
Abstract
Background:
The treatment of chronic ankle sprains has largely focused on lateral ankle instability in the literature. There is a scarcity of data regarding the diagnosis and management of chronic medial ankle instability secondary to deltoid ligament injury.
Methods:
A literature search was performed using the National Center for Biotechnology Information (NCBI) database for studies evaluating chronic ankle instability (CAI) involving deltoid ligament pathology. Studies were evaluated for workup including clinical presentation, imaging, treatment algorithm and operative techniques. Descriptive statistical analysis was conducted across the pooled data set.
Results:
Nine studies representing 516 patients with CAI were included in our analysis. Plain radiographs assessed talar-tilt angle in 440 patients (85%) and anterior displacement in 296 patients (57%). A total of 465 patients underwent magnetic resonance imaging, with deltoid injuries identified in 289 (62%) of patients. Of these 289 patients, superficial deltoid involvement was specified in 61 patients and deep deltoid in 146 patients. Surgical treatment most commonly included arthroscopy in 255 patients with open deltoid ligament repair in 199 patients. Repair method included suture anchors in 173 patients (87%), bone tunnels in 23 patients (12%), and unspecified technique in 3 patients (1.5%). Thirteen patients (6.5%) had suture anchor repairs augmented with an internal brace. Three patients underwent deltoid reconstruction with plantaris tendon autograft.
Conclusion:
Deltoid ligament injuries are common in patients with CAI. These data improve our understanding of chronic deltoid injuries and can help patients and surgeons better comprehend the pathoanatomy of chronic ankle instability.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
The deltoid ligament is a complex structure that is pivotal in medial ankle stability by preventing valgus tilt and axial rotation of the talus.4,17,21 It is divided into deep and superficial layers, each composed of multiple bands. 6 The superficial deltoid stabilizes the medial tibiotalar, subtalar, and talonavicular joints. The deep deltoid is made up of the deep anterior tibiotalar and the larger deep posterior tibiotalar ligaments, crossing only the ankle joint.6,8,15
Deltoid pathology can be due to acute trauma or secondary to chronic strain. In acute trauma, the deltoid ligament is often injured secondary to supination external rotational forces, commonly seen in ankle fractures24,26 as well as up to 15% of acute inversion ankle sprains. 13
Pathology of the deltoid ligament can also be secondary to chronic lateral ankle instability. Attenuation of the deltoid ligament leads to coronal and sagittal ankle instability, further increasing stress on the superficial deltoid. 14 Individuals will often present with pain localized at the anteromedial ankle and medial gutter, as well as sensation of medial laxity. 27
Magnetic resonance imaging (MRI) and ankle arthroscopy can be used to supplement diagnosis with high specificity and ability to confirm insufficiencies to the deltoid ligament as well as osteochondral lesions. 10 However, there is little published work outlining surgical technique and long-term outcomes.
Moreover, there remains a gap in knowledge between acute and chronic deltoid pathologies in patients without evidence of posterior tibialis tendon insufficiency. The nuanced complexities of chronic injury and medial instability, and the role it plays in the progression of ankle arthritis, warrant further investigation.23,27 We sought to analyze the current available data and provide an outline on the clinical diagnosis, relevance, and utility of preoperative plain radiographs and advanced imaging, and surgical management of chronic deltoid injury to better understand pathology and treatment options.
Methods
A systematic review was performed using PubMed database evaluating studies published between 1994 and 2023 that evaluated the workup and management of chronic deltoid injuries. The following search terms were used: (“deltoid” OR “deltoid ligament” OR “medial” OR “medial ligament” OR “avulsion” OR “avulsion fracture”) AND (“ankle”). Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed.
Studies were included if they discussed injuries involving the deltoid ligament present for greater than 6 months, in the English language, with full-text availability. Exclusion criteria included studies that focused on nonhuman models, systematic reviews, meta-analyses, commentaries, editorial pieces, case reports, acute deltoid injury, and patients with chronic deltoid pathology due to posterior tibialis tendon insufficiency. Each study’s references were evaluated for further studies to include.
The evaluation process was performed by 2 independent authors, with disagreements reconciled by a third reviewer filtering by title, abstract, and then full-text review. After full-text article review, data were extracted for qualitative analyses. Data were compiled for each particular objective. Each article was evaluated for methodologic quality using the Methodological Index for Non-randomized Studies. Our objectives were to define (1) clinical presentation of the study population, (2) preoperative examination and imaging methods for assessment of deltoid ligament injuries, and (3) the treatment options and reported outcomes for study population. We have summarized our data detailing examination, plain radiographs, and MRI findings in Table 1.
Summary of Included Studies (N = 9).

Abbreviations: MRI, magnetic resonance imaging; N/A, not available.
Results
A total of 903 articles were identified to be reviewed and of these 9 met the final inclusion criteria after the final full article review (Figure 1). A description of each study is shown in Table 1.
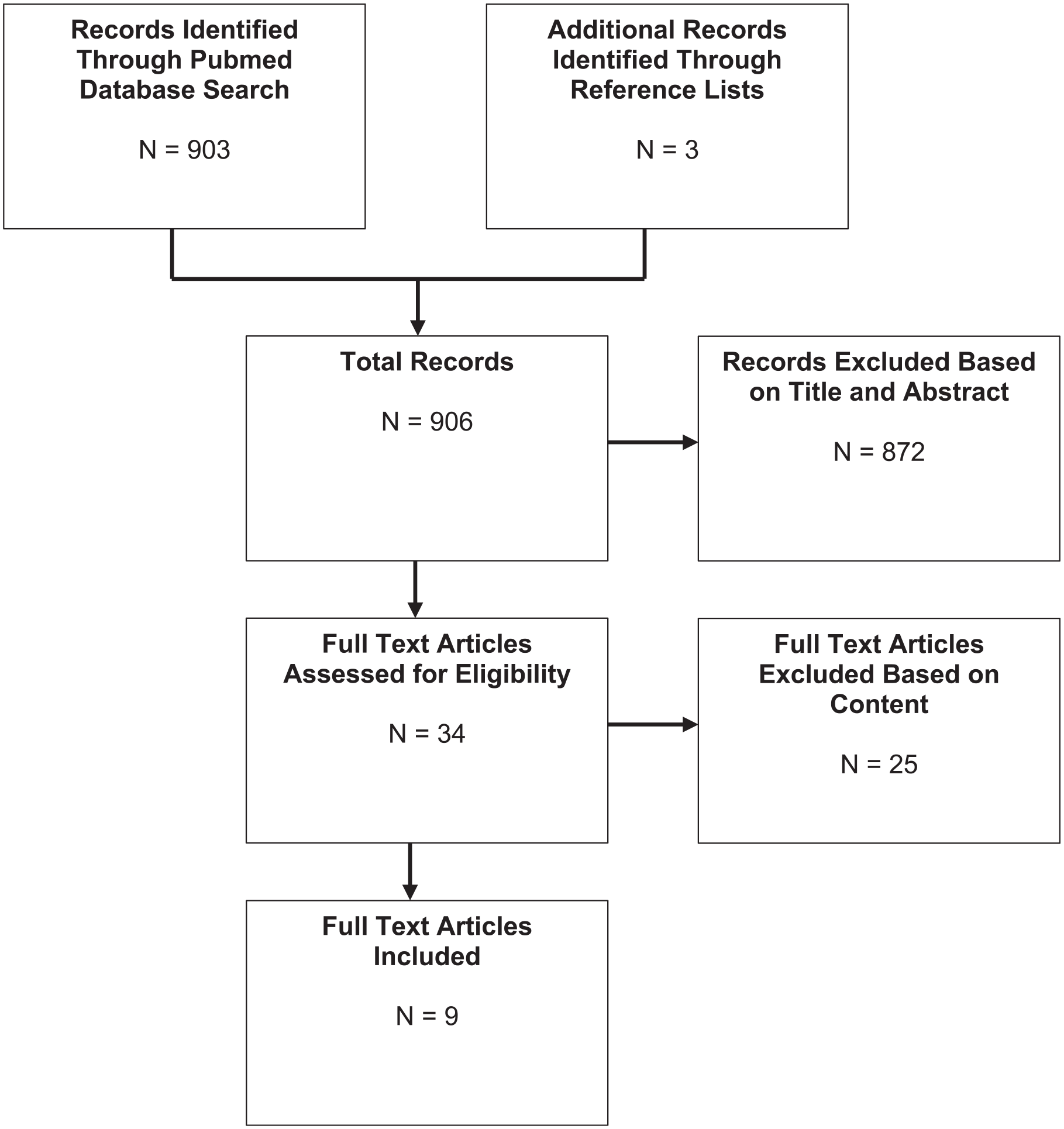
Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flowchart for the 9 included studies.
Main Aims and Objectives of Studies
The studies included in this review were diverse, yet all aimed to investigate evaluation and treatment options for patients with chronic deltoid injuries. We defined chronic deltoid injuries as those to the superficial and/or deep deltoid ligament occurring over 6 months prior. Of the 9 studies identified for full-text review, all used preoperative plain radiographs and MRI for assessment. Eight discussed surgical management, and 7 studies discussed specific techniques for deltoid ligament repair.
Patient Clinical Presentation
All studies reported patient symptoms of ankle instability such as giving way, particularly medially, or subjective ankle weakness following an initial ankle sprain over 6 months prior. Five of 9 studies described patients in their study population with medial ankle pain.6,15,21,24,26 In one series, 10 patients had prior failed lateral ankle ligament reconstruction. 3 All studies excluded patients with neuropathy and inflammatory arthritis. Two studies specifically discussed patients with concomitant lateral ankle pain.6,24
Physical Examination
Five of the studies specifically documented the presence of medial-sided ankle pain on clinical examination in 166 of 208 patients (77%).6,15,21,24,26 Other studies used presence of positive anterior drawer to help diagnose ligamentous instability while acknowledging that this is not specific for deltoid pathology.15,24 One study more specifically described clinical diagnosis of medial ankle instability as medial gutter pain with positive anterior drawer test. 27 Another study described assessing medial instability by applying valgus tilt stress to the heel and comparing to the contralateral side. 15 Pellegrini et al 21 used asymmetric flexible hindfoot valgus deformity as an inclusion criteria in addition to medial-sided ankle pain and subjective instability symptoms. Preoperative range of motion was measured by goniometer in one study, noting decreased ankle dorsiflexion in patients with mechanical ankle instability. 4
Preoperative Imaging
All studies used plain radiographs and MRI in evaluation of their patients. Radiographic measurements included talar-tilt angle in 440 patients (85%) and anterior displacement in 296 patients (57%) (Table 1). Although not specific for deltoid ligament pathology, Lee at al 17 showed 58 of 299 patients with positive varus stress and anterior drawer stress radiographs had evidence of deltoid injury on MRI.
One study described using stress radiographs evaluating degrees of talar tilt in supination, without further details or examples of the stress technique. 4 Another defined stress radiograph diagnosis of medial ankle instability as talar tilt angle ≥2 degrees compared to contralateral ankle. 27
Crim et al 8 used weightbearing ankle and hindfoot alignment radiographs in 42 of 47 ankles showing neutral hindfoot alignment in 33 patients (79%), varus alignment in 7 patients (17%), and valgus alignment in 2 patients (5%).
MRI was used to evaluate the deltoid ligament complex with specific findings discussed for 465 patients. A total of 366 patients (79%) were identified as having concurrent lateral ligament injuries. Deltoid injuries were identified in 289 (62%) of patients with superficial deltoid in 61 and deep deltoid in 146 of patients when specified (Table 1). Chun et al 6 found 18 of 50 patients with chronic lateral ankle instability had MRI findings of deltoid ligament injury, with isolated superficial deltoid injury in 50%, isolated deep deltoid in 11%, and both superficial and deep deltoid in 39%. Crim et al 8 found 72% of their patients had MRI abnormalities in either the superficial or deltoid ligament, with a majority of those involving both components. Lee et al 17 found MRI evidence of deltoid injury in 25% of their patients with ankle instability.
Intraoperative Methods
Diagnostic arthroscopy
Surgical evaluation of deltoid ligament pathology most commonly involved arthroscopy in 255 patients.4,6,8,15,21,24,26 Bucchorn et al 4 described an evaluation of ligament tension, continuity and evaluation of proximal ligament insertion, and measurement of tibiotalar distance while applying pronation stress. Further specifics on measurements or technique were not provided.
Chun et al 6 described assessing medial ligament competence by introducing a 2.9-mm probe into the medial gutter with traction removed from the ankle. Crim et al 8 performed arthroscopy in 36 of 47 cases, with medial ligaments described as normal or abnormal with acknowledgment of variability in evaluation. Hintermann et al 15 assessed instability under valgus stress, and further graded it based on ability to pass a 2- or 5-mm arthroscope into the tibiotalar space. Pellegrini et al 21 described the presence of an ankle drive-through sign, inserting a 5-mm probe toward the posterior aspect of the ankle through the medial gutter to assess for a denuded medial malleolus. Vega et al 24 diagnosed deltoid ligament injury by the ability to introduce a probe between the medial malleolus and deltoid origin in addition to looking for deltoid separation from the medial malleolus while applying an internal rotation force. Wang et al 26 documented performing ankle arthroscopy to confirm injury to the deep deltoid ligament, but did not specify details on technique.
Medial ligament reconstruction
There is a variety of reported techniques for patients diagnosed with chronic deltoid ligament injuries (Table 2). Six studies discussed simultaneous repair or reconstruction of lateral and medial ligaments.4,6,15,21,24,27 Deltoid ligament was repaired in 199 patients, with suture anchors in 173 patients (87%). Suture anchors of various sizes were reported to be used including 13 with Arthrex (Naples, FL) Pushlock 2.9 mm, 24 13 patients with Arthrex 5.0-mm corkscrew, 21 81 patients with Arthrex 2.4-mm, 4 17 patients with Smith & Nephew (Warsaw, IN) 3.5 mm, and 49 patients with Mitek (Depuy Synthes, Raynham, MA) anchors. 15 Thirteen patients had their deltoid repair with suture anchors augmented with an Internal Brace (Arthrex, Naples, FL). 21 Twenty-three patients underwent repair using bone tunnels. 27 Three patients underwent repair involving deltoid ligament but did not specify the exact surgery (Table 2). Deltoid ligament was reconstructed in 3 patients using plantaris tendon autograft. 15
Summary of Surgical Management.

Postoperative Methods and Outcomes
A range of postoperative protocols was used among the studies. Some prescribe nonweightbearing in a splint or cast for 3 weeks 26 to 4 weeks. 27 Others had patients partial weightbearing for 3 weeks in a controlled ankle motion boot after combined medial and lateral ligament repairs, with physical therapy starting at approximately 4 weeks postoperatively. Patients with concomitant osteochondral lesions were maintained nonweightbearing for 4 weeks.4,24
Pellegrini et al 21 did not immobilize patients or restrict weightbearing, and encouraged early rehabilitation after deltoid ligament repair with internal brace augmentation. Other studies were nonspecific and allowed full weightbearing when patients had no pain with ankle loading using a stabilizing shoe for 6 weeks postoperatively. 15
Postoperative functional outcome scores were assessed and reported in 6 studies.4,15,21,24,26,27 Short-term postoperative outcomes at 3 months in one series of combined medial and lateral ligament repairs showed significant improvements in American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot score, range of motion, and decrease in pain using visual analog scale (VAS) scores. 4 Hintermann et al 15 found AOFAS hindfoot score improved overall from 42.9 to 91.6 at final mean follow-up of 4.4 years after surgical reconstruction. One series of patients with chronic rotatory instability who underwent internal brace augmentation for deltoid ligament repair had preoperative Foot and Ankle Ability Measure (FAAM) and 36-Item Short Form Health Survey (SF-36) scores improve from 58.7 to 75.3 and from 60.2 to 84.4 postoperatively, respectively, at a mean time of 13.5 months (P < .01). 21 Vega et al 24 found that the median AOFAS scores increased from 70 (44-77) preoperatively to 100 (77-100) at a final median follow-up of 35 months with a range of 18-42 months in addition to subjective improvement in ankle instability. Similarly, another study on combined medial and lateral ankle ligament reconstruction showed a significant improvement between preoperative and postoperative Karlsson scores from 69.0 to 96.1 points, respectively, and Japanese Society for Surgery of the Foot (JSSF) scores from 69.8 to 94.5 points, at a mean follow-up time of 30 months with range of 24-52 months. 27
The authors also reported radiographic outcomes with a decrease in anterior displacement on stress radiography from 20.1% preoperatively to 10.1% postoperatively, and decrease of talar tilt angle on stress radiographs from 16.7 to 4.6 degrees. 27
Postoperative Complications
Postoperative complications were discussed in 8 studies.4,6,8,15,21,24,26,27 Paresthesias were found in 3 patients in the superficial peroneal nerve distribution, proximal medial malleolus, and in the plantaris graft harvest site that resolved.4,15 Delayed wound healing was reported in 4 patients and superficial wound infection in 1 patient that resolved with local wound care.4,15 No other complications including deep infection, implant failure, or need for reoperations were reported.4,6,8,15,21,24,26,27
Discussion
Approximately 15% to 20% of patients who sustain acute ankle sprains go on to develop chronic ankle instability and recurrent ankle sprains.10,23 Previous studies have shown that the deltoid ligament acts as a lateral stabilizer against inversion in patients with chronic lateral ankle ligament insufficiency. 28 Moreover, chronic deficiency of the lateral ankle ligaments can result in excessive internal rotation and anterior translation of the talus. This can subsequently lead to overload of the anterior deltoid ligaments and result in an abnormal increase in talar rotation, or rotational ankle instability. 24 However, it is unclear if this is a natural sequence of pathology, or whether acute injury to the deltoid ligament complex is a prerequisite. Moreover, despite high clinical outcomes reported after lateral ankle ligament reconstruction for ankle instability, up to 35% of patients demonstrate some level of long-term dissatisfaction or persistent instability.2,12,19 This raises the question of whether the role of medial instability has been underrecognized and undertreated.
Our work specifically evaluated studies discussing the diagnosis, workup, and treatment for chronic deltoid ligament pathology in patients with ankle instability.
Diagnosis
Our study found a variety of clinical examination, radiographic, and arthroscopic parameters discussed in the literature to diagnose and treat chronic deltoid injuries.
The presence of medial-sided ankle pain was the most consistently reported symptom in suspected medial sided ankle instability.4,6,15,21,24,26 One study found correctable hindfoot valgus and pronation deformity, and history of patient-described sensation of their ankle giving way to have the highest positive predictive value in arthroscopically confirmed medial ligament pathology. They emphasized the importance of concurrent calcaneal osteotomy in cases of hindfoot malalignment, in order to prevent recurrent instability after resuming sports activity. 15
Overall, the presence of laxity to anterior drawer in the setting of medial gutter pain and instability may warrant further evaluation of medial ligaments in addition to lateral ligaments. However, challenges to diagnosis include delineating specific eversion or pronation trauma from patients’ reported history because of lack of patient recollection as well as often multitude of sprains prior to presentation.
Plain radiographs can assist in evaluation of patients with CAI, but clear radiographic parameters have not been established. Plain radiographs assessed talar-tilt angle in 440 patients (85%). Yasuda et al 27 defined medial ankle instability as a talar tilt ≥2 degrees compared to the contralateral ankle. Hintermann et al 15 noted normal talar tilt and anterior drawer stress radiographs in their 12 patients with isolated medial instability. Contrastingly, Buchhorn et al specifically used supination stress ankle radiographs, which showed significant improvement postoperatively. However, no context was given on normal values relative to their listed preoperative and postoperative values, or details on the clinical significance of their measurements. 4 Crim et al 8 obtained hindfoot alignment radiographs, but no correlation was made between alignment and presence of deltoid pathology. 21
Radiographic criteria defining ankle instability under varus stress has previously been defined as >15 degrees of tibiotalar tilt angle or >10-degree difference between ankles. 7 Although high interobserver reliability in measurements has been demonstrated, 18 consistency in technique and image quality has been shown to be a concern. 5 This raises the question of whether a difference of 2 degrees can be reliability appreciated as a criterion in diagnosing medial ankle instability.
The correlation between MRI findings and clinical significance is unclear. Studies showed an overall high incidence of deltoid ligament pathology on MRI in patients with ankle instability, ranging from 25% 17 to 72%. 8
In one study, preoperative MRI was deemed diagnostic of instability if the posterior tibiotalar ligament lacked normal striations or demonstrated hyperintense signal change on T2 or echo sequences. 27 Chun et al found that of 18/50 patients with deltoid ligament pathology on MRI, only 5/18 had medial ankle tenderness on examination. They further found MRI sensitivities for detection of deltoid ligament injury to be 91% when compared to arthroscopic findings. 6 Similarly, Crim et al 8 found 72% incidence of deltoid pathology on MRI in their cohort of 46 patients without any medial ankle pain. Contrastingly, Buchhorn et al 4 found 83% correlation between imaging and radiographic findings. However, neither the clinical nor radiographic parameters used was clearly defined in their work.
These data highlight the importance of detailed physical examination of the medial ankle in all patients with ankle instability symptoms, in addition to MRI evaluation of the deltoid ligament for pathology.
Arthroscopy
Use of diagnostic arthroscopy has been discussed to aid in diagnosis of deltoid ligament injuries, with various methods described. Several studies have defined a drive through test for deltoid insufficiency as the ability to pass either a 2.9-mm arthroscope or 4.0-mm shaver into the medial gutter.13,21,22 However, the sensitivity and specificity of this test has not been validated. Hintermann et al 14 similarly defined moderate instability as the ability to pass a 5-mm hook into the medial gutter. They also characterized visualization of the deltoid ligament for assessment of continuity and degree of distension with eversion and pronation of the foot. One study found that arthroscopic visualization of posterior tibialis tendon was indicative of complete deep deltoid injury, whereas inability to completely visualize the posterior tibialis tendon was indicative of partial deep deltoid injury. 1
Buchhorn et al 4 evaluated tension of the collateral ligaments at their proximal insertion under tension during arthroscopy, although clear parameters defining abnormal pathology or technique were not specified. They reported 83% correlation between clinical and arthroscopic findings, with deep deltoid injury in 83% and combined deep and superficial deltoid lesions in 17% of their patients. Another study documented arthroscopic appearance of the posterior tibiotalar ligament as torn, partially fibrotic, or meniscoid in form. No arthroscopic instability maneuvers or tests were described for deltoid ligament stability. 27
Based on these data, arthroscopic identification of deltoid ligament injuries should involve direct visualization of the ligament under static tension and pronation and eversion stress, as well as instability assessment with attempted passage of at least a 2.9-mm arthroscope or probe into the medial gutter.
Operative Treatment
The deltoid ligament plays an important role in rotatory stability of the ankle, yet there is a scarcity of data specifically discussing surgical technique in patients with CAI. Previous studies have looked at deltoid repair constructs in ankle fractures noting that placing an anchor in the middle of the anteromedial aspect of the medial malleolus recovered a near to normal tibiotalar coupling and medial clear space values. 25 This may be extrapolated to patients who have chronic deltoid ligament injuries in the setting of CAI. Contrastingly, Yoo et al 16 described a case of medial and lateral ankle ligament reconstruction with semitendinosus autograft. Consideration can be taken for use of allograft in patients with hyperlaxity, failed prior repair, high demand sports or labor, or BMI >30.9,11,20
Six studies discussed simultaneous repair or reconstruction of lateral and medial ligaments.4,6,15,21,24,27 In the majority of patients in our identified series, suture anchor was used in repair.
Hintermann et al 15 performed concurrent calcaneal osteotomy in patients with valgus and pronation deformity in order to prevent loss of correction after resuming sports activity.
Outcomes
All studies showed significantly improved function and pain relief following medial ligament procedures, as evaluated by various outcome scoring methods. In one series of 13 patients undergoing combined all-inside repair of medial and lateral ligaments with suture anchors, 12 of 13 had complete resolution of medial ankle pain. 24 Another series of 23 athletes who underwent simultaneous deltoid and lateral ligament repair, all returned to their preinjury level of sports. 27 There were no reported secondary procedures performed for any patients in the assessed studies.
Limitations
This study has several limitations. This is a systematic review study with risk of potential unmeasured bias. We sought to include all studies that met our inclusion and exclusion criteria, but cannot ensure that all studies were included in our analysis. It is also difficult to draw conclusions regarding isolated medial ankle instability as many of our included studies discussed medial and lateral ankle ligament injuries. Source studies were mainly retrospective case series.
Conclusions
Deltoid injuries have been shown to commonly occur in patients with CAI. This work highlights the importance of recognizing these injuries on comprehensive preoperative physical examination and imaging, as well as evaluation of the medial structures during diagnostic arthroscopy. Our work also demonstrates that there is currently limited data on the correlation between imaging findings and clinical significance, as well as specific diagnostic tests on examination or imaging to guide surgical treatment. Future work in this area would be helpful to improve our understanding of chronic deltoid injuries to help patients and surgeons better comprehend treatment options for medial ankle instability.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251323903 – Supplemental material for Diagnosis and Management of Deltoid Ligament Injuries in Chronic Ankle Instability: A Systematic Review
Supplemental material, sj-pdf-1-fao-10.1177_24730114251323903 for Diagnosis and Management of Deltoid Ligament Injuries in Chronic Ankle Instability: A Systematic Review by Amanda Anderson, Maddison McLellan, Ryan Kim and Naudereh Noori in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study as there are no patient identifiers in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.