
Abstract
Background:
Surgical management of patients with acute and chronic ankle instability (CAI) has historically focused on the lateral ligament complex. Recent studies in CAI patients have shown that magnetic resonance imaging (MRI) and arthroscopy demonstrate concomitant injury to the deltoid ligament complex We performed a systematic review to determine if consistent clinical, diagnostic imaging, or arthroscopic findings of deltoid ligament injury in the setting of CAI have been described. In addition, we sought to determine if treatment options and/or clinical outcomes have been described.
Methods:
A systematic review was conducted using the PubMed, MEDLINE, and Embase databases. Articles were included if they had a majority of patients 18 years of age or older, focused on deltoid ligament injury in ankle instability, and reported diagnostic and/or treatment methods. Articles were excluded if the study focused on the deltoid ligament in the acute fracture setting. All included articles were assessed for diagnostic criteria, treatments, and patient outcomes.
Results:
Our search yielded 157 articles, of which a total of 13 were included in our study. Arthroscopy was described as the gold standard to diagnose and evaluate the severity of deltoid ligament injury, however, little objective data on the arthroscopic diagnosis of deltoid ligament insufficiency was reported. MRI was the imaging modality of choice to evaluate deltoid ligament injury and had a high sensitivity and specificity when compared with arthroscopy. No standard MRI diagnostic criteria for deltoid ligament injury were identified in the literature. Specific treatment techniques and long-term outcomes were not well described in the manuscripts included in this review.
Conclusion:
There is limited knowledge on deltoid ligament insufficiency in the setting of chronic ankle instability. Criteria for characterizing deltoid ligament damage with diagnostic imaging appear to be evolving, but there is no standard classification. Only 1 author has described a method to evaluate deltoid ligament competency on arthroscopic examination. There are currently no objective data to guide treatment decisions.
Level of Evidence:
Level III.
Introduction
Ankle sprains are among the most common sports-related injuries. 1,27 Approximately 10% to 30% of these patients will fail conservative management and develop chronic ankle instability (CAI). Persistent pain, a sensation of “giving way,” and recurrent injures are common symptoms that characterize CAI. 2,11,23 Damage to the lateral ligament complex in patients with CAI has been widely described in the literature, and surgery to repair the lateral ligament complex of the ankle has been the primary surgical treatment. 12,18,23 Recently, there has been evidence to suggest that there is frequently a concomitant injury to the deltoid ligament complex in CAI cases.
Though a multiband structure, it is accepted that the deltoid ligament is composed of superficial and deep components, typically separated by a fat pad. 4,20 The superficial structure is made up of the superficial tibionavicular, tibiospring, and tibiocalcaneal ligaments. 4,20 Their function is to resist external rotation of the talus in relation to the tibia. 22 The deep deltoid complex contains 2 components, the deep posterior tibiotalar ligament and the anterior tibiotalar ligament. 22 Similar to the superficial component, the deep complex aids in resisting external rotation of the talus against the tibia and is also the primary constraint to valgus forces and lateral translation. 14 Together, the bands are also responsible for resisting posterior translation of the talus. 26
Recent studies have shown that CAI involves the medial ligament complex more often than previously thought. Hintermann et al first demonstrated the prevalence of deltoid ligament injuries using arthroscopy. 12 Since then, multiple studies have shown injury to the deltoid ligament on magnetic resonance imaging (MRI) in patients complaining of CAI. 3,7,9,12,13 The suggested high prevalence of deltoid ligament injury demonstrates the need for further knowledge in this area.
The literature exploring the role of the deltoid ligament in CAI is limited, but emerging. We performed a systematic review of the literature to determine if consistent clinical, diagnostic imaging or arthroscopic findings of deltoid ligament injury have been described. In addition, we sought to determine treatment options and clinical outcomes.
Materials and Methods
A systematic review was performed using the databases MEDLINE (OVID), PubMed, and Embase. Articles were selected if they met the following inclusion criteria: Biomechanical, cadaveric, and clinical studies examining the clinical diagnosis, diagnostic imaging, or treatment of acute and chronic deltoid/medial ankle ligament injuries in the absence of acute ankle fracture Majority (>50%) adult patients (age ≥18 years) English language or translation available
Exclusion criteria were as follows: Studies that did not meet inclusion criteria Review articles Studies in which more than 50% of the participants were under 18 years of age.
Both authors independently performed the review. Results from all databases were combined and the duplicate titles were removed. All the articles were reviewed by the 2 authors at each stage (titles, abstracts, manuscripts) and disagreement at all stages except the final led to inclusion. At the final stage (manuscripts), a consensus decision was made on all disagreements. Figure 1 demonstrates the search strategy and flow chart for the review.

Figure outlining search strategy and numbers of papers included at each stage of the review.
Once the manuscripts were selected, both authors performed data extraction together. Basic information extracted included title, authors, level of evidence, year of publication, and number of patients. Specific data extracted included diagnostic criteria used, physical examination, radiologic and arthroscopic findings, comparisons between arthroscopic and diagnostic imaging, method of surgical intervention, and patient outcomes.
Results
A total of 13 articles met the inclusion criteria and were included in the final analysis (Table 1). Six described physical examination findings for medial ankle instability. 6,8,12,13,15,25 All six articles described different physical examination criteria; the most common physical findings, present in 5 of the papers, were medial-sided pain and a sensation of “giving way” medially. Two papers described a fallen medial longitudinal arch with a calcaneal valgus deformity. 12,25 None of the papers commented on correlation between examination findings and degree of damage on imaging and/or arthroscopy.
Articles Included in the Final Analysis and Their Level of Evidence.

Eight of the 13 articles described diagnostic imaging findings, with MRI being the modality of focus in all of those articles. 5,6,8 -10,15,16,21,25 One study showed that there was increased medial space widening on radiography with external rotation of the ankle while holding the hindfoot in varus. Four articles included a classification scheme for their findings, which are summarized in Table 2. 6,9,15,21 There were similarities in grading scheme between 2 of the papers, with otherwise no consistency among the others. 9,15
Summary of MRI Criteria for Diagnosis of Deltoid Ligament Injury.
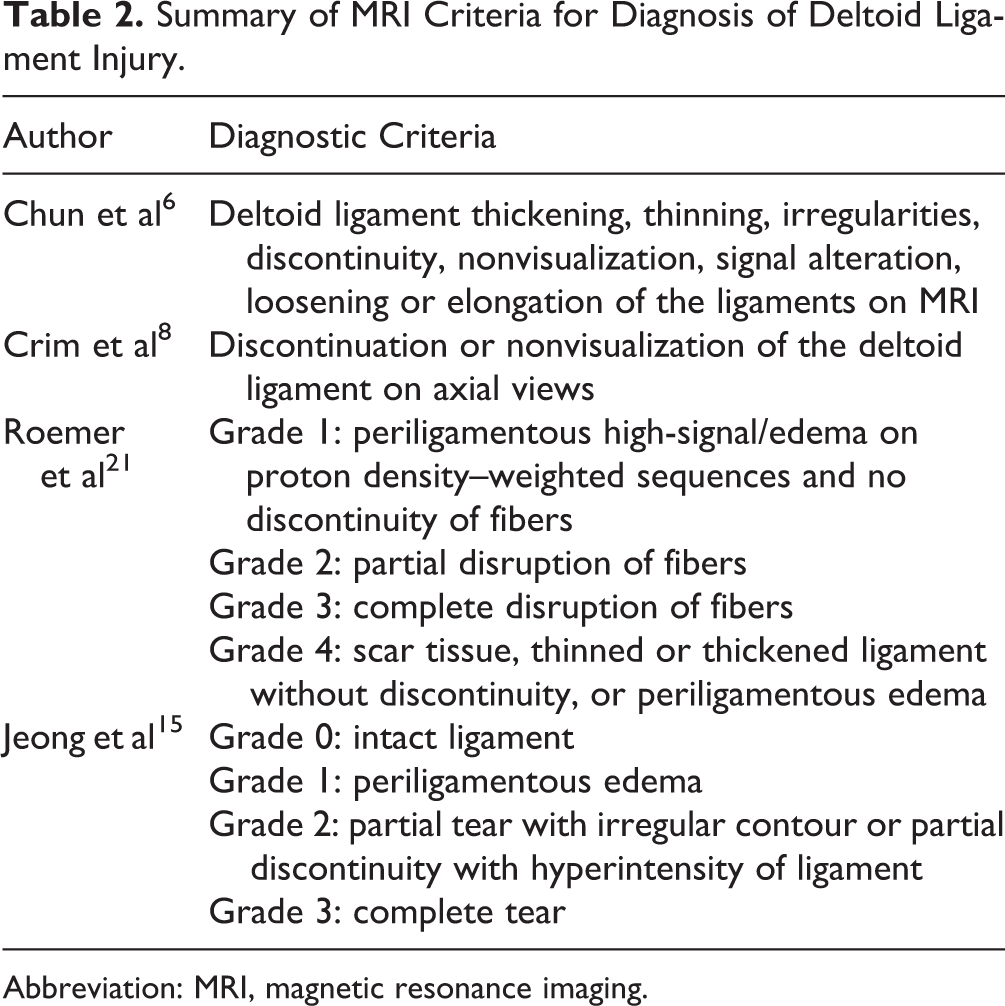
Abbreviation: MRI, magnetic resonance imaging.
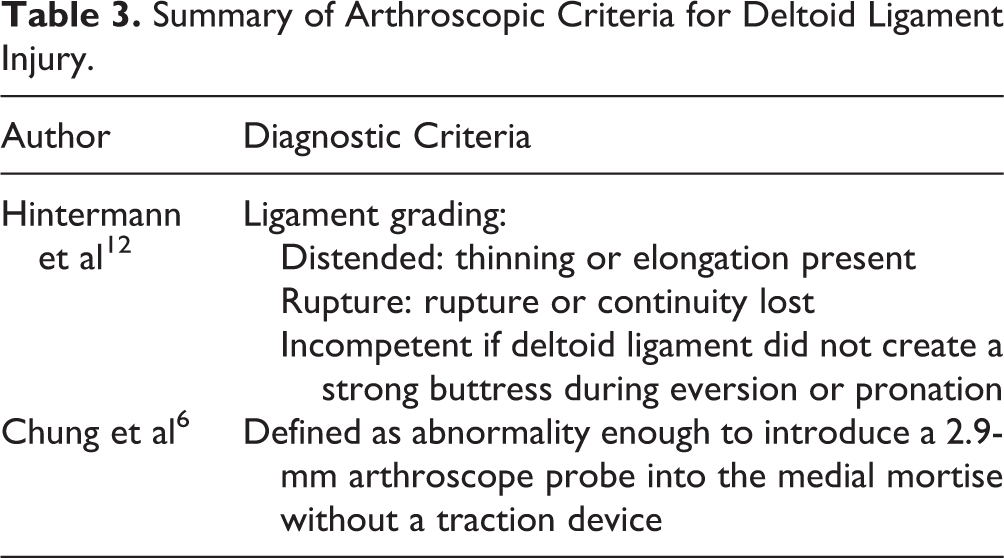
Arthroscopy was presented as the gold standard for diagnosis in all papers 3,6,9,12,13,15,25 ; however only 1 study described its arthroscopic diagnostic criteria. 12 Two studies described a classification system for ligament injury grading 6,12 (Table 3). The classification system was not correlated to treatment or outcome in either paper. Two papers correlated MRI findings of deltoid ligament injury to arthroscopic findings and found that MRI had a sensitivity of 83.5% and a specificity of 94% of detecting the presence of deltoid injury. 6,8 No article correlated the grade of deltoid injury on arthroscopy or MRI to physical examination findings.
Summary of Arthroscopic Criteria for Deltoid Ligament Injury.
Seven articles described treatment, with 3 of the articles describing suture anchor fixation of the deltoid ligament and 1 describing a Brostrom-type procedure. 3,6,8,13,15,17,25 One article described concomitant fixation of the lateral and deltoid ligaments in the same procedure, with the deltoid fixation being performed with a suture anchor. 3 Three articles (all 3 using suture anchor fixation) described improved American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot outcomes 3,13,25 postoperatively (Table 4).
Summary of AOFAS Hindfoot Outcomes Following Deltoid Ligament Repair in the Setting of CAI.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; CAI, chronic ankle instability.
Discussion
Ankle sprains are common injuries and, for those that fail non-surgical management, the first line of treatment has focused on lateral ligament complex reconstruction. 18 There is mounting diagnostic imaging and arthroscopic evidence that there is frequently injury to the medial ankle ligament complex. In the authors’ opinion, the diagnosis of medial-sided ankle instability is very challenging, and obvious physical examination features are often not present. We believe this condition is potentially underdiagnosed and undertreated. This systematic review evaluates the evidence surrounding deltoid ligament injury in CAI.
The deltoid ligament is made up of discrete superficial and deep layers, with each layer having different functions. 4 The deep deltoid complex resists posterior talar translation and acts as a restraint against lateral translation of the talus away from the medial malleolus. 14,19,22 The superficial ligament is the primary restraint against rotation, acting to prevent external rotation of the talus. 22 The included studies did not describe any physical examination maneuver that would test for rotational instability or increased posterior translation. Given the function of the deltoid complex, these would arguably be the most important tests for clinically determining competence of the deltoid ligament. The authors are not aware of any method to reproducibly demonstrate rotational instability of the talus. Both the lateral and medial ligament complexes contribute to rotational stability of the talus in the mortise, which makes interpreting any demonstrated rotational instability challenging. 22
MRI is the imaging modality of choice to assess damage to the deltoid ligament. It has been shown to be both sensitive and specific in detecting injury to the deltoid ligament. The major drawback to MRI (and all static imaging) is the lack of correlation between ligament injury and ligament function. Because of the sensitivity of MRI, any prior injury to the deltoid ligament complex may be discovered; however, this does not inform the surgeon if the talus is truly unstable in the sagittal or axial planes. MRI may, however, be able to provide information that can increase the treating surgeon’s suspicion for deltoid incompetence.
Further work needs to be done to create a standard classification scheme for deltoid injury and correlating this to arthroscopic findings. Ideally, a stress test or weightbearing imaging technique that could demonstrate axial plane instability could be developed to confirm rotational instability of the talus. One potential for this would be weightbearing CT scans. 24 The authors are not aware of any such imaging technique having been described for deltoid insufficiency.
Arthroscopy was presented as the gold standard for classifying deltoid ligament pathology. Hintermann et al 12 were the first to describe a classification scheme for arthroscopic findings of deltoid ligament injury in CAI; however, the description is somewhat challenging to interpret. Diagnostic criteria described include the lack of “an obvious strong medial buttress” to eversion, and an “excessive lifting away of the talus from the medial malleolus with anterior stress.” The authors find this difficult to interpret when performing ankle arthroscopy, as there is substantial variability in talar motion between patients. Ideally a description of “normal” medial-sided talar motion on ankle arthroscopy could help define what abnormal medial translation, rotation, and distraction look like. None of the articles reviewed describe a correlation between clinical findings and arthroscopic findings. Furthermore, the arthroscopic findings described do not dictate treatment.
Three studies used the AOFAS hindfoot score to report outcomes. The objective component of the AOFAS hindfoot score and its reliability has not been validated. Given the poor reliability of this score, it is difficult to comment of the validity of these findings. One of the major symptoms of CAI is instability. Potentially, an instability score—such as the identification of functional ankle instability scale—might be better used to capture true improvement in ankle function.
The major weakness of this study is the lack of quantitative data in the studies included in the review. All of the studies included in this review were cohort studies. The lack of high-quality evidence limits the impact of this systematic review. There is a clear need for further studies in this area.
In conclusion, injury to the deltoid ligament in CAI is more common than previously believed and can have a significant outcome on patient function. However, there are no objective diagnostic criteria for deltoid ligament insufficiency. Although arthroscopy is the gold standard for the diagnosis of deltoid insufficiency, there does not exist objective criteria to use in making this diagnosis, nor is there evidence to guide treatment decision making.
Supplemental Material
Supplemental Material, FAO860073-ICMJE - Diagnosis and Management of Deltoid Ligament Insufficiency
Supplemental Material, FAO860073-ICMJE for Diagnosis and Management of Deltoid Ligament Insufficiency by Sarup S. Sridharan and Andrew Dodd in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.