
Abstract
Background:
Hallux rigidus is a degenerative condition of the first metatarsophalangeal (MTP) joint that can significantly impair function and quality of life. The introduction of polyvinyl alcohol (PVA) hydrogel implants, such as Cartiva, offered an alternative to arthrodesis by preserving joint motion. However, failures of these implants, often resulting in bone loss and joint instability, present a challenge for revision surgery.
Methods:
We report the case of a 43-year-old woman with persistent pain and functional limitations after a failed PVA hydrogel implant in the first MTP joint. The revision surgery involved a biologic resurfacing using the Osteochondral Autograft Transfer System (OATS) with a graft harvested from the ipsilateral femoral condyle, complemented by interpositional arthroplasty with a dermal graft and a proximal phalanx closing wedge osteotomy to correct residual hallux valgus.
Results:
At the 3-year follow-up, the patient-reported complete resolution of pain and returned to full activity with improved range of motion (40 degrees dorsiflexion, 15 degrees plantarflexion). Radiographic evaluation demonstrated graft incorporation and restoration of joint space, confirming the success of the procedure.
Conclusion:
This case highlights the potential of OATS combined with interpositional arthroplasty as a viable option for revision surgery in complex cases of failed synthetic cartilage implants in hallux rigidus. By addressing bone loss and preserving joint function, this approach provides a patient-specific alternative to traditional arthrodesis. Further studies are warranted to establish the long-term efficacy of this technique in similar cases.
Level of Evidence:
Level V, case report.

Introduction
Hallux rigidus, the second most prevalent condition affecting the first metatarsophalangeal (MTP) joint after hallux valgus, manifests in approximately 25% of individuals over 50 years old, with an overall prevalence of 1 in 40.13,24,38 Although most instances of hallux rigidus are idiopathic, associations with arthritic changes resulting from traumatic or iatrogenic causes have also been observed.31,34,38 Chronic pain, altered gait, and shoewear discomfort are common complaints because of joint degeneration and osteophytic growths. Nonoperative management, including nonsteroidal anti-inflammatory drugs, injections, activity modifications, and footwear adjustments, are the initial management for more than half of hallux rigidus patients.11,38 Surgical interventions, including cheilectomy for early stages and joint fusion for advanced arthritis, are considered for nonresponsive cases. However, addressing bone loss and achieving optimal outcomes in revision surgeries is challenging, with limited literature available to guide the selection of the most suitable surgical approach to eliminate pain, preserve motion, and restore patients to an active lifestyle.16,19,39
In the mid-2000s, a groundbreaking polyvinyl alcohol (PVA) hydrogel implant, known as Cartiva, was introduced. Achieving FDA approval as the first synthetic cartilage replacement in 2016, it rapidly secured a significant market share for addressing hallux rigidus.8,52 The initial studies assessed outcomes in comparison to fusion surgery.2,23 Although initial results were promising, numerous reports have highlighted less satisfactory outcomes.5,10 Additionally, managing failed implant surgeries poses challenges in terms of addressing bone loss, and MTP joint fusion often becomes the ultimate outcome for preserving motion.9,35,42,43,45
This case report and literature review highlights the journey of a 43-year-old woman who continued to battle with pain and functional limitations of her first MTP after failing previous conservative and surgical treatment modalities. The complexity of her case necessitated a nuanced approach, demanding careful consideration of treatment options.
Our discussion examines the historical progression of cartilage replacement, tracing the evolution from early synthetic implants to present-day challenges. We explore various techniques, such as arthrodesis and alternative implants, to provide a comprehensive overview of hallux rigidus revision surgery. This report introduces the osteochondral autograft transfer system (OATS) in combination with interpositional soft tissue arthroplasty, as a novel approach for revision surgery. Although traditionally used for other conditions, our adaptation of the OATS procedure for hallux rigidus offers a unique option, particularly for cases with limited or failed previous surgeries. To our knowledge, this is the first documented case of an OATS procedure combined with soft tissue interposition after a failed PVA implant. As efforts persist in search of effective solutions, our findings offer valuable insights for clinicians and researchers dedicated to advancing hallux rigidus treatment.
Clinical Case
A 43-year-old female patient presented with a 10-year history of right foot pain and a diagnosis of hallux rigidus. She had previously undergone 2 prior surgeries at an outside hospital. Her most recent surgery 2 years prior included synovectomy, revision dorsal cheilectomy, and placement of a polyvinyl alcohol (PVA) hydrogel implant. The patient reported continued pain after surgical intervention with unrelenting worsening pain over the preceding 6 months. On physical examination, she had a surgical excision over the dorsum of her first MTP joint. She had painful passive and active range of motion of her first MTP. Her dorsiflexion was 10 degrees and her plantarflexion 30 degrees. Preoperative CT scan demonstrated a substantial defect at the distal aspect of the first metatarsal associated with the implant, along with dorsal cortex loss, bone-on-bone impingement of the phalanx with cystic degeneration, and hallux valgus drift at the MTP joint (Figures 1 and 2). Additionally, magnetic resonance imaging of the right foot depicted an osteolytic defect at the distal pole of the first metatarsal and extensive intra-articular synovitis. Further imaging confirmed implant failure, resulting in complete collapse, bone-on-bone impingement, and dorsal osteophyte formation (Figure 3).

Computed tomographic scan 3D reconstruction reveals a defect at the end of the first metatarsal, associated to the implant. (A) Lateral/oblique view, (B) Dorsal view.

Computed tomographic images show a defect at the end of the first metatarsal associated to the implant, with loss of dorsal cortex and bone-on-bone impingement. (A) Sagittal view, (B) Axial view.

Magnetic resonance imaging of the right foot showing an osteolytic defect at the end of the first metatarsal. (A) Sagital view, (B, C) Axial view at different levels.
Considering the patients’ symptoms and in light of her imaging findings, a comprehensive discussion was had with the patient where multiple treatment modalities were discussed, including (1) arthrodesis, (2) interpositional arthroplasty with synthetic cartilage covering with cautery foam, (3) interpositional arthroplasty with cortical cancellous graft from the ipsilateral calcaneus, and (4) biologic resurfacing with an OATS from the ipsilateral knee. After careful consideration of the risks and benefits of each procedure, the patient consented to undergo a biologic resurfacing with an OATS from her ipsilateral knee. In addition, the patient would undergo a lateral closing wedge osteotomy of the base of proximal phalanx of her first ray in order to address residual hallux valgus deformity.
A dorsal longitudinal incision over the first MTPJ was made, and the dorsal capsule was attenuated and excised, revealing a disintegrating Cartiva implant within the metatarsal head (Figure 4). After removal of the implant (Figure 5), the defect in the bone measured 10 × 6 mm. The cancellous bone surrounding the implant was soft and provided no structural integrity. Curettage was performed back to healthy bone. An osteochondral autograft transplant procedure was performed. 29 A central guide pin was placed in the first metatarsal shaft and a 10-mm coring reamer was used removing the remainder of corticocancellous bone in preparation for the osteochondral plug (Figure 6).

Intraoperative photograph depicting the disintegration of a Cartiva implant within the metatarsal cavity.
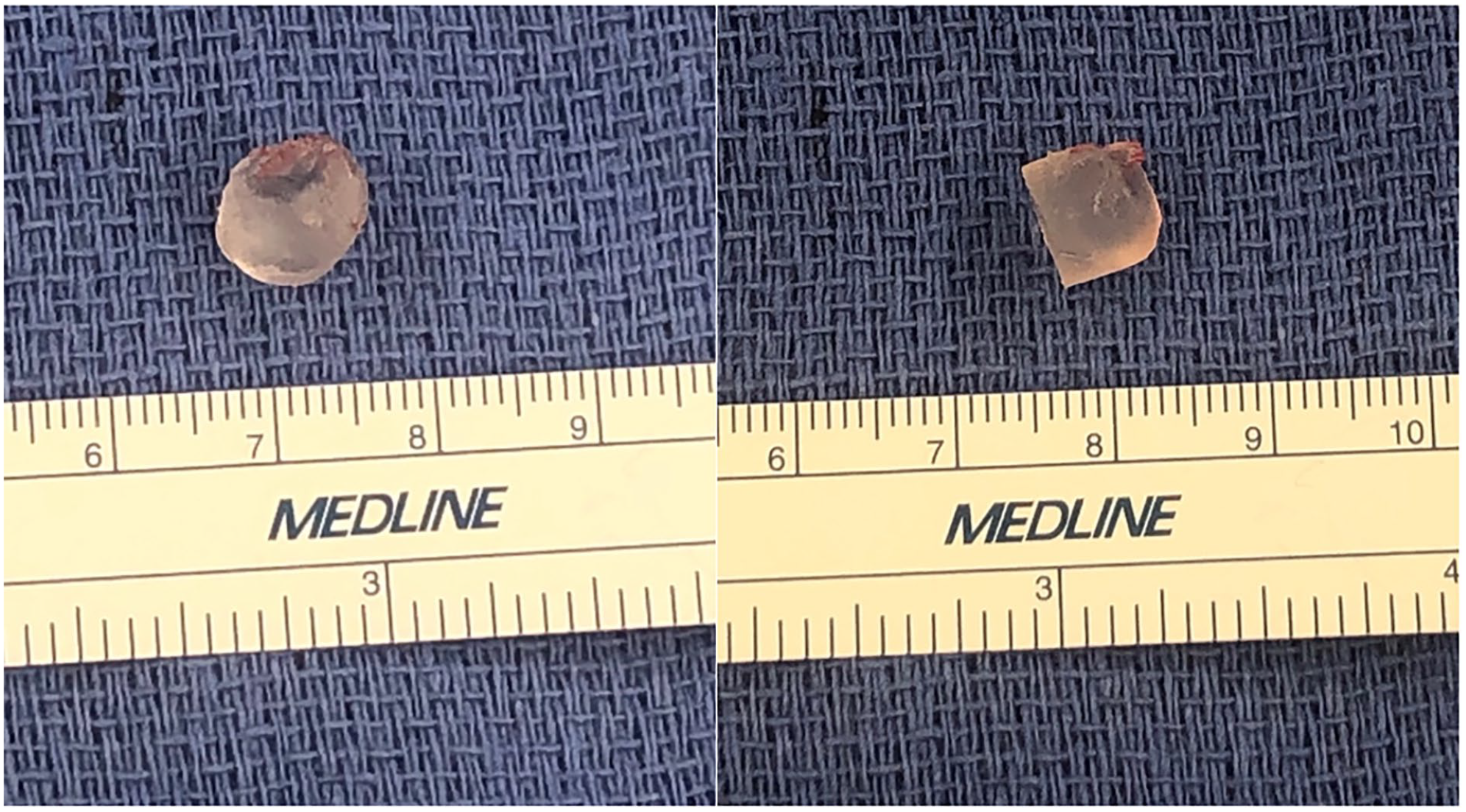
Fragmented Cartiva implant pieces extracted from the metatarsal cavity during surgery.

Intraoperative photograph demonstrating the preparation of recipient site after a guide pin and coring reamer were used in order to remove the remainder of diseased bone.
At the ipsilateral knee, as previously described by Kennedy and Murawski, 29 a small 2-cm lateral incision was made in the lateral retinaculum at the level of the articular cartilage of the lateral femoral condyle. Once the articular surface was identified, the donor site was chosen based on the articular contour that would closely match the articular contour of the metatarsal head. Using a 10-mm trephine a 10 × 18-mm osteochondral plug was harvested and immersed in bone marrow aspirate concentrate (Figure 7). The osteochondral plug was bulleted for ease of graft placement and lightly tamped into place. The final graft position restored the native cartilage surface and was stable to axial and rotational stress (Figure 8).

Intraoperative photograph of the 10 × 18-mm osteochondral plug, harvested and immersed in bone marrow aspirate concentrate.

Final graft positioned to restore the native cartilage surface, ensuring stability against axial and rotational stress, and aligning with the previous cheilectomy. (A) Dorsal and (B) Oblique view of the graft positioned in the defect, (C) Dorsal view of the graft contoured to fit the defect.
Because of significant cartilage loss on the proximal aspect of the proximal phalanx, an intraoperative decision was made to augment the procedure with interpositional arthroplasty using dermal graft. In addition, a proximal phalanx closing wedge osteotomy was performed to address the patient’s residual interphalangeal hallux valgus.
Postoperatively, the patient was placed in a tall controlled ankle motion boot for 4 weeks and was allowed to weightbear at 2 weeks postoperative. At the patient’s 4-week appointment she was transitioned to a postoperative shoe for an additional 2 weeks, and then finally transitioned to regular sneakers with a Morton extension for an additional 4 weeks.
At the 2- and 8-week follow-ups, the patient’s postoperative pain continued to improve. At her 3-month follow-up, the patient was able to return to light-impact activities and was able to return to full-impact activities at 6 months. At 3-year follow-up, the patient was completely pain free with a hallux range of motion (ROM) of 40 degrees dorsiflexion and 15 degrees of plantar flexion. Although she reports a return to normal activities, her ability for higher level function has been limited because of the development of contralateral hallux rigidus symptoms. At the 3-year follow-up, radiographs demonstrate improved joint space and complete graft incorporation (Figure 9). The patient initially experienced ipsilateral knee pain at the OATS donor site, this resolved following a cortisone injection and a course of physical therapy focused on vastus medialis obliquus (VMO) strengthening.

Radiographs, at the 3-year follow-up, demonstrating improved joint space and complete graft incorporation. (A) Lateral and (B) AP views.
Discussion
The objective of this case report was to describe a reproducible and effective surgical intervention for patients undergoing revision surgery for hallux rigidus after an unsuccessful synthetic PVA hydrogel implant, particularly in cases involving substantial bone loss, and expressing the desire to preserve motion at the first metatarsophalangeal (MTP) joint.
In 1973, Bray and Merrill initiated the exploration of synthetic implants composed of PVA for cartilage replacement. Their study focused on the compressive properties, permeabilities of PVA hydrogels, water contents, tensile properties, and pore sizes of cationic PVA hydrogels. Their research proposed that crystallized hydrogel polymers of PVA, created through electron crosslinking, were potential candidates for a synthetic articular cartilage material suitable for application in reconstructive joint surgery. 6 Maruoka et al 33 further demonstrated the biocompatibility of PVA hydrogels by injecting them into the eyes of crab-eating macaques, showing no adverse effects at 3-month follow-up.
The Cartiva implant gained prominence following a prospective, randomized, multicentered clinical trial comparing it to first metatarsophalangeal arthrodesis in advanced hallux rigidus. The trial concluded with equivalent pain relief and functional outcomes, emphasizing the benefit of preserving joint motion.2,8 Additionally, Daniels et al 14 reported positive midterm clinical outcomes with reduced visual analog scale (VAS) score at a 5-year follow-up after PVA hydrogel hemiarthroplasty of the first MTP joint in advanced hallux rigidus. Glazebrook et al 22 demonstrated an increase in the Foot and Ankle Ability Measure (FAAM) score at a 2-year follow-up, but admitted a notable hardware removal rate and conversions to arthrodesis.
Our patient, similar to other cases in the literature, underwent synthetic implant removal with significant bone loss. 17 The removal of these implants poses a significant limitation when failures occur, attributed to extensive glycosaminoglycan loss and cartilage fibrillation.5,10 Additionally, factors such as implant subsidence, rotation, and lack of integration contribute to instability.9,35,43,45 We believe implant malpositioning contributed to failure of the PVA implant in this case. Approximately 40% of the metatarsal head was resected as result of the primary and revision cheilectomy. The implant appeared to have been inserted with dorsal angulation and lacked sufficient dorsal cortical support. We suspect this allowed the implant to “flip” or rotate within the metatarsal bone. However, attempting to insert the implant more plantarly would have invaded the crista of the metatarsal head and broached the metatarsal-sesamoid articulation.
Arthrodesis continues to be regarded as the gold standard for patients facing severe hallux rigidus and remains a viable option for revisions following unsuccessful joint preservation methods.4,7,18,20,25,36,44,49 However, in this specific case, the patient made it clear that arthrodesis was not an option she wished to consider. Her desire was to return to her active lifestyle with preservation of her first MTP joint motion. Although arthrodesis may have addressed our particular patient’s pain, numerous studies have reported elevated nonunion rates especially in active patients. A recent systematic review, including 6 studies with 76 patients averaging 54.9 years old, revealed a nonunion rate of 16.5% at a 48-month follow-up. 48 The increased incidence of nonunion has prompted the development of systems specifically designed for the easier revision of failed Cartiva implants, such as the AVITRAC system (Paragon 28), Arthrex Cannulated Bone Dowel system, and First MTP Fusion with Metatarsal Head Bone Loss system (CONMED).1,12,37 Additionally, first MTP joint arthroplasty has demonstrated encouraging short-term results. A study comparing total joint replacement with arthrodesis of the first MTP joint found similar clinical outcomes at 3- and 12-month follow-ups, including patient reported outcome measure scores, Visual Analogue Scale for Foot and Ankle, and European Foot and Ankle Society scores. The final follow-up at 37 months revealed increasing scores for patients who underwent total joint replacement compared with arthrodesis. 41
In this case, the patient expressed a strong preference for preserving joint motion and explicitly rejected fusion. Several surgical strategies were considered to fill the void created by the failed implant while maintaining motion, including simple bone grafting with autograft vs allograft, structural bone plug with overlying cartilage allograft, and interpositional arthroplasty. Each of these techniques has inherent limitations, and careful selection must be made based on the specific requirements of the patient and the availability of appropriate tissue.
Metal hemiarthroplasty implants are an option for revision surgery following unsuccessful primary hallux rigidus procedures. 18 However, in the long term, complications including loosening, subsidence, and persistent pain often necessitate arthrodesis.21,40
Other options for revision surgery include joint surface preservation implants made of ceramic or silicone. However, the available literature mainly comprises small cohorts, single case reports, or short-term follow-up studies.30,46,47 Notably, there are no long-term studies on revision surgeries involving silicone or ceramic surface implants. A study on primary hallux rigidus surgery, with a 2- to 8-year follow-up using the MOJE ceramic-on-ceramic press-fit arthroplasty implant in 31 patients, reported a reoperation rate of 26% at 8 years, with 16 patients (52%) experiencing device loosening. 15
Interpositional arthroplasty where a biologic spacer is introduced between the 2 bone surfaces can preserve first MTPJ range of motion and minimize the need for bone resection.3,26 The biologic spacer can be an autograft, typically using the dorsal capsule and extensor hallucis brevis (EHB), or an allograft composed of acellular matrix or cadaveric tendon.3,26,28,32 In a retrospective review of 19 patients who had previously failed joint preservation techniques for hallux rigidus, tibialis anterior allograft tendon interpositional arthroplasty of the first MTP joint was performed. 50 The average American Orthopaedic Foot & Ankle Society (AOFAS) score for all patients was 68.5 preoperatively and 74.1 postoperatively at the final follow-up (16 months), demonstrating an increase in joint space radiographically. A case involving a failed metal hemi-cap implant with a previous Keller resection underwent interpositional arthroplasty under the care of the senior author with pain-free motion achieved at the 12-month follow-up.
To our knowledge there is only one other case report in the literature using osteochondral autograft as a revision procedure in the setting of hallux rigidus to revise a failed metal hemi-cap implant. 27 By the 6-month follow-up, their patient was pain-free and able to walk more than 15 miles per week. At the 1-year mark, the patient was discharged with no symptoms or signs of hallux rigidus. 27 Title et al 51 reported an osteochondral autograft technique for hallux rigidus without a prior cheilectomy in which they obtained a donor plug from the dorsal aspect of the same metatarsal head, followed by a standard cheilectomy. However, the previous dorsal cheilectomy in our patient prevented this option. Consequently, the senior author opted for an autologous osteochondral graft from the nonweightbearing femoral condyle, using the technique for talus osteochondral lesions. 29 This approach ensured that we could obtain a graft of appropriate size and contour with excellent integration potential, critical in this revision setting.
Although our surgical plan was to perform an isolated osteochondral autograft procedure to address the cartilage defect in the metatarsal head, the extensive cartilage loss identified at the base of the articulating phalanx determined intraoperatively necessitated augmentation with interpositional arthroplasty using dermal allograft. This option had been discussed with the patient preoperatively. Although an osteochondral autograft or interpositional arthroplasty (combined with bone grafting of the metatarsal defect) may have been sufficient in the short term, we hope the combined approach will provide a longer-term successful outcome in our young female patient. Nevertheless, we appreciate that it is not possible to separate the contributions of each technique to the final outcome at this early stage.
Conclusion
This study highlights the intricate challenges and complexities inherent in managing hallux rigidus, particularly in the revision setting. The presented case of a 43-year-old woman who underwent multiple interventions sheds light on the limitations of synthetic cartilage implants and underscores the urgent need for alternative solutions. Our patient’s experience highlights the balancing act between symptom relief and preserving joint function.
The patient’s reluctance toward joint fusion, a traditional approach with its own limitations, led us to explore diverse alternatives. The use of an ipsilateral knee osteochondral autograft bone plug, combined with interpositional arthroplasty, exemplifies a nuanced and patient-specific surgical innovation. It is not possible to separate the contributions of each technique to the final outcome. However, given the extensive joint destruction, we are hopeful the combined technique will maximize the chances of a positive long-term result. This approach not only addressed the specific case complexities but also contributes to the broader discourse on hallux rigidus revision surgeries.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251330300 – Supplemental material for Revision Surgery for Failed Polyvinyl Alcohol Hydrogel Implant in the First MTP Joint: A Case Report and Comprehensive Review
Supplemental material, sj-pdf-1-fao-10.1177_24730114251330300 for Revision Surgery for Failed Polyvinyl Alcohol Hydrogel Implant in the First MTP Joint: A Case Report and Comprehensive Review by Thelma R. Jimenez Mosquea, Christopher A. Colasanti, Hugo A. Ubillus and Raymond J. Walls in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.