
Abstract
Background:
Hallux rigidus is a common arthritic condition that has been addressed surgically with a range of techniques, from an isolated cheilectomy to first metatarsophalangeal (MTP) joint fusion. Recently, hemiarthroplasty with polyvinyl alcohol (PVA) hydrogel implant has been used as an alternative treatment to relieve pain while preserving motion of the first MTP joint. We retrospectively reviewed patient-reported outcome scores and clinical outcomes for patients treated for hallux rigidus with PVA hydrogel implant at an academic, multisurgeon center.
Methods:
A total of 103 patients who underwent first MTP hemiarthroplasty with PVA hydrogel implant between January 2017 and October 2018 were retrospectively reviewed (average, 26.2 months). Eight surgeons were represented. Baseline Patient-Reported Outcomes Measurement Information System (PROMIS) scores for the Physical Function, Pain Interference, Pain Intensity, Global Physical Health, Global Mental Health, and Depression domains were collected prospectively and compared with PROMIS scores collected at a minimum of 1 year postoperatively (average, 13.9 months). Seventy-three patients had both preoperative and postoperative scores. Ten of these patients had undergone a prior procedure of the first MTP, and 52 underwent concurrent Moberg osteotomy at the time of PVA hydrogel implantation.
Results:
For patients with baseline and postoperative PROMIS scores, significant pre- to postoperative improvement was detected for the Physical Function, Pain Interference, Pain Intensity, and Global Physical Health domains (P < .05). Patients who had undergone a prior procedure of the first MTP had significantly higher postoperative Pain Intensity scores compared with those who did not undergo a prior procedure. Patients undergoing concurrent Moberg osteotomy had significantly lower postoperative Pain Interference and Pain Intensity scores compared with those who did not undergo a Moberg. Two patients underwent revision procedures in the first 2 years postoperatively, one with revision hemiarthroplasty and one with conversion to arthrodesis.
Conclusion:
On average across our entire cohort, physical function and pain scores improved significantly pre- to postoperatively; however, postoperative pain scores were significantly higher for patients who had undergone a prior procedure of the first MTP and significantly lower for patients who underwent concurrent Moberg osteotomy. The implant displayed excellent survivorship in the first 2 years postoperatively, with only 2 revision procedures.
Level of Evidence:
Level III, comparative series.
Keywords
Introduction
Hallux rigidus is characterized by degenerative arthritis of the first metatarsophalangeal (MTP) joint. It affects 2.5% of people over 50 years of age in the United States, making it the most prevalent type of foot arthritis. 11 Standard treatment varies depending on the severity of symptoms, which include pain and decreased range of motion. Nonoperative treatment includes activity modification, footwear modification, and orthotics designed to limit motion at the MTP joint. 11 Nonsteroidal anti-inflammatory drugs (NSAIDs) and steroid injections can also be used to reduce pain. 11 Collectively, these nonoperative methods may successfully provide relief for about half of all hallux rigidus patients according to 1 retrospective study. 9 Cases that fail to improve with nonoperative management often require operative intervention, with a range of methods used depending on the severity of symptoms.
Most often in grade II and III hallux rigidus, a standard cheilectomy has been used to improve dorsiflexion movement and reduce pain while preserving the MTP joint. 13 Generally, however, cheilectomy is most effective for less severe cases of hallux rigidus, and subsequent procedures may be required in certain cases. Particularly for patients presenting with more severe hallux rigidus, standard cheilectomy has been shown to result in persistent symptoms for about 10% to 15% of patients at intermediate- to long-term follow-up.5,6 Further, failure rates for an isolated cheilectomy have been reported as high as 37.5% for patients with grade III hallux rigidus. 10 O’Malley et al 13 have reported favorable clinical and patient-reported outcomes for grade III hallux rigidus patients following cheilectomy with the addition of a Moberg osteotomy. The Moberg osteotomy has been found to increase dorsiflexion and shift the center of pressure on the proximal phalanx more plantarly.12,13 Cheilectomy with Moberg osteotomy is routinely used at our institution as a joint-preserving procedure to address hallux ridigus.
As an alternative to standard joint-preserving procedures, a synthetic cartilage implant (SCI) (Cartiva Inc, Alpharetta, GA) was approved by the US Food and Drug Administration (FDA) in 2016 for use in hemiarthroplasty of the first MTP joint. The goal of this polyvinyl alcohol (PVA) implant is to provide pain relief while maintaining motion of the joint. A randomized clinical trial sponsored by the manufacturer of the implant showed equivalent pain relief and functional outcome scores at 2-year follow-up when comparing patients undergoing hemiarthroplasty with patients undergoing first MTP fusion. 3 However, a recent non–industry- sponsored study demonstrated less promising results with this implant. These authors report that 33 out of 64 patients (52%) in their cohort required therapeutic steroid injection at an average of 7.6 months after initial implantation, and 13 out of 64 (20%) required reoperation at an average of 12.3 months postoperatively. Subsequent procedures included implant removal and conversion to arthrodesis for 5 out of 64 patients (8%). 4 In addition to relatively high rates of complication and revision surgery, these authors present validated Patient-Reported Outcomes Measurement Information System (PROMIS) scores for the Pain Interference and Physical Function domains, as well as patient satisfaction measures. For their cohort of 60 patients with 64 implants, mild pain symptoms, mild physical dysfunction, and neutral levels of satisfaction were reported. 4 However, PROMIS scores were not collected preoperatively, so postoperative scores could not be compared with baseline scores.
The current study aimed to evaluate outcomes following first MTP hemiarthroplasty with PVA hydrogel implant at an academic, multisurgeon center. In addition to retrospective review of clinical outcomes, we prospectively collected baseline PROMIS scores through our institution’s foot and ankle registry and compared them with scores collected postoperatively. We performed a subgroup analysis to evaluate outcomes for patients undergoing prior procedure of the first MTP compared with patients who did not undergo a prior procedure. We also compared outcomes for patients undergoing concurrent Moberg osteotomy versus those who did not undergo a Moberg. We hypothesized that outcomes would generally improve and would not be affected by prior procedures, but that patients undergoing a concurrent Moberg osteotomy would report significantly better outcomes compared with those who did not undergo a Moberg.
Methods
Approval was obtained from the institutional review board steering committee, which oversees our institution’s foot and ankle registry. One hundred three hallux rigidus patients who underwent first MTP hemiarthroplasty with PVA hydrogel implant between January 2017 and October 2018 were identified. Patients treated with or without concurrent Moberg osteotomy were eligible for inclusion. Patients undergoing PVA hydrogel implant for a condition other than hallux rigidus were excluded. Eight fellowship-trained orthopedic foot and ankle surgeons at a single academic institution were represented.
Study Population and Design
Retrospective chart review was performed to assess for prior procedures, operative procedure performed, postoperative events, and clinical outcomes. Demographic data including age at time of surgery, gender, and body mass index (BMI) were also collected. The average age of this cohort was 57.7 (range, 26-76) years, and 74 out of 103 patients (71.84%) were female. The average BMI was 25.9 (range, 18.2-42.3) kg/m2. The average time to clinical follow-up was 26.2 (range, 14-36) months.
Baseline PROMIS scores for the Physical Function, Pain Interference, Pain Intensity, Global Physical Health, Global Mental Health, and Depression domains were collected prospectively through our institution’s foot and ankle registry. These same PROMIS domains were administered at 1 and 2 years postoperatively, when applicable. Of the 103 total patients, 90 (87.4%) had baseline PROMIS scores, and 73 out of 90 (81%) had minimum 1-year postoperative scores. For patients with postoperative PROMIS scores, the average time to the follow-up survey was 13.9 (range, 12-25) months.
Of the 73 patients with baseline and postoperative PROMIS scores, 10 patients (14%) had undergone a prior procedure of the first MTP. Four patients had prior cheilectomy with or without Moberg osteotomy, 4 had double metatarsal osteotomy (DMO) with or without Akin osteotomy, and 1 had prior hemiarthroplasty (Table 1). Fifty-two of the 73 patients (71%) underwent concurrent Moberg osteotomy at the time of PVA hydrogel implantation based on surgeon evaluation of the joint. In patients undergoing Moberg osteotomy, cheilectomy was also performed but only involved approximately 10% of the dorsal aspect of the metatarsal. This removed the dorsal osteophyte but still allowed for ample dorsal coverage of the PVA implant.
List of Patients Undergoing a Prior Procedure of the First MTP (10 of 73 Total Patients With PROMIS Scores).
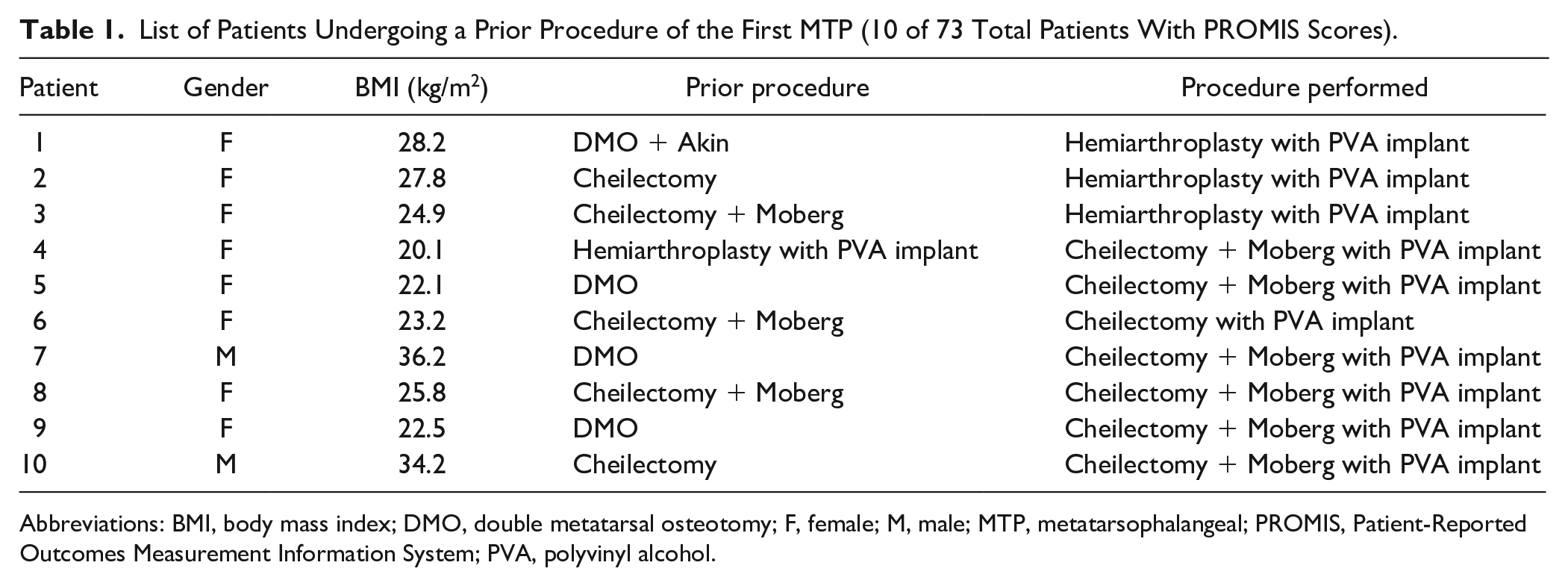
Abbreviations: BMI, body mass index; DMO, double metatarsal osteotomy; F, female; M, male; MTP, metatarsophalangeal; PROMIS, Patient-Reported Outcomes Measurement Information System; PVA, polyvinyl alcohol.
Statistical Analysis
Patient PROMIS scores were analyzed using Student t tests. Preoperative and postoperative scores were compared for the full cohort. Subgroup analyses were performed using t tests to evaluate differences in preoperative scores, postoperative scores, or pre- to postoperative change. Statistical significance was evaluated at
Surgical Technique and Postoperative Protocol
The first MTP joint was accessed through a straight dorsal incision and osteophytes were then removed with a rongeur or a saw blade to limit impingement while also ensuring that a sufficient amount of intact cortical rim remained. This usually involved approximately 10% of the metatarsal head. If a Moberg osteotomy was performed, a 2- to 3-mm wedge of dorsal bone of the proximal phalanx was removed and secured with a 7 × 9–mm staple or 2-mm screw, depending on surgeon preference. An oscillating rasp was used to contour the metatarsal head and the proximal phalanx to ensure that no sharp edges remained.
The implant was placed per manufacturer guidelines. A 10-mm implant was utilized in 66 patients, and an 8-mm implant in 7 patients (Figure 1). The PVA implant was placed into the implant delivery system and seated in the metatarsal head protruding 2 mm above the metatarsal head (Figure 1). A layered closure was then completed. A soft dressing with postoperative shoe or splint was applied. Patients were allowed to immediately bear weight or were limited for the first 2 weeks to allow the incision to heal. Sutures were removed 2 to 3 weeks postoperatively and patients were transitioned into regular shoe wear.
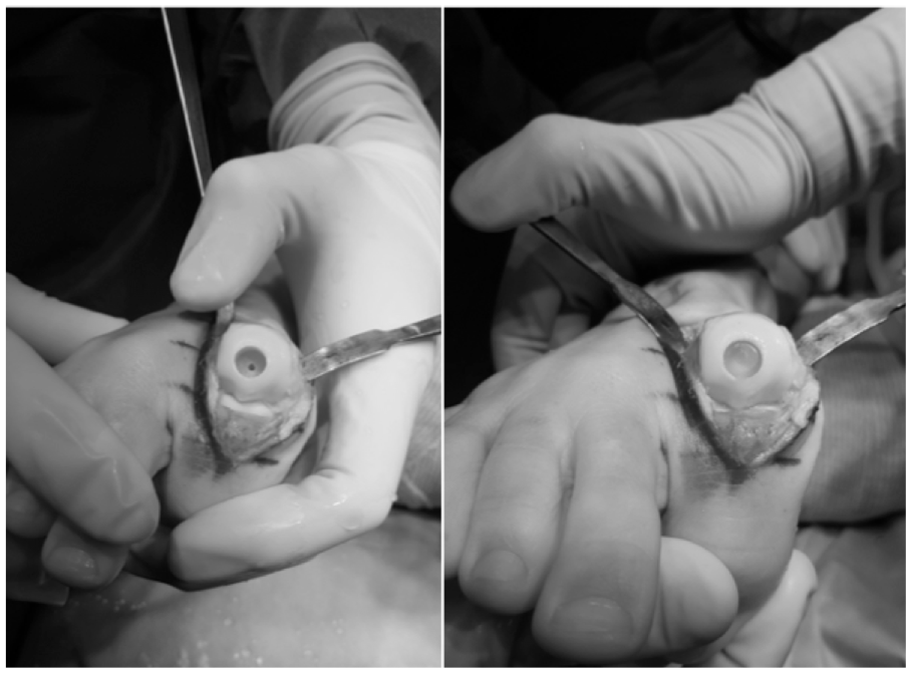
Intraoperative images show the placement of the polyvinyl alcohol hydrogel implant.
Results
Patient-Reported Outcomes
For the 73 patients with both baseline and postoperative PROMIS scores, the mean baseline PROMIS scores demonstrated mild functional impairment and pain interference and normal ranges for the Pain Intensity, Global Physical Health, Global Mental Health, and Depression domains (Table 2). Mean postoperative scores demonstrated statistically significant (P < .05) improvement across all PROMIS domains except Global Mental Health (P = .50) and Depression (P = .63). At postoperative follow-up, the average scores for all PROMIS domains were within normal ranges (Table 2).
Baseline and Postoperative PROMIS Scores for All 73 Patients With Pre- and Postoperative PROMIS Surveys. a
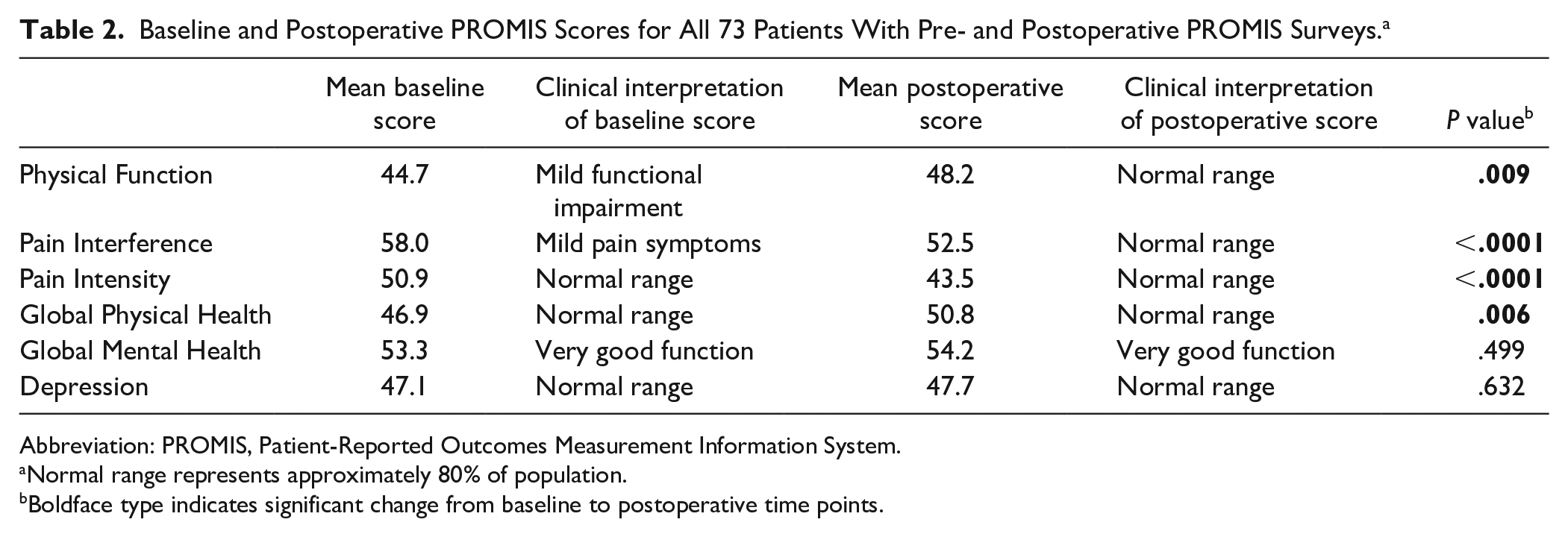
Abbreviation: PROMIS, Patient-Reported Outcomes Measurement Information System.
Normal range represents approximately 80% of population.
Boldface type indicates significant change from baseline to postoperative time points.
Subgroup analysis was performed to compare outcomes for the 10 patients who had undergone a prior procedure of the first MTP with the 63 patients who did not undergo a prior procedure. Patients undergoing prior procedures presented at our institution with significantly lower Physical Function scores (average, 39.8 vs 45.5; P = .03) and significantly higher Depression scores (average, 51.6 vs 46.4; P = .02).
Postoperatively, patients undergoing a prior procedure had higher Pain Intensity scores compared with patients who did not undergo a prior procedure (average, 49.9 vs 42.5; P = .01). The pre- to postoperative change in Pain Intensity scores was also statistically significant, with an average decrease of 2.5 points for the prior procedure group and an average decrease of 8.7 points for those without a prior procedure (P = .05). Patients undergoing a prior procedure had significantly lower postoperative Physical Function scores (average, 42.5 vs 49.1; P = .02), though they also had lower baseline Physical Function scores. The pre- to postoperative change in Physical Function scores was not statistically significant (P = .71) (Table 3).
Prior Procedure Versus No Prior Procedure PROMIS Comparison.
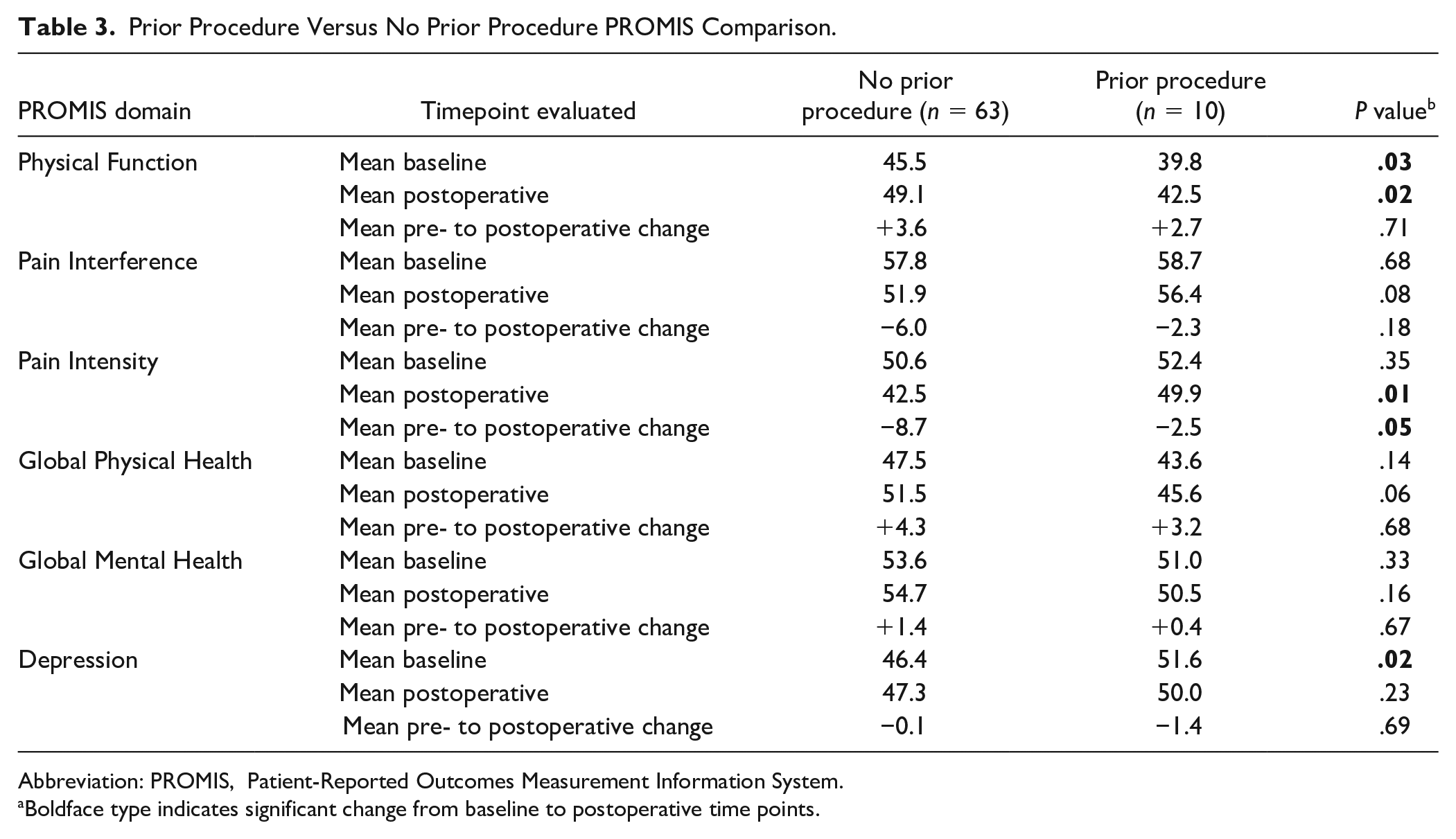
Abbreviation: PROMIS, Patient-Reported Outcomes Measurement Information System.
Boldface type indicates significant change from baseline to postoperative time points.
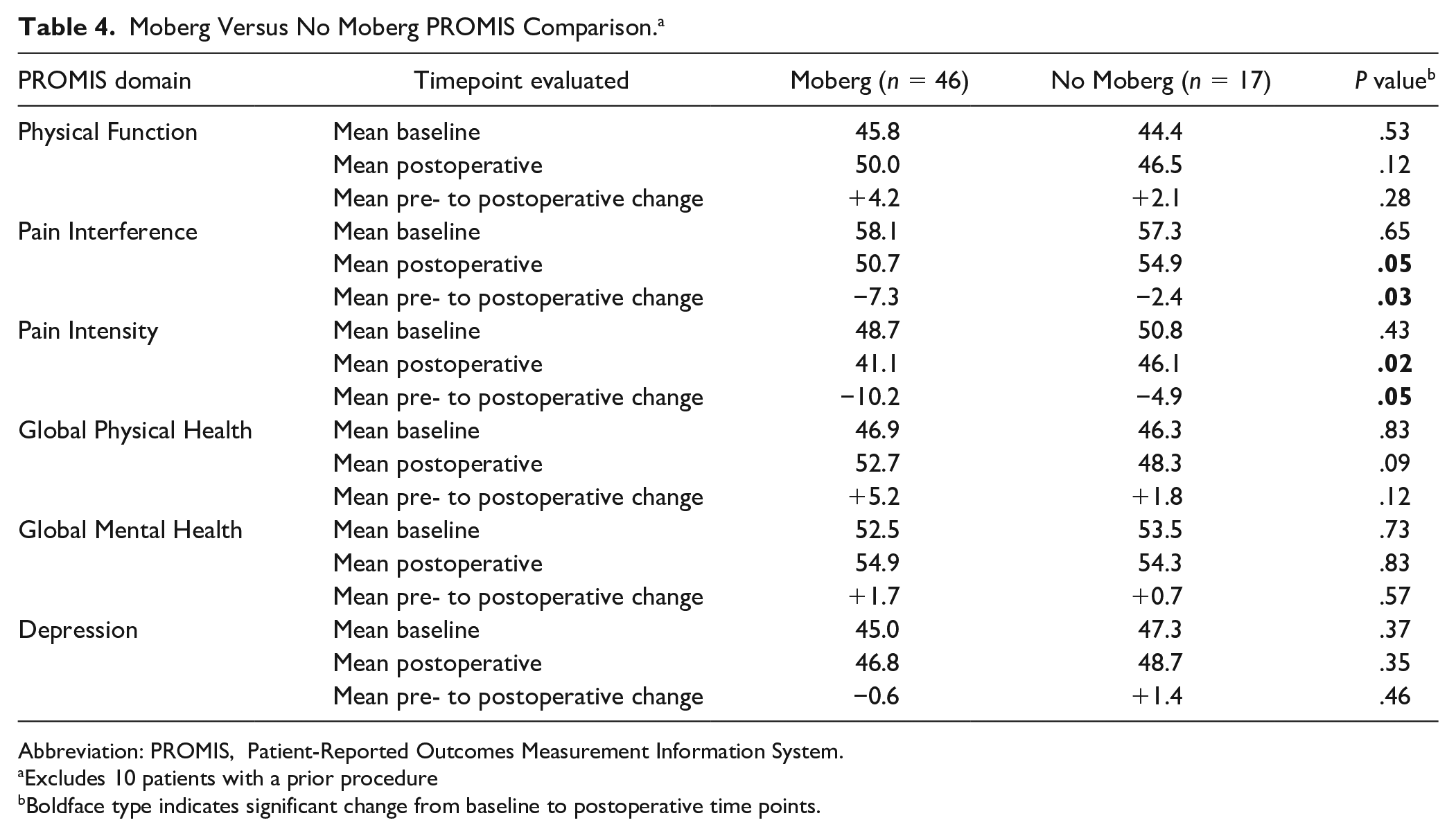
Subgroup analysis was also performed to compare outcomes for patients who underwent concurrent Moberg osteotomy with those who did not. Because the patients undergoing prior procedures demonstrated significantly different baseline and postoperative PROMIS scores for certain PROMIS domains when compared with the patients who did not undergo a prior procedure, the 10 patients who had a prior procedure were excluded from the Moberg subgroup analysis. Of the 63 remaining patients, 46 had cheilectomy with Moberg osteotomy, while 17 had cheilectomy only or first MT resurfacing at the time of PVA hydrogel implantation. There were no significant differences in preoperative PROMIS scores between groups. Postoperatively, Moberg patients demonstrated significantly lower Pain Interference (50.7 vs 54.9; P = .05) and lower Pain Intensity (41.1 vs 46.1; P = .02) scores. Pre- to postoperative improvements in Pain Interference (−7.3 vs −2.4; P = .03) and Pain Intensity (−10.2 vs −4.9; P = .05) were also significantly greater for Moberg patients (Table 4).
Moberg Versus No Moberg PROMIS Comparison. a
Abbreviation: PROMIS, Patient-Reported Outcomes Measurement Information System.
Excludes 10 patients with a prior procedure
Boldface type indicates significant change from baseline to postoperative time points.
Clinical Outcomes
Two out of 103 total patients (1.9%) with clinical follow-up underwent revision surgery within 2 years of implant placement after experiencing persistent pain. Neither patient had prior surgery of the first MTP before presenting at our institution. Both patients underwent cheilectomy with Moberg osteotomy and PVA hydrogel implantation in their initial procedures. The first revision was a conversion to arthrodesis performed at 14 months after initial PVA implantation (Figure 2). In the revision procedure, the implant was noted to be loose, with inflammation and fibrous tissue at the MTP joint level. The second revision occurred 21 months postoperatively, and a revision hemiarthroplasty with PVA implant was performed. In this revision procedure, the implant was found to have marked loss of contour at the medial aspect of the toe. Before undergoing PVA hydrogel implantation, both revision patients reported higher baseline Physical Function (52.6 and 49.8) and lower baseline Pain Interference (50.1 and 51.9) scores compared with the cohort averages of 44.7 and 58.0, respectively. One year after the initial procedure, both patients reported higher Pain Interference (64.2 and 53.9) and Pain Intensity (56.3 and 49.9) scores compared with the postoperative cohort averages of 52.5 and 43.5, respectively.

Sixty-three-year-old female undergoing initial polyvinyl alcohol hydrogel implantation in December 2017 with conversion to arthrodesis 14 months postoperatively. Images shown (left to right) are preoperative, 2 weeks following polyvinyl alcohol implantation with Moberg osteotomy, and 1 month following first metatarsophalangeal arthrodesis.
Of the 103 patients with clinical follow-up, 6 (5.8%) underwent therapeutic steroid injection between 2 and 11 months postoperatively. Three patients requiring injection had a prior procedure of the first MTP, 2 of whom underwent concurrent Moberg osteotomy in the procedure performed at our institution. The remaining 3 patients undergoing injection had no prior procedure and underwent concurrent Moberg osteotomy. Six patients (5.8%) were prescribed symptom-specific orthotics between 3 and 6 months. One of these patients had a prior procedure and underwent concurrent Moberg at our institution. Two of the remaining 5 patients requiring symptom-specific orthotics had a Moberg osteotomy. Magnetic resonance imaging (MRI) scans performed on 22 out of 103 total patients (21.4%) with persistent postoperative pain showed persistent edema surrounding the implant (Figure 3), and included the 2 patients who underwent a revision procedure. One patient sustained an intraoperative metatarsal fracture during application of the implant, which was addressed at the time with open reduction and internal fixation (ORIF). Minor, nonsurgical wound complications were observed in 3 patients (2.9%). Two patients (1.9%) underwent the same procedure with PVA hydrogel implant on the contralateral side within 1 year of the initial surgery.
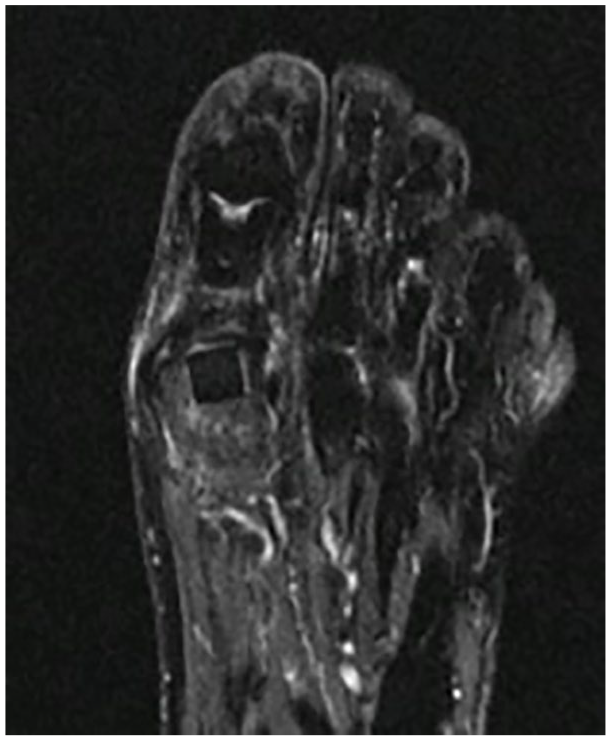
Postoperative magnetic resonance imaging performed 6 months after polyvinyl alcohol hydrogel implantation showing persistent edema in the first metatarsal head.
Discussion
To our knowledge, this study represents the largest cohort of patients undergoing PVA hydrogel implantation with both baseline and minimum 1-year PROMIS scores. The demographics of this cohort are comparable to those described in the existing literature with regard to age, gender, and BMI.3,4 Our cohort differs from others used in evaluating the PVA hydrogel implant because 52 of 73 patients in our cohort underwent concurrent Moberg osteotomy. At the discretion of each surgeon, a Moberg was added to increase dorsiflexion and shift pressures plantarly, which is a technique that has been described by O’Malley et al 13 and was reported to improve clinical and patient-reported outcomes. Our results are consistent with those previously reported, as patients who underwent concurrent Moberg osteotomy experienced significantly greater pain relief compared with those who did not undergo an additional Moberg. Though our cohort differs from the original clinical trial cohort in that we frequently added a Moberg osteotomy when placing the PVA hydrogel implant, this study adds to the limited literature evaluating the PVA implant outside of the cohort used for the initial clinical trial.
Cassinelli et al 4 presented the first study evaluating the PVA hydrogel implant outside of industry-sponsored studies. 1 They evaluated a cohort of 60 patients (64 implants), with 40 postoperative PROMIS Pain Interference scores, 42 postoperative PROMIS Physical Function scores, and 64 patient satisfaction responses. These authors report only descriptive statistics, with no baseline PROMIS scores to compare postoperative scores. A strength of the present study is that the analysis of PROMIS scores utilizes preoperative scores, collected through a prospective registry at our institution. For our full cohort of 73 patients, our findings show significant improvement in the Physical Function, Pain Interference, Pain Intensity, and Global Physical Health domains from baseline to postoperative time points. Cassinelli et al 4 reported an average postoperative Pain Interference score of 60 (n = 40) and Physical Function score of 42 (n = 42) at 15 months of follow-up. Our average postoperative scores for these same PROMIS domains show substantially lower Pain Interference (53.2) and higher Physical Function (47.7), with 73 responses in each domain and an average survey follow-up of 13.9 months.
With an average clinical follow-up of 12.5 months, Cassinelli et al 4 reported therapeutic injections for 33 out of 64 joints (52%), reoperation for 13 out of 64 joints (20%), and conversion to arthrodesis for 5 out of 64 joints (8%). A recent study by An et al 1 evaluated 18 symptomatic implants from this cohort using MRI. We observed similar patterns of edema in the first metatarsal for patients with persistent postoperative pain who underwent MRI, which included 22 out of 103 patients (21.4%). However, with an average clinical follow-up of 26.2 months, we observed subsequent intervention in only 8 out of 103 patients (7.7%), with therapeutic injections in 6 patients (5.8%) and revisions in 2 patients (1.9%), including 1 conversion to arthrodesis (0.97%). Our revision rate is also lower than the rate reported for the initial clinical trial cohort undergoing hemiarthroplasty with PVA implant, where 17 of 152 patients (11.2%) underwent subsequent procedures and 14 of 152 cases (9.2%) were converted to arthrodesis about 1 year after implantation on average (average, 390 days). 3 The minimum follow-up for the clinical trial cohort was 2 years.
The primary patient-reported outcomes in the initial clinical trial for the PVA hydrogel implant were the Foot and Ankle Ability Measure (FAAM) sports and activities of daily living scores, and the visual analog scale (VAS). 3 Because we did not administer FAAM or VAS surveys, we are unable to compare outcomes directly. However, significant improvement in postoperative VAS pain scores and FAAM sports and activities of daily living scores was reported for clinical trial patients who received the PVA implant, 3 and we similarly observed significant pain relief and increase in physical function based on PROMIS scores. However, we also observed variation in PROMIS scores in our subgroup analyses, suggesting that different factors may contribute to the success of a PVA implant procedure.
Ten patients in our cohort had prior procedures before undergoing their first MTP hemiarthroplasty at our institution. Prior procedures represented included cheilectomy with or without Moberg osteotomy, DMO with or without Akin osteotomy, and prior hemiarthroplasty. These patients presented with significantly worse Physical Function and Depression scores. They also demonstrated a significantly smaller decrease in Pain Intensity scores when compared with patients who did not undergo a prior procedure. Though the number of patients with prior procedures is relatively small and we can therefore only draw a limited conclusion, our results suggest that prior procedure of the first MTP may affect the success of a subsequent hemiarthroplasty procedure. This result is consistent with the contraindications utilized for the initial clinical trial, where previous cheilectomy resulting in inadequate bone stock was a criterion for exclusion. 3
Because we observed significant differences in PROMIS scores between the patients who had undergone a prior procedure and those who did not, we excluded the 10 who had undergone a prior procedure when evaluating the effect of the additional Moberg osteotomy. Of the 63 remaining patients, 46 patients underwent concurrent Moberg osteotomies at the time of PVA hydrogel implantation, while 17 did not. We observed significantly lower postoperative Pain Interference and Pain Intensity scores for the Moberg patients, as well as significantly greater pre- to postoperative improvements in those domains. Though the analysis is limited to only 17 patients who did not have a Moberg osteotomy, this finding corroborates previously published results that suggest improved outcomes with the addition of a Moberg osteotomy in the surgical management of hallux rigidus. 13
There are several limitations of this study. Of the 103 patients undergoing PVA hydrogel implantation at our institution between January 2017 and October 2018, 13 were missing baseline PROMIS scores. Another 17 patients were missing postoperative PROMIS scores. However, clinical follow-up was available on all 103 patients. In addition to patient-reported outcomes, other studies have also evaluated range of motion or radiographic outcomes, which were not evaluated in our study.2,4 Our cohort was also not subdivided by grade of hallux rigidus, though indication for operative intervention with PVA implant at our institution typically includes patients with grade II or grade III hallux rigidus based on the Coughlin scale. 5 A prior study assessing hemiarthroplasty with PVA hydrogel implant based on hallux rigidus grade showed that the implant can be used successfully for patients with grade II, III, or IV hallux rigidus. 8 The nature of this multisurgeon cohort also introduces the potential for variations in surgical technique, which could influence patient outcomes. However, the representation of 8 surgeons may allow for more generalizable conclusions about the utility of the implant, without the influence of 1 specific surgical technique. Finally, a future randomized controlled trial to test the efficacy of an additional Moberg osteotomy to PVA implantation more rigorously is warranted.
With an average survey follow-up of 13.8 months and average clinical follow-up of 26.2 months, patient outcomes must be followed for a longer period of time to evaluate long-term outcomes, including survivorship of the implant. A follow-up study using patients from the original clinical trial cohort at a minimum of 5 years postoperatively demonstrated that the reduction in pain and symptoms seen in the first 2 years was maintained at midterm follow-up. 7 However, the study showed that an additional 9 out of 119 patients (7.6%) underwent conversion to arthrodesis between 2 and 5 years. 7 This suggests that longer-term follow-up may reveal more limitations with respect to the PVA hydrogel implant. Lastly, this study lacks a control group, which would allow for comparison of outcomes following PVA hydrogel implantation to those following standard joint-preserving procedures, such as cheilectomy with or without additional osteotomy. Particularly because our results demonstrated that patients receiving a Moberg osteotomy had better postoperative pain outcomes than those who did not, such studies would allow for comparison of outcomes between similar procedures with and without the addition of the PVA implant.
Conclusion
In general, treatment of hallux rigidus with PVA hydrogel implant appears to provide improved function and pain outcomes as assessed through PROMIS scores at a minimum of 1 year postoperatively. The implant displayed excellent survivorship at the 2-year time point, with only 2 patients undergoing revision in the first 2 years after initial implantation. The success of a PVA implant procedure appears to be influenced by prior and concurrent procedures. Patients who undergo a prior procedure of the first MTP may experience more severe pain symptoms following hemiarthroplasty with PVA implant, while the addition of a concurrent Moberg osteotomy at the time of implantation appears to improve postoperative pain interference and pain intensity.
Supplemental Material
FAI932526_disclosures – Supplemental material for Clinical Outcomes of the Polyvinyl Alcohol (PVA) Hydrogel Implant for Hallux Rigidus
Supplemental material, FAI932526_disclosures for Clinical Outcomes of the Polyvinyl Alcohol (PVA) Hydrogel Implant for Hallux Rigidus by Stephanie K. Eble, Oliver B. Hansen, Bopha Chrea, Taylor N. Cabe, Jonathan Garfinkel and Mark C. Drakos in Foot & Ankle International
Footnotes
Acknowledgements
We would like to acknowledge Megan Chapter, DO, for her contributions to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.