
Abstract
The deltoid ligament is the primary stabilizer of the medial side of the ankle joint. It is a complex structure with an origin at the medial malleolus from where it spreads fan shaped distally with an insertion into the medial side of the talus, calcaneus and navicular bone. This chapter gives an overview of the anatomy, function, and pathology of the deltoid ligament.
The deltoid ligament can become insufficient as a result of an ankle injury or prolonged strain. In the acute setting, deltoid insufficiency often coincides with multi ligament injury the ankle joint; syndesmosis injury, or ankle fractures. Management in the acute phase remains a subject of debate. Some orthopedic surgeons have a tendency towards repair, whereas most trauma surgeons often treat the deltoid nonoperatively. In the chronic setting the ligament complex is often elongated as a result of prolonged strain. It often coexists with a hindfoot valgus, as is the case in planovalgus feet. In such a case a realignment procedure should be combined with the deltoid repair.
Introduction
The deltoid ligament is the primary stabilizer of the medial side of the ankle joint. It is a complex structure with an origin at the medial malleolus from where it spreads fan shaped distally with an insertion into the medial side of the talus, calcaneus and navicular bone. Deltoid is Greek for deltoeides, triangular. In the literature the deltoid ligament is also referred to as the medial collateral ligament of the tibiotalar joint.
The deltoid ligament has a superficial and a deep part, which spring from the medial distal side of the medial malleolus. It has multiple insertions of which the deep fibers insert into the talus at multiple locations. The superficial bands of the deltoid insert into the sustentaculum of the calcaneus, a portion extends down to the spring ligament medially and a portion extends plantar into the medial aspect of the navicular forming a thickened expansion of the medial capsule of the talonavicular joint. As a result the deltoid acts to stabilize the talus in the ankle mortise, stabilize the medial side of the subtalar joint, and supports the medial column of the arch of the foot at the talonavicular joint.
There are a number of scenarios in which the deltoid can be insufficient. In acute trauma, the deltoid can be injured as part of an ankle injury with syndesmosis instability. This results in an unstable ankle joint, which leads to peak loading of the cartilage at certain spots, which might lead to early osteoarthritis. 1 Furthermore, when trauma to the deltoid is left untreated, the instability can result in a posttraumatic planovalgus foot. 2 These two pathologies can coexist. As such, the deltoid may need to be repaired and debrided in the late presentation of syndesmosis instability, and may need to be repaired after a deltoid ligament injury with the development of a symptomatic unilateral planovalgus foot.
Deltoid ligament anatomy
Studies on deltoid anatomy have identified separate ligament structures. It is widely agreed upon that the deltoid complex is composed of two layers, the deep and superficial. The majority of the superficial ligaments cross two joints: the ankle and the subtalar or talonavicular joints. The deep ligaments cross only the ankle joint.
3
The deep and superficial parts can be further subdivided. Milner et al. proposed a subdivision into six ligaments,
4
which has been reported afterwards in literature.
5
The subdivision is somewhat arbitrary as most of the bands are continuous to one another.
6
Furthermore all six ligaments are not always present. The deltoid was divided into two deep and four superficial ligaments. Two deep bands consist of the deep posterior tibiotalar and deep anterior tibiotalar ligament. Four superficial ligaments consist of the tibiospring (or tibioligamentous), tibionavicular, superficial posterior tibiotalar, and tibiocalcaneal ligaments (Figure 1). The deep posterior tibiotalar ligament was the largest ligament of the deltoid complex. The tibionavicular, tibiospring and deep posterior tibiotalar ligaments are present in every individual. The other three previous described ligaments show anatomic variation. Of which superficial variants are called: anterior tibiotalar ligament, the anterior tibiotalonavicular ligament, and the intermediate tibiotalar ligament. Regarding the deep ligaments four variants were described.4,5 The ‘spring ligament’ cannot be seen separately from the deltoid ligament complex as they are closely related via the tibiospring ligament. Therefore they interplay in stabilizing the medial side of ankle and subtalar joints.
3
Finally, the deltoid is partially covered by the tibialis posterior tendon, of which the tendon sheath forms a part of the deltoid fibers, covering the posterior and middle part. This is comparable to the peroneal tendon sheath covering the lateral ligaments
7
. Schematic depiction of multiple segments of the deltoid ligament. The left figure depicts the deep part of the deltoid ligament. The right image depicts the superficial part of the deltoid ligament. 1. Deep posterior tibiotalar ligament; 2. Deep anterior tibiotalar ligament; 3. Superficial tibiotalar ligament; 4. Tibiocalcaneal ligament; five Tibiospring ligament; 6. Tibionavicular ligament; 7. Spring ligament.
Function of the deltoid ligament
The deltoid ligament is a strong restraint in limiting talar abduction. This motion is also described as negative tilt or valgus tilt of the talus. Based on cadaver studies the deep and superficial part of the deltoid are both effective at restraining this motion. The intact deltoid ligament allows only 2–3 mm of separation between the talus and medial malleolus. When the deep deltoid ligament is released, the talus can be separated from the medial malleolus by 4 mm. 8 This is known as the “drive through” sign in the ankle joint. Other restraints the deltoid provides are on rotation of the talus in the mortise and medial restraints to the subtalar joint and talonavicular joint. The talocalcaneal ligament specifically limits talar abduction, while the deep layers of the deltoid ligament rupture in external rotation without the superficial portion being involved. 8 The tibiospring and tibionavicular ligaments have more complex restraints on the medial ankle, as the first forms a complex with the spring ligament and the latter also crosses the talonavicular joint. 5 Further understanding of specific function of separate parts of the deltoid ligament is needed and might result in a better and more anatomical repair and reconstruction guidelines.
Deltoid insufficiency can occur in the acute setting or as a result of chronic overload. In the acute setting an eversion and/or pronation injury can result in injury to the deltoid ligament. An example of this is when the foot is fixed on the ground and the body produces an eversion force to the foot, resulting in valgus stress in the ankle. A second possibility is when the lower leg is forced into internal rotation, when the foot is fixed on the ground. This results in a pronation stress to the hindfoot, and direct stress on the deltoid ligament (mainly deep part).
In the setting of a chronic deltoid insufficiency, the talus tilts in the ankle mortise, which results in a decrease of the tibiotalar contact area of the cartilage. Focal increase of pressure can result in damage to cartilage and eventually an arthritic ankle. 1 Therefore deltoid ligament repair is needed, even in a well-preserved ankle joint, with deltoid ligament instability.
The repair of an instable deltoid complex might slow down the degeneration of the cartilage.
Diagnosis of deltoid insufficiency
Physical exam
Typically, in the acute setting, the patient presents with tenderness and hematoma formation along the deltoid ligament. In the chronic setting pain over the anteromedial side of the ankle as well as the medial gutter is often described. Patients can report a feeling of medial laxity. When weightbearing the foot often shows increased pronation and a valgus hindfoot. Active recruitment of the tibialis posterior tendon can correct this phenomenon. Varus stress test and the anterior drawer test can confirm deltoid insufficiency. 2
Imaging
Deltoid insufficiency can be diagnosed via simple weightbearing radiographs. In the acute setting, the talus can shift laterally as a result of damage to the lateral restraints of the ankle mortise, as is the case in syndesmosis injury and certain ankle fractures. An increased medial clear space is observed. In the chronic setting, when the deltoid is ruptured or elongated imaging can show the talus tilted into varus, showing widening on the medial side (Figure 2). More than 3 mm widening can be considered pathological. Furthermore, plain radiographs are used to exclude other bony pathologies. Stress radiographs can be helpful for uncertain cases, but remains disputable as the technician needs to know exactly what to do. Conventional imaging of left foot: AP and Lateral weightbearing images showing a chronic deltoid ligament insufficiency in the setting of chronic stress due to the severe valgus hindfoot alignment with a severe planovalgus foot. As a result of the deltoid insufficiency, the talus is allowed to tilt in the mortise, leading to edge loading of the talar dome onto the tibia plafond.
A conventional CT scan can be helpful to asses the congruency of the ankle joint as well as the medial clear space in more detail (Figure 3). But the CT scan is mainly helpful to exclude other pathology, such as ankle fractures, coalitions etc. Weightbearing CT scans are expected to be sensitive in diagnosing subtle deltoid ligament insufficiency. A superficial deltoid ligament injury in a marathon runner.
A MRI scan is very sensitive in detecting any form of deltoid injury. As a result, the clinical implications of subtle findings on MRI scan are often not clear (Figure 4). Furthermore, a high incidence of deltoid abnormalities is present in healthy individuals. Mainly the deep deltoid is prone to misinterpretation as it often appears striated and hyperintense on T2 MRI images.
9
All in all, to come to the right diagnosis and treatment plan, the history and physical exam in combination with weightbearing X-rays remain key. A 3D reconstruction of a CT scan, showing the medial widening, in the setting of a acute deltoid ligament rupture with a lesion of the syndesmosis and a more proximal fibula fracture. There is an avulsion fracture of the distal tibia visible in the posterior view of the syndesmosis.
Ankle arthroscopy
Ankle arthroscopy can assist in the diagnosis of deltoid ligament insufficiency. The tearing of the anterior part of the deep and anterior part of the superficial deltoid off the medial malleolus or off the medial talus can be seen (Figure 1). When assessing the superficial deltoid only the anterior part can be visualized, which is challenging, as the joint space is narrow. Additionally arthroscopy allows for detecting additional pathologies such as lateral ligament instability and cartilage lesions. Around 75% of patients who have chronic medial instability of the ankle show an associated insufficiency of the anterior talofibular ligament that results in a complex rotational instability of the talus within the ankle mortise. 8
During arthroscopy, the ankle joint is graded stable when there is some translocation of the talus, but not enough to open the ankle joint by more than 2–3 mm. The joint can be considered unstable when the talus subluxes out of the ankle mortise, allowing for introduction of the arthroscope into the tibiotalar space. The joint is severely unstable when the talus moves easily out of the ankle mortise, or when access into the posterior aspect of the ankle joint is obtained without significant traction on the heel. 10
Ankle arthroscopy is also useful in the setting of a chronic deltoid injury. Not only to determine the severity of the deltoid instability, but mainly to debride the medial gutter and to assess other structures in the ankle. Anterior osteophytes may cause anterior ankle impingement and may block reduction of the talus to a neutral position in the ankle mortise and thereby impair adequate deltoid ligament repair. 11
Need for deltoid repair in acute setting
Controversy remains regarding the management of a deltoid rupture in the acute setting. When left unreconstructed, the deltoid might not heal adequately. The possibility of developing medial ankle instability, secondary deformities, articular impingement, mal-reduction, and osteoarthritis is high.12,13 Some would advocate for a more aggressive approach to instability. 14 ). When the deltoid is repaired, possibly a more aggressive rehabilitation and an earlier return to activities can be achieved. 15 Non-operative approach to deltoid lesions in ankle fractures omits the risk of wound complications. In a traumatized ankle, the risk of wound complications should not be underestimated. 16
Deltoid ligament insufficiency in ankle fractures with syndesmotic injury
Typically, the deltoid injury coincides with an ankle fracture and injury to the syndesmosis. Historically, the preference is given to exclusive repair of the fracture and syndesmosis. 17 However, a biomechanical cadaveric study showed that a repair of the deltoid ligament in combination with treatment of the syndesmotic injury and/or the ankle fracture, resulted in increased joint stability regarding the talar tilt and talar slide. 18
It has been shown that the deltoid ligament repair will result in reduction of the medial clear space when measured during the follow up period. 19 A systematic review did not provide an answer as the data were not unambiguous, but deltoid ligament repair was suggested to be a better alternative than trans syndesmotic fixation. 20 A deltoid repair resulted in good outcomes in 20 ankles. A full arthroscopic repair of the deltoid and lateral ligaments has shown great promise. 21 In patients with a high risk for wound complications, such as patients with diabetes, an arthroscopic technique is recommended.
Need for deltoid repair in chronic setting
In the setting of a chronic deltoid insufficiency, the talus tilts in the ankle mortise, which results in a decrease of the tibiotalar contact area of the cartilage. Focal increase of pressure can result in damage to cartilage and eventually an arthritic ankle. 1 Therefore deltoid ligament repair is needed, even in a well-preserved ankle joint, with deltoid ligament instability.
The repair of an unstable deltoid complex might slow down the degeneration of the cartilage. 14 ). In the chronic condition often multiple bands of the deltoid complex are affected. Therefore, the entire deltoid ligament complex should be repaired. 10 In the setting of an end stage OA patient the deltoid repair can be combined with a total ankle replacement. In the setting of a flatfoot and with ankle osteoarthritis, the deltoid repair should be combined with a flatfoot correction. In the setting of partial cartilage damage, an offloading distal tibial osteotomy plus a ligament repair can be considered. It remains unclear which construct and which technique is superior in reconstructing the deltoid ligament in the chronic setting. Often the injury includes a tear of the superficial anterior bundles, as well as parts of the deep bundles. As such the entire deltoid should be reconstructed.
Deltoid repair techniques
In repair either a suture anchor system, allograft or autograft tendon is used. Depending on the skill of the surgeon this can be done as an open technique, an arthroscopic technique or a combined technique. Mechanical studies comparing the repair types are not present. Some authors report reconstruction techniques that show promising results in restoring eversion and external rotation stability to the talus, with similar results to the intact deltoid ligament. They report that the components chosen to fix the tendon graft to the bone are of great importance. 1
General technique
A general anesthetic, spinal anesthetic or nerve block can be used. If a spinal or general anesthetic is applied, a thigh tourniquet can be used, which can be beneficial when regarding the relaxation of the tendons medially. Furthermore, it allows for autologous hamstrings tendon harvest. If a nerve block is applied, then a sterile calf tourniquet is the best alternative. Equipment needed includes a scope, preferably a larger 2.9 scope, a 3.5 shaver, and devices to repair the deltoid ligament provided by the industry. The patient should be positioned in such a way, that the limb could be changed in position in case a direct medial approach is required. A beanbag is considered practical as it can be deflated if needed. Usually one starts with the arthroscopic inspection of the ankle joint and deltoid ligament. Portals include the standard anteromedial and anterolateral portal, and a portal at the location of the medial malleolus or medial gutter. Occasionally a posterior portal is required. Once the scope is inserted the deltoid ligament is inspected. As the deltoid is often injured in combination with damage to the syndesmosis, the integrity of both should be inspected through the arthroscope (see Figure 5(a)). The deltoid can be probed and its insufficiency determined. If there are medial osteophytes present these can be removed using a burr and a shaver. The medial gutter may also have ligament fragments or bone fragments preventing reduction (see Figure 5(b)). These can be removed using the two medial portals. Images of an anterior ankle scope of a right ankle: (a) Deficiency of the deltoid: ruptured ligament fibers in the joint space and medial widening of the ankle joint. The talar dome is inferior and the tibial plafond superior. (b) Medial impingement: congestion of the medial gutter with scar tissue and remnant deltoid fibers as a result of the rupture of the deep deltoid ligament.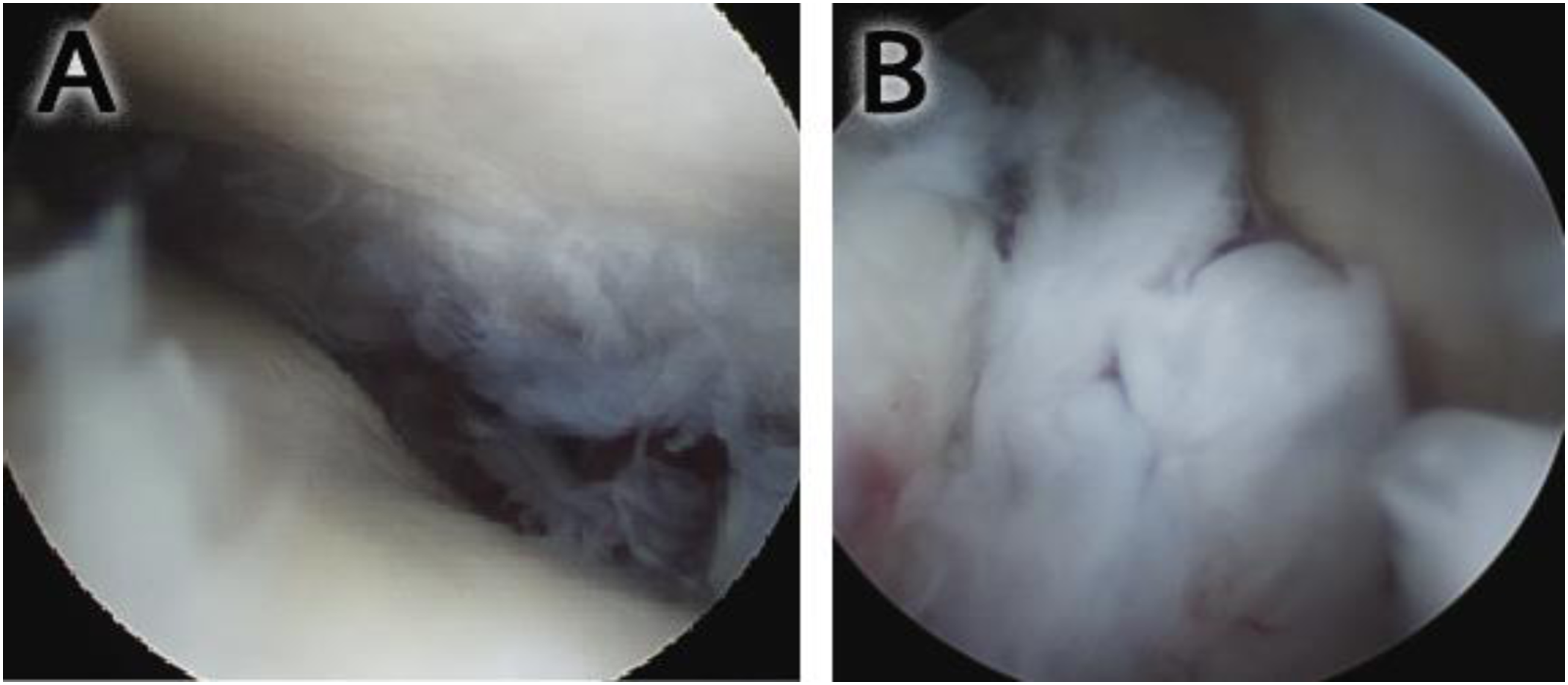
Open reconstruction with autograft
Autologous gracilis tendon graft is a good choice for its anatomic and mechanical characteristics of length and strength. The gracilis tendon length is sufficient and the thickness is generally sufficient for the purpose.
22
Different reconstructions are possible. Pisanu et al.
10
advise reconstruction of the superficial tibiocalcaneal band and the deep anterior tibiotalar band. Some repair the deep anterior tibiotalar ligament only.
11
The authors prefer to repair both the deep posterior and anterior tibiotalar band, as the combination might provide better stability in the axial and the coronal plane (Figure 6). In the setting of a planovalgus foot with subtalar dislocation the tibionavicular ligament and spring ligament should be assessed and potentially treated. The tibial footprint is made in the medial malleolus at the intercollicular groove, aiming at the anterior tibial crest. Based on which bands are reconstructed, the other footprints drilled; the free tendon graft should be fixed proximally with a suspensory fixation, for example the TightRope (Arthrex, Naples, Florida) and distally with two interference screws, for example Bio-Tenodesis Screws. Studies comparing repair techniques are lacking as they are hampered by the quantity of patients. Moreover variable baseline characteristics make comparison of repairs difficult, such as hindfoot alignment and the presence of osteoarthritis. The suture tape repair design: the goal is to restore the restraints on tilt and rotation of the talus in the ankle joint. Therefore, repair of the deep posterior deltoid band as well as a more anterior oriented tibiotalar band is advised. Tibiocalcaneal, tibiospring, and tibionavicular ligament reconstructions should be considered to augment the medial stability.
Arthroscopic technique
Via standard anterolateral and anteromedial arthroscopic portals, the scope is used to clean the joint and assess possible associated injuries. Medial instability should be confirmed arthroscopically. When lateral ligament instability is present as well, it is the advice of the authors to address this as well. 21 Subsequently, the deltoid repair is addressed: a medial anchor is inserted at the medial malleolus. The anatomical reference for this anchor is the intersection of the following two lines: a line parallel and at the level of the ankle joint, and a line perpendicular that intersects the tip of the lateral border of the medial malleolus. 21 The anchor is placed inferomedially into this intersection. Sutures are passed through the deltoid ligament, respecting the safe zone illustrated by. 23 The ankle is positioned in neutral (no posterior drawer) and the lateral sutures tightened with arthroscopic knots (if a lateral repair is done). Finally, the medial repair is finalized by tightening the deltoid sutures with the ankle still in neutral position.
In this specific example, an all inside technique is described addressing the deep deltoid only. In addition, to add to deltoid stability, the superficial bands of the deltoid can be repaired. In such a case the authors advocate an open approach.
Post operative regimen
Patients should be put in a walker boot. Common postoperative regiment includes non-weight bearing for one or 2 weeks after which progressive weight bearing can begin. The boot can be replaced by a rigid ankle brace after four to 6 weeks. This brace is used until 8 weeks full time and then progressively removed, but used for sports for several months more. Physical therapy is normally started at the second postoperative week, with restriction on inversion, eversion, or rotation until the sixth week mark. Patients are allowed to return to practice or baseline activities in a light manner after 3 months. Full return to competitive sport activity is generally allowed after 6–9 months.24,25
Additional procedures
Lateral ligament repair
As lateral ligament instability is present in the majority of cases, a reconstruction of the lateral ligamentous complex of the ankle should be considered. If the condition of the anterior talofibular ligament and calcaneofibular ligament allows an adequate primary repair, these ligaments are reconstructed by shortening and reinsertion. An augmentation with a tendon graft or internal brace should be performed, especially when ligamentous material present is not sufficient.
Flatfoot reconstruction
A flatfoot reconstruction should be considered if there is pre-existing valgus hindfoot and/or deformity of the forefoot. In patients with severe attenuation or defect of the tibionavicular, tibio-spring or spring ligaments these ligaments should be addressed as well.
Triple arthrodesis
A triple arthrodesis is considered when the medial ankle instability is so pronounced that a valgus tilt of talus within the mortise is seen on anteroposterior standard views of the ankle with the foot weight bearing. A calcaneus slide osteotomy might not be sufficient. Attention must be paid to fully correct the entire deformity.
Conclusions and limitations
The deltoid ligament is a complex structure on the medial side of the ankle joint which consists of multiple bands. It is widely accepted that the deltoid consists of a deep and superficial portion. The deep deltoid can be divided in two bands that only cross the tibiotalar joint, a large posterior band and a smaller anterior band. The superficial part of the deltoid fans out to the talus, calcaneus, spring ligament and navicular bone. It is debated whether these bands can seen separately, or that they are part of one structure. There is limited evidence showing that the deep bands control talar abduction as well as talar rotation in the ankle mortise. Of the superficial bands, the talocalcaneal band provides talar abduction restraint. The tibiospring and tibionavicular ligaments have a more complex restraint on the medial ankle, as the first forms a complex with the spring ligament and the latter also crosses the talonavicular joint.5,8 Further understanding in specific function of separate parts of the deltoid ligament is needed and might result in a better and more anatomical repair and reconstruction guidelines.
Whether the deltoid should be repaired in the acute setting, often the result of a multidirectional ankle trauma, remains a subject of debate. Large studies have not shown added value of direct repair of the deltoid, compared to nonoperative treatment of the deltoid with treatment the syndesmosis injury.14,26 One of the limitations of these studies is that a specific subgroup is not identified: patients with a significant pre-existing hindfoot valgus. They are considered prone to develop chronic deltoid insufficiency after deltoid ligament injury. Consequently, this subgroup might benefit from an aggressive approach in repairing the deltoid in combination with realignment of the hindfoot in the acute setting.
When regarding the repair of the deltoid ligament, multiple repair techniques are described. It remains unclear whether the use of autograft, allograft or suture tape augmentation is superior. Additionally, uncertainty exists to which bands of the deltoid should be addressed. Some authors advocate repairing the talocalcaneal band in combination with the deep anterior tibiotalar band. 10 Some repair the deep anterior tibiotalar ligament only. 11 The authors prefer to repair both the deep posterior and anterior tibiotalar band, as the combination might provide better stability in the axial and the coronal plane. In the setting of a planovalgus foot with subtalar dislocation, the tibionavicular ligament and spring ligament should be assessed and potentially treated.27,28
Studies comparing of repair techniques are lacking as they are hampered by the number of patients. Moreover variable baseline characteristics make comparison of repairs hard, such as hindfoot alignment and the presence of osteoarthritis.
The authors believe that deltoid repair with suture tape augmentation is warranted in patients with good tissue quality, as is the case in the acute setting (Figure 7). A full arthroscopic repair of the deltoid and lateral ligaments has shown promise. In patients with a high risk for wound complications, such as patients with diabetes, an arthroscopic technique might be beneficial. Intra operative images of direct deltoid ligament repair with suture tape augmentation. (a): the flexor retinaculum is identified and incised to create a flap that can be reattached. (b): position of the dorsal talar anchor. The ankle joint is visible, which has been treated with anteromedial debridement. (c): Drilling of the tibial tunnel at the intercollicular groove of the medial malleolus. Suture tape is visible protruding from the distal anchors, which were made the location of the insertion of the deep posterior deltoid as well as deep anterior deltoid ligament. (d): After deltoid repair; the fixation of the suture tape is not visible anymore as it is deep to the repaired deltoid tissue.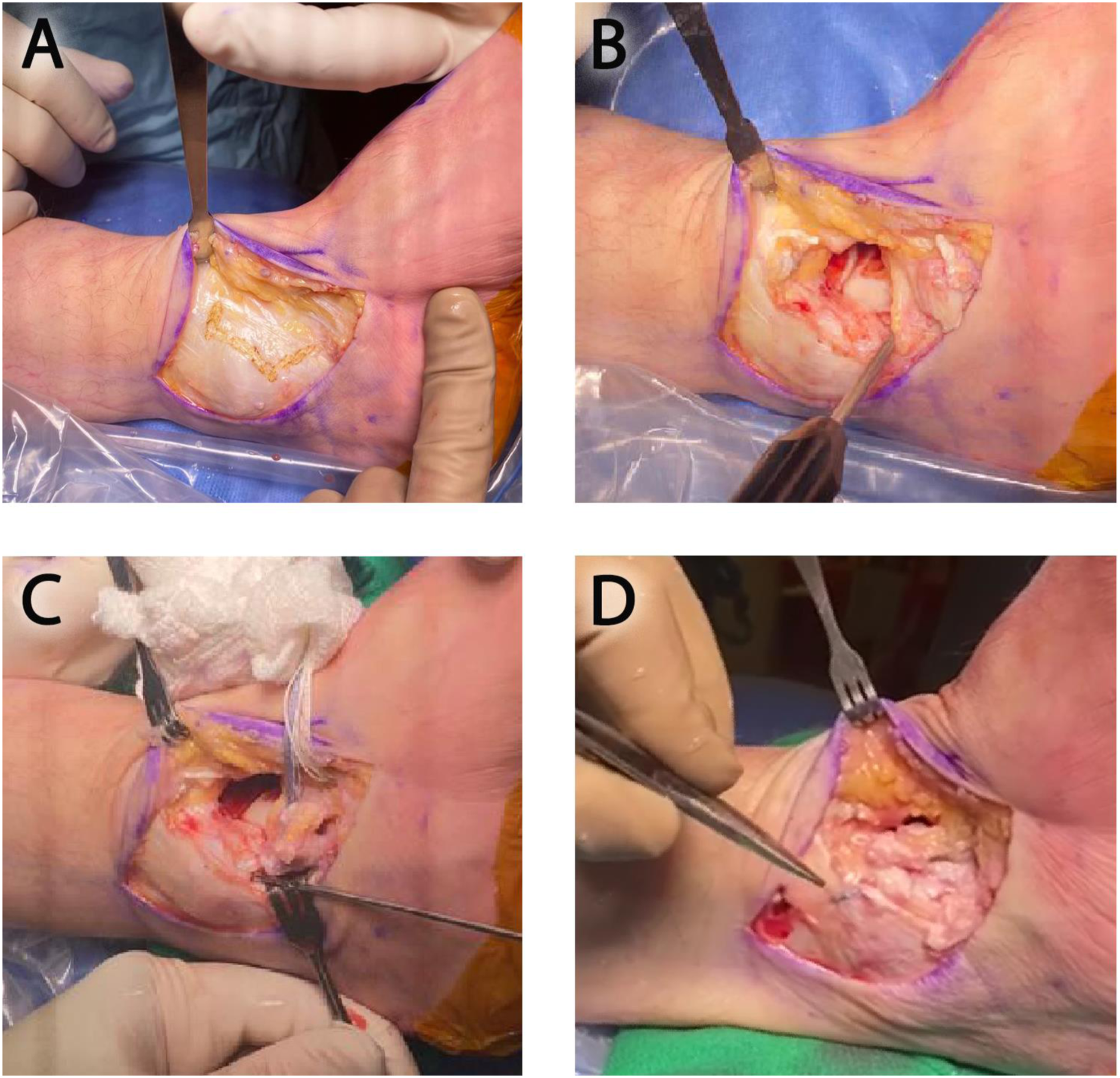
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.