
Abstract
Background:
Limited literature is available to guide surgeons on which patients with insertional Achilles tendinopathy (IAT) may be the best candidates for minimally invasive dorsal closing wedge calcaneal Zadek osteotomy (MIS ZO). We hypothesized that the severity of IAT on preoperative magnetic resonance image (MRI) may correlate with post-operative functional outcomes and help guide patient selection for treatment with MIS ZO.
Methods:
Patients who underwent MIS ZO for IAT ± Haglund deformity were identified and retrospectively analyzed. IAT severity was graded on preoperative MRI. Patient Reported Outcome Measurement Information System (PROMIS) scores, complications, and revisions were recorded. Continuous data were compared by analysis of variance with Bonferroni post hoc analysis.
Results:
Seventeen patients treated with MIS ZO, with follow-up >6 months, and preoperative MRI met our inclusion criteria. PROMIS pain scores significantly improved in patients with IAT grades 1-3, with 5, 5, and 7 patients, respectively, in each subgroup. In this small series we only identified statistically significant improvements in PROMIS function (P = .031), and mobility (P = .009) scores were only observed in patients with grade 2 pathology. Sixteen of 17 patients (94.2%) were very satisfied with their procedure and would undergo it again.
Conclusion:
In this pilot study, we did not find preoperative MRI findings to correlate well with patient-reported outcome scores following MIS ZO.
Level of Evidence:
Level IV, case series.
This is a visual representation of the abstract.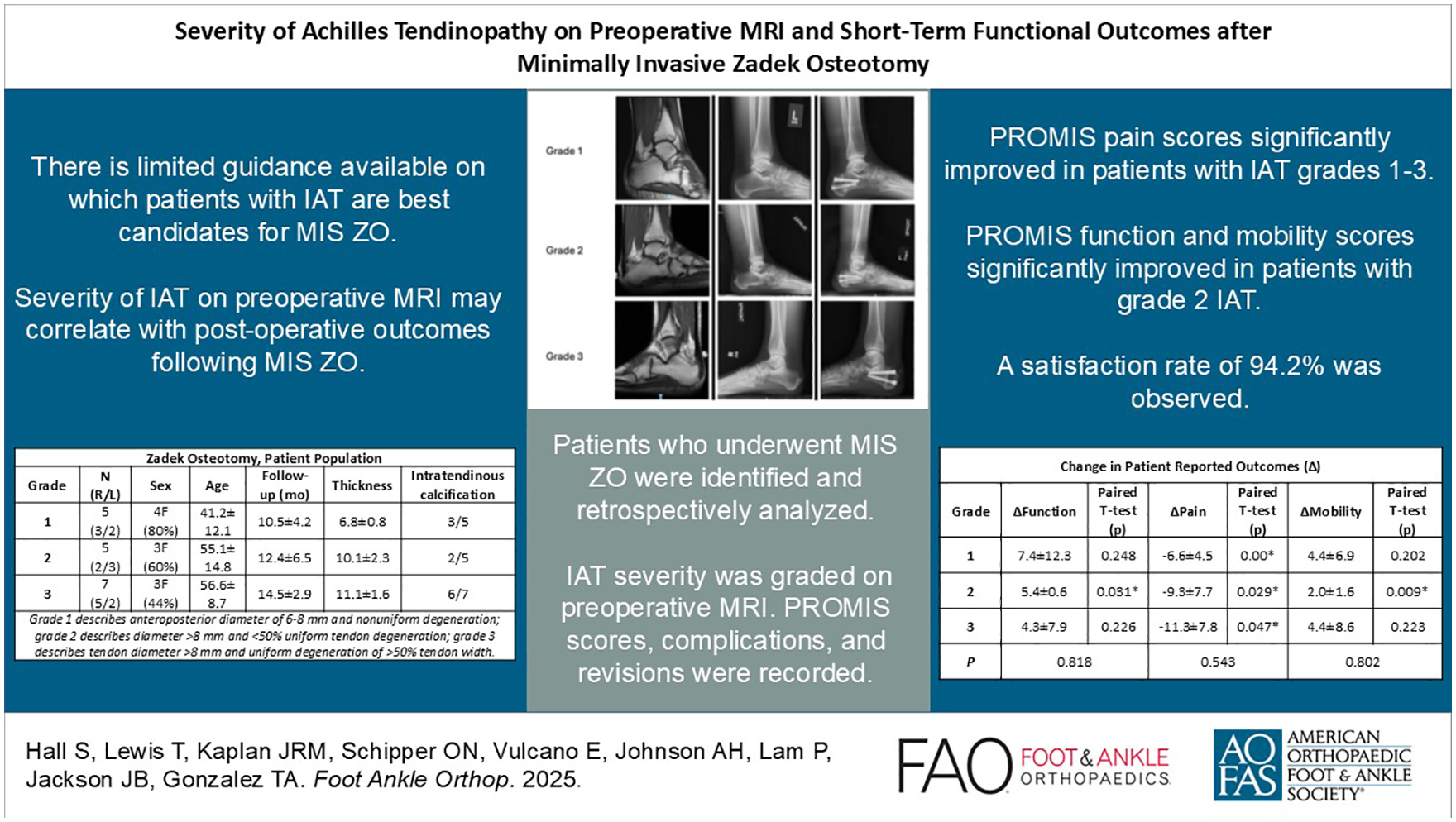
Keywords
Introduction
The minimally invasive Zadek osteotomy (MIS ZO) is a safe and effective surgical intervention for patients with insertional Achilles tendinopathy (IAT) ± Haglund deformity. 4 However, there is little evidence to define the best candidates for MIS ZO. Previous studies have proposed measurements such as Chauveaux-Liet angle (>12 degrees), X/Y ratio (>2.5), increased calcaneal pitch angle (>30 degrees) on standard radiographs to identify appropriate patients for MIS ZO.7 -9 Still, very few studies report patient outcomes following ZO with respect to these radiographic parameters.
Although standard radiographs may demonstrate structural causes for IAT, magnetic resonance imaging (MRI) allows for direct visualization of the tendinopathy. Although it has not been formally evaluated in the literature, it has been suggested previously that patients with severe degeneration and calcification about the Achilles may be contraindicated for ZO.2,3 Accordingly, it has been suggested that MRI analysis of IAT may help identify patients who are best suited for MIS ZO rather than alternative interventions. 2 However, MRI is not a standard component of surgical evaluation for IAT, and there is very little data in the literature to correlate MRI findings to postoperative outcomes in patients with IAT, especially following MIS ZO. Accordingly, the current study aimed to compare postoperative outcomes among patients with various grades of IAT on MRI who underwent MIS ZO to see if preoperative MRI findings affected functional outcomes after MIS ZO.
Methods
Patients with IAT were first treated with nonoperative management strategies such as shoe wear modifications, activity modifications, eccentric loading therapy, formal physical therapy, and anti-inflammatory medication. If symptoms persisted or worsened after 3-6 months, surgery was offered. The surgeons participating in the current study consider MIS ZO to be first-line surgical management offered to all patients with IAT of any severity. Patients who required surgery underwent MIS ZO as previously described. 5 A 10-mm dorsal based wedge was removed from the calcaneus through <5-mm incisions. The MIS ZO was performed with the assistance of a Shannon burr, copious cooled irrigation, and fluoroscopic guidance. Surgeons used the cut guide described by Kaplan et al. 5 Patients were nonweightbearing for 2 weeks, weightbearing as tolerated in a boot from postoperative week 2-6, and in regular shoes by 6 weeks. Patients were identified and retrospectively analyzed at a minimum of 6-month follow-up.
All patients underwent MRI prior to surgical intervention. Achilles pathology was graded on MRI by a fellowship trained orthopaedic foot and ankle surgeon as previously described by Nicholson et al. 6 Preoperative and postoperative Patient Reported Outcome Measurement Information System (PROMIS) scores, complications, and revisions were recorded for each patient and compared using a paired t test. Continuous data were compared by analysis of variance; all categorical data were compared using χ2 analysis.
Results
Between June 2021 and April 2024, a total of 17 patients (10 female, 7 male) treated with MIS ZO met our inclusion criteria. The mean follow-up duration was 12.5 ± 3.9 months and mean age 51.0 ± 8.9 years. There were no significant differences in follow-up duration or age of patients among cohorts (P = .453 and .094, respectively) (Table 1).
Zadek Osteotomy, Patient Population.

Grade 1 describes an anteroposterior diameter of 6-8 mm and nonuniform degeneration; grade 2 describes diameter >8 mm and <50% uniform tendon degeneration; grade 3 describes tendon diameter >8 mm and uniform degeneration of >50% tendon width.
PROMIS pain score improved postoperatively in patients with grade 1 (66.0 ± 3.39 to 59.4 ± 7.20, P < .01), grade 2 (66.1 ± 3.58 to 56.8 ± 10.1, P = .029), and grade 3 (69.4 ± 5.83 to 58.1 ± 7.43, P = .047) IAT. In patients with grade 2 pathology, PROMIS function scores significantly improved (37.8 ± 6.10 to 66.1 ± 3.58, P = .031) and mobility scores significantly improved (37.0 ± 5.7 to 39.0 ± 6.4, P = .009). We did not identify a significant change in function or mobility in the grade 1 or grade 3 cohorts (Table 2). There were no statistically significant differences detected in the change (∆; preoperative – postoperative) in PROMIS function, pain, or mobility scores between cohorts (P = .818, .543, and .802, respectively) (Table 3).
Zadek Osteotomy, Patient-Reported Outcomes. a

Abbreviation: PROMIS, Patient Reported Outcome Measurement Information System.
Data are presented as mean ± SD. Data compared between groups by independent sample, 2-tailed t test. P < .05 considered to be statistically significant for each analysis.
Change in Patient-Reported Outcomes (∆). a

Data are presented as mean ± SD. The data were compared between groups by independent sample, 2-tailed t test, and compared within each group by paired, 2-tailed t test. *P <.05 is considered to be statistically significant for each analysis.
One patient experienced transient neuritis that self-resolved at 3 months without further treatment and 1 patient required revision surgery to an open Haglund resection due to ongoing symptoms of IAT; both of these were in the grade 3 cohort. Two patients had persistent plantar fasciitis at final follow-up. Sixteen of the 17 patients (94.2%) were very satisfied with their procedure and would undergo it again.
Discussion
The current study demonstrated significant improvement in patient-reported pain following ZO in patients with grade 1-3 IAT. Statistically significant improvement in patient-reported function and mobility following MIS ZO was only seen in patients with grade 2 IAT. However, there was no statistical difference detected in the amount of change (∆) observed between preoperative and postoperative PROMIS pain, function, or mobility scores among cohorts.
Nicholson et al 6 described the severity of IAT on MRI as a proportion of the amount of degeneration compared with the total diameter of the tendon. According to their grading system, nonuniform degeneration of <8 mm on MRI (grade 1 IAT) is likely to be successfully treated with conservative techniques. Nevertheless, Nicholson et al 6 reported about 12.5% of their patients with grade 1 IAT still required surgical intervention to achieve symptom resolution. Degeneration that is uniform and/or exceeds 8 mm (grade 2, grade 3) are more likely to require surgical management; 90.8% of their patients with grade 2 and 70.4% of their patients with grade 3 IAT required surgery. 6 Although this grading scale may offer guidance on which patients will historically fail nonoperative management, few conclusions have been drawn in relation to postoperative outcomes among grades of IAT. Furthermore, there has been no investigation into which patients will be best suited for MIS ZO in comparison to other procedures for IAT, such as the open midline Achilles tendon–splitting approach.
It has been suggested that patients with extensive degeneration and calcification of the Achilles, such as grade 3 IAT, may be contraindicated for MIS ZO. 3 However, data from this study suggest MIS ZO may be effective management, no matter the grade of IAT. We found that patients with grade 3 IAT experienced significant improvement in their pain following MIS ZO. Of note, 1 patient with grade 3 IAT did experience persistent symptoms and required a revision to an open Haglund resection. However, this was likely due to inadequate wedge resection, less than 1 cm, which did not allow for adequate anteriorization of the calcaneal tuber and posterior heel decompression. Overall, this correlates to a 5.9% revision rate, and a 94.1% satisfaction rate in our small retrospective cohort study. Also of note, there were no differences detected in the preoperative PROMIS scores reported between cohorts. These findings suggest that despite differences in IAT on MRI, patients’ clinical presentation may be similar between cohorts. This further supports the argument that MRI may not be a necessary component of preoperative evaluation in patients with IAT.
Few other studies have attempted to correlate radiographic findings and surgical management of IAT. A retrospective study by Baumbach et al 1 graded 88 patients with IAT by 15 separate radiographic/MRI parameters. The criteria previously described by Van Dijk in 2011 was used to grade IAT on MRI 10 ; the Victorian Institute of Sport Assessment–Achilles and general health questionnaires were used as patient-reported outcome measures. All patients in their study underwent an open midline Achilles tendon–splitting procedure for IAT.
In comparison to the open midline splitting technique, the MIS ZO is a minimally invasive procedure that decompresses the retrocalcaneal space without detachment and reattachment of the Achilles. Recent retrospective analysis by Hall et al 4 demonstrated significant improvement in patient reported outcomes, a high rate of patient satisfaction (98.1%), and a lower rate of complication (3.8%) in over 100 patients, at minimum 2 years following MIS ZO. Despite the vastly different surgical approaches used, Baumbach et al and the current study had similar findings. Baumbach reports a 77.0% rate of patient satisfaction and no correlation in patient-reported outcomes and MRI parameters such as tendon degeneration, partial tendon rupture, retrocalcaneal bursitis, posterosuperior calcaneal prominence, or superficial calcaneal bursitis. 1 Neither study found any statistical association between preoperative MRI findings and postoperative outcomes; MRI findings may not be predictive of surgical outcomes for patients with IAT. Therefore, MRI may not be a necessary component of preoperative evaluation in this population.
This study is not without limitations; as a retrospective study, our outcome measures reflect patient-reported pain, function, mobility. Our outcome measures do not include an objective evaluation of the Achilles tendon function (ie, push-off strength) following MIS ZO. Additionally, we did not compare the outcomes of MIS ZO to those of an open Haglund resection; therefore, we cannot define any particular grade of IAT severity that may have superior outcomes with one procedure over another. At this time, we can only report satisfactory outcomes with the MIS ZO in grade 1-3 IAT. Further, MRI may not be a necessary component of preoperative evaluation in patients with IAT. Future investigation in the form of multicenter, large, prospective trials are required to properly evaluate the biomechanical advantage of MIS ZO in comparison to other procedures for IAT ± Haglund deformity.
Conclusion
These early data in this pilot study suggests that patients with IAT who failed >3-6 months of nonoperative management may improve after MIS ZO, regardless of IAT severity on preoperative MRI. Further, 94.1% of all patients were satisfied with their procedure. MRI may not be predictive of successful ZO intervention. Further, large prospective studies are warranted to further investigate outcomes and indications of MIS ZO.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251322775 – Supplemental material for Severity of Achilles Tendinopathy on Preoperative MRI and Short-term Functional Outcomes After Minimally Invasive Zadek Osteotomy
Supplemental material, sj-pdf-1-fao-10.1177_24730114251322775 for Severity of Achilles Tendinopathy on Preoperative MRI and Short-term Functional Outcomes After Minimally Invasive Zadek Osteotomy by SarahRose Hall, Thomas Lewis, Jonathan R. M. Kaplan, Oliver N. Schipper, Ettore Vulcano, A. Holly Johnson, Peter Lam, J. Benjamin Jackson and Tyler Gonzalez in Foot & Ankle Orthopaedics
Footnotes
Appendix
Ethical Approval
IRB application was completed, and the study was approved. Project title: Patient outcomes and radiographic analysis of percutaneous Zadek osteotomy [2170226-2].
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thomas Lewis, MBChB(Hons), BSc(Hons), MRCS, MFSTEd, reports disclosures relevant to manuscript as consultant for Vilex. Jonathan R. M. Kaplan, MD, reports disclosures relevant to manuscript as consultant for Artelon, Edge Surgical, Enovis / Novastep, Exactech, Surgical Fusion Technologies, Treace Medical Concepts, Vilex, Surgebright; and royalties for Surgical Fusion Technologies, Treace Medical Concepts, Vilex. Oliver N. Schipper, MD, reports disclosures relevant to manuscript as consultant for Treace Medical Concepts Inc, SFI, Enovis, Exatech; and royalties for Treace Medical Concepts Inc, SFI, Enovis. Ettore Vulcano, MD, reports disclosures relevant to manuscript as consultant for Novastep, Treace, Vilex, Surgebright; royalties for Surgical Fusion Technologies, Treace Medical Concepts, Vilex; and stock options for GLW, Curvebeam. A. Holly Johnson, MD, reports disclosures relevant to manuscript from royalties for Novastep, Treace; stock options for Carbon22, Altior Traima, BICMD. Peter Lam, MBBS(Hons), FRACS, reports disclosures relevant to manuscript as consultant for Enovis. J. Benjamin Jackson III, MD, MBA, reports disclosures relevant to manuscript as consultant for Synthes. Tyler Gonzalez, MD, MBA, reports disclosures relevant to manuscript as consultant for Treace Medical Concepts Inc, Surgical Fusion Technologies, Stryker, Enovis, Exactech, Surgebright; royalties for Surgical Fusion Technologies, Treace Medical Concepts, Vilex. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.