Months Postoperation: X/Y ≥ 2.5 (n = 10).
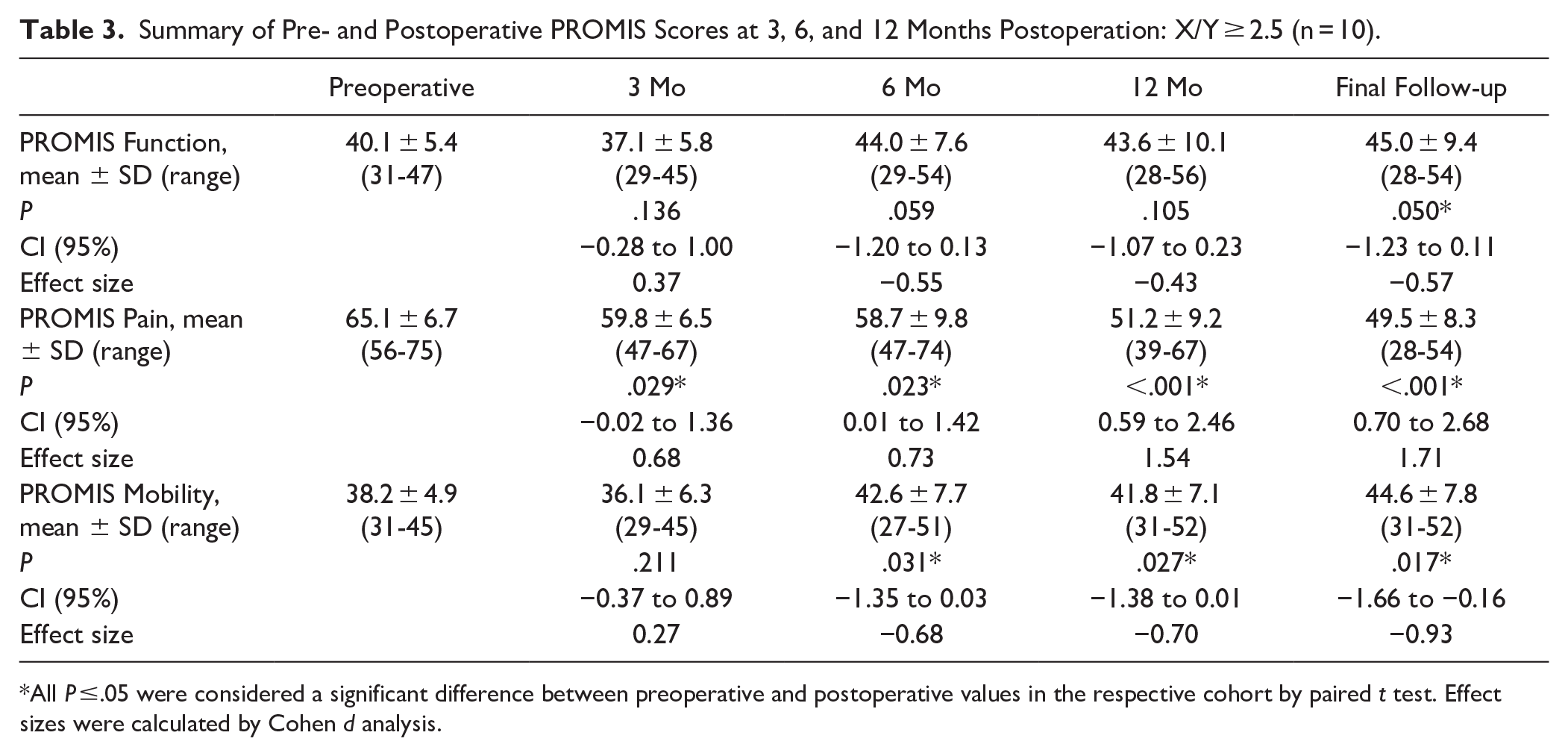
All P ≤.05 were considered a significant difference between preoperative and postoperative values in the respective cohort by paired t test. Effect sizes were calculated by Cohen d analysis.
When comparing the preoperative-to-postoperative changes (Δ) observed in each cohort, there was no difference in Δ function or Δ mobility scores at 3, 6, or 12 months postoperatively. However, patients with X/Y ≥2.5 preoperatively had a larger change in PROMIS pain scores (P = .013) in comparison to patients in the X/Y <2.5 cohort (Table 4). Of note, the mean Δ PROMIS pain scores were each at or above the minimal clinically important difference in both cohorts by the 3-month follow-up.
Summary of Change in PROMIS Scores at 3, 6, and 12 Months Postoperation.
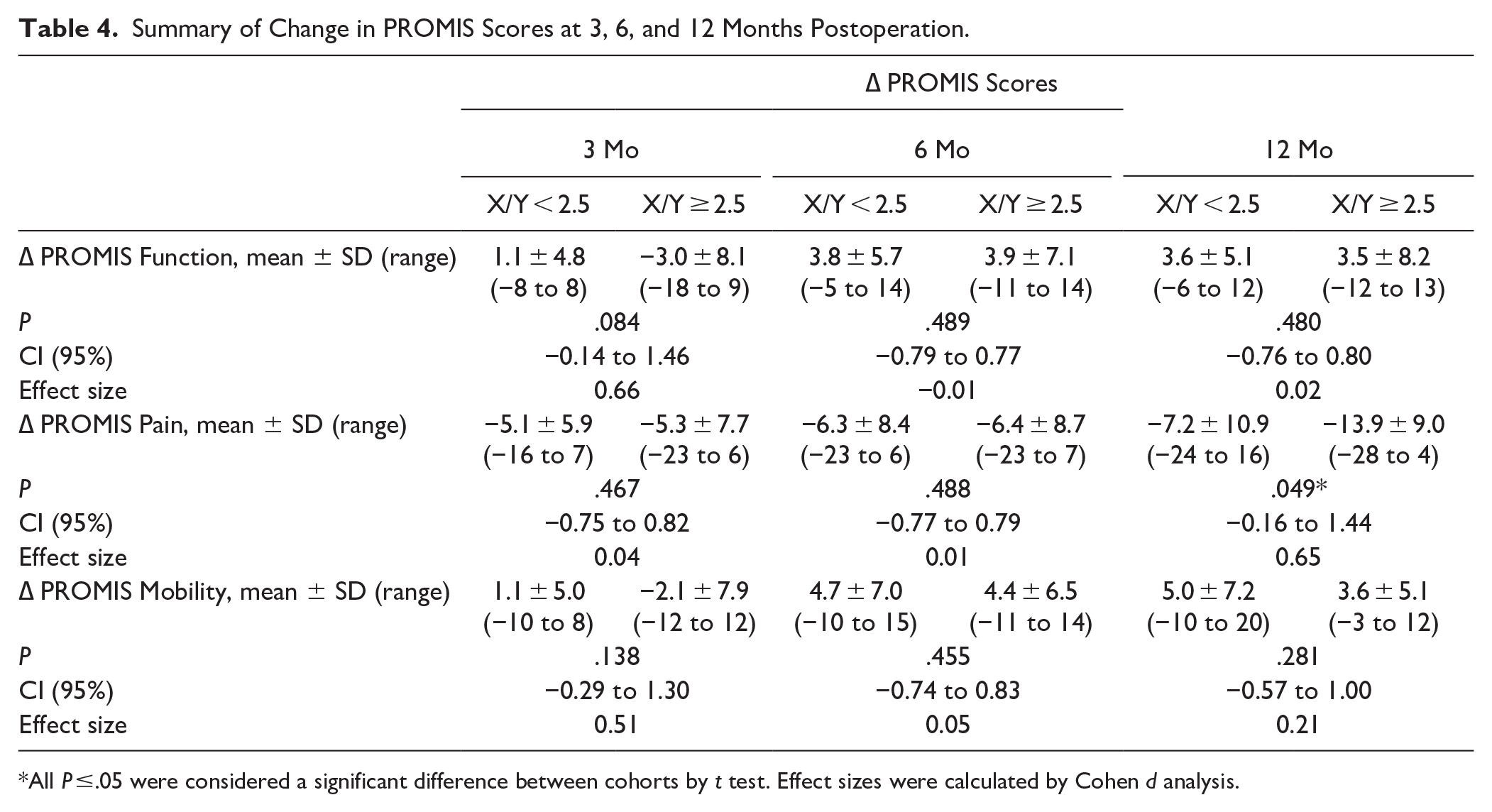
All P ≤.05 were considered a significant difference between cohorts by t test. Effect sizes were calculated by Cohen d analysis.
Secondary Outcomes
Neither patients in the X/Y <2.5 cohort nor in the X/Y ≥2.5 cohort demonstrated a significant difference in calcaneal pitch angle following percutaneous ZO (P = .818, .345). Patients with an X/Y <2.5 had a mean calcaneal pitch angle of 22.3 ± 5.9 (range, 12.5-31.7) before intervention, and 22.4 ± 5.6 (range, 14.6-30.5) following ZO. Similarly, patients in the X/Y ≥2.5 cohort had a mean calcaneal pitch angle of 21.3 ± 7.7 (range, 12.1-36.1) before percutaneous ZO, and 22.0 ± 7.1 (range, 13.1-36.1) at final postoperative follow-up. Patients in both cohorts demonstrated a significant increase in the X/Y ratio following ZO (P < .001). When comparing the preoperative-to-postoperative changes observed within each cohort (Δ), there was no difference detected in the amount of change seen in X/Y (P = .311) or calcaneal pitch measurements (P = .248) (Table 5).
Summary of Preoperative, Postoperative, and the Calculated Change (∆) in Calcaneal Pitch Angle, and X/Y Ratio Measurements.
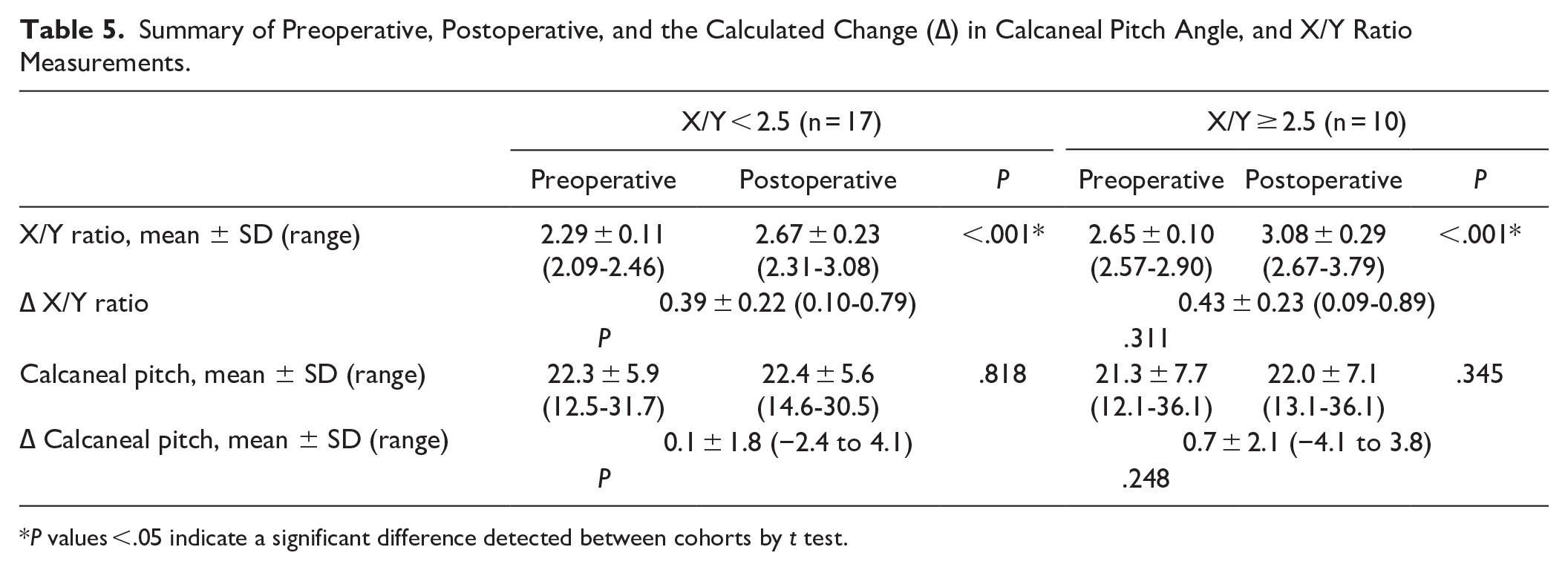
P values <.05 indicate a significant difference detected between cohorts by t test.
Complications were minimal. In the X/Y <2.5 cohort, there was 1 case of postoperative sural neuropathy treated with injection. Separately, 1 patient in this cohort experienced recurring pain and was revised with an open midline Achilles tendon splitting approach. There were no instances of nonunion, infection, or other complications. There was no significant difference detected between cohorts regarding revision (P = .434). Furthermore, 98% of patients were satisfied with their percutaneous ZO procedure and reported a willingness to undergo the procedure again.
Discussion
Numerous studies have reported outcomes and patient satisfaction following open or percutaneous ZO.1,4,10 However, the explicit indications for ZO, as opposed to other surgical interventions for IAT and Haglund deformity, remain largely undefined in the literature. Although Tourné et al 13 suggested an X/Y <2.5 can be used as a criterion to predict successful ZO intervention, findings in the current study conflict with this suggestion. The current study found patients with IAT, regardless of X/Y ratio, statistically and clinically improved function, pain, and mobility after percutaneous ZO at minimum 12 months’ follow-up. Interestingly, patients with X/Y ratio ≥2.5 (outside of Tourné’s criteria) were observed to have a significantly greater improvement in PROMIS pain scores at 12 months (P = .049) and final follow-up (P = .013) in comparison to the X/Y <2.5 group.
Of note, Tourné et al 13 did not analyze outcomes following ZO in cohorts of patients within and outside of their criteria. Although the X/Y ratio may be predictive of patients with Haglund deformity, not all patients with IAT have a posterosuperior prominence of the calcaneus; however minimally invasive ZO has been indicated for surgical management of IAT with or without this deformity, with many studies reporting good short- to midterm outcomes.4,5 Tourné et al 13 also suggested that in a successful ZO intervention, an X/Y >2.5 would be achieved. 12 However, despite the significant improvement in patient symptoms and 98% satisfaction rate observed in the current study, not all patients achieved a postoperative X/Y >2.5.
Previously, Nakajima analyzed the X/Y ratio in patients with symptomatic vs asymptomatic IAT on radiographs. 9 Although there was a statistically significant increase in the size of Haglund deformity and amount of calcification about the Achilles tendon insertion in the symptomatic cohort (P < .05), they found no difference in patients’ X/Y ratio in comparison to the asymptomatic group (P = .87). Of note, the mean X/Y ratio in both groups was reportedly >2.5 (2.8 ± 0.3). 9 Similar to the findings in the current study, their observations may suggest the X/Y ratio is not analogous to severity of insertional Achilles disease.
Other interventions for IAT have demonstrated a simultaneous increase in X/Y and improvement in patient-reported outcome metrics. A recent multicenter, prospective analysis of open vs endoscopic Haglund resection for IAT demonstrated a significantly greater increase in X/Y ratio in the endoscopic cohort. 11 The endoscopic cohort also had a faster return to sport at 3 months and greater improvement in EFAS scores at 6 months. Despite improvement in patient outcome scores, many patients maintained an X/Y ratio <2.5 postoperatively. 11 Similar to findings in the current study, these observations may suggest that a specific X/Y ratio may not correlate with a successful intervention for patients with IAT.
The current study was limited in ways that are important to note. As this was a retrospective study, cohorts were not matched in size, age, sex, or laterality or other confounders. While there were no significant differences among the demographic profile or complications observed between cohorts, there was a larger proportion of patients with diabetes in the X/Y <2.5 group (P = .160), and all complications occurred in patients with X/Y <2.5. It is reasonable to suggest with the limited size of our cohorts that these factors still may have influenced outcome scores; further investigation is warranted to expand on these findings. Additionally, many patients do not have a long calcaneus but IAT without Haglund deformity and thus will likely have an X/Y ratio >2.5. However, even without a Haglund deformity, patients with IAT benefit from a minimally invasive Zadek as shown in multiple studies.2,4,7,10 Another notable concern is that radiographic measurements were performed by a single rater, and MRI data were not uniformly available to assess severity of tendinopathy. Finally, we included consecutive cases with a minimum follow-up of 12 months (mean 21.4), which could limit the differences we were able to detect within each cohort and/or between cohorts.
Nevertheless, despite these limitations, this small retrospective study found similar improvement in outcome scores following percutaneous ZO for IAT in patients with an X/Y ratio <2.5 and ≥2.5 and suggests that the preoperative X/Y ratio may not be a useful standalone criterion for patient selection. Both groups demonstrated improvements exceeding minimal clinically important difference thresholds, reinforcing the clinical relevance of the observed changes. The high satisfaction rate (98%) and low complication rate further support the procedure’s safety and efficacy in a broader patient population.
Conclusion
This small sample-sized study found that patients with insertional Achilles tendinopathy experienced significant and clinically meaningful improvements in PROMIS pain, function, and mobility scores after percutaneous Zadek osteotomy, regardless of their preoperative X/Y ratio. Notably, patients with X/Y ≥2.5—outside of the traditionally recommended range—demonstrated greater pain improvement at 1 year. These findings suggest that reliance on an X/Y <2.5 threshold may unnecessarily restrict candidacy for ZO. Although the sample size limits generalizability, the results support considering percutaneous ZO for a broader subset of patients with IAT. Further prospective research is needed to clarify long-term outcomes and refine selection criteria.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007251341890 – Supplemental material for The Effect of Preoperative X/Y Ratio on Clinical Outcomes following Percutaneous Zadek Osteotomy for Insertional Achilles Tendinopathy
Supplemental material, sj-pdf-1-fai-10.1177_10711007251341890 for The Effect of Preoperative X/Y Ratio on Clinical Outcomes following Percutaneous Zadek Osteotomy for Insertional Achilles Tendinopathy by Sarah Hall Kiriluk, Anne Holly Johnson, Jonathan R. M. Kaplan, Ettore Vulcano, Thomas Lewis, Peter Lam, Oliver Schipper, J. Benjamin Jackson and Tyler A. Gonzalez in Foot & Ankle International
Footnotes
Ethical Approval
Ethical approval for this study was obtained from Institutional Review Board at Prisma, University of South Carolina [
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Anne Holly Johnson, MD, reports disclosures relevant to article from royalties: Novastep, Treace Medical Concepts; stock: Carbon22, Altior Traima, BICMD. Jonathan R. M. Kaplan, MD, reports disclosures relevant to article as consultant for Artelon, Edge Surgical, Enovis / Novastep, Exactech, Surgical Fusion Technologies, Treace Medical Concepts, Vilex, Surgebright; royalties: Surgical Fusion Technologies, Treace Medical Concepts, Vilex. Ettore Vulcano, MD, reports disclosures relevant to article as consultant for Novastep, Treace, Vilex, Surgebright; royalties: Surgical Fusion Technologies, Treace Medical Concepts, Vilex. Thomas Lewis, MBChB(Hons), BSc(Hons), MRCS, MFSTEd, reports disclosures relevant to article of royalties and consulting from Vilex beyond the scope of this study and general disclosures from PhD tuition fees supported by MIFAS. Peter Lam, MBBS(Hons), FRACS, reports disclosures relevant to article as consultant for Enovis. Oliver Schipper, MD, reports disclosures relevant to article as consultant for Treace Medical Concepts Inc, SFI, Enovis, Exactech; royalties: Treace Medical Concepts Inc, SFI, Enovis. J. Benjamin Jackson III, MD, MBA, reports disclosures relevant to article as consultant for Synthes. Tyler A. Gonzalez, MD, MBA, reports disclosures relevant to article as consultant for Treace Medical Concepts Inc, Surgical Fusion Technologies, Stryker, Enovis, Exactech, Surgebright; royalties: Surgical Fusion Technologies, Treace Medical Concepts, Vilex. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.