
Abstract

Introduction
Triplane ankle fractures are unique ankle injuries that typically occur in adolescents aged 12-15 years as they approach skeletal maturity. 8 They account for 5% to 15% of pediatric ankle fractures. 10 These fractures follow a predictable pattern based on the order of closure of the distal tibia physis. 7 Over a period of 18 months, this physis closes from center to medial (antero- and posteromedial), and then lateral. 10 Therefore, a supination-external rotation injury can lead to a fracture propagating through the open lateral physis, involving the coronal, sagittal, and axial planes.7,10 Multiple fracture patterns were described but the basic configuration is an epiphyseal fragment anteriorly and metaphyseal fragment posteriorly. 1 Soft tissue entrapment has been described as a rare complication of complex adult ankle injuries, with a reported incidence of 10% to 15% in adult pilon fractures.2,9 Of these cases, the incidence of posteromedial neurovascular entrapment was 10% and presenting with varying degree with neurologic manifestations, most commonly plantar dysthesia. 2 The incidence of this complication is not well recognized in pediatric ankle fractures. This case report discusses an adolescent patient who had neurovascular compromise after a triplane fracture.
Case Report
An otherwise healthy 16-year-old male adolescent presented to the emergency department at an outside institution after sustaining a right ankle injury during a soccer game. He had a displaced triplane fracture (Figure 1). The foot had normal capillary refill but the posterior tibial (PT) and dorsalis pedis (DP) pulses were not palpable due to swelling. The patient had numbness to the plantar hallux. Active movement of the toes was not possible, due to pain. Attempted closed reduction led to further fracture displacement (Figure 2). After this reduction attempt, the patient lost sensation to the plantar hallux and his toes were colder than the contralateral side. A preoperative computed tomography (CT) scan was obtained (Figure 3, A-C). His fracture line propagated through the 3 planes. The patient had an anteriorly displaced distal fragment and a posteriorly based epiphyseal sagittal split. The patient was taken on an urgent basis to the operating room for open reduction, internal fixation of the fracture. A medial incision was used to expose, clean, reduce, and stabilize the fracture (ORIF) with a plate and screws including an independent anterior-to-posterior screw inserted through a separate small anterior incision. A lateral incision was used to perform ORIF of the fibula fracture (Figure 4). The operative note described entrapped periosteum in the fracture site but did not report entrapment of the neurovascular/tendinous structures. At the end of the procedure, the toes remained cold with no arterial Doppler signals in the PT or DP pulses. Doppler signals in anterior tibial and peroneal pulses were present. An urgent postoperative CT angiogram (CTA) showed a filling defect of the PT, with a sharp tortuous course at the fracture site (Figure 5). Because of ongoing neurovascular compromise, the patient was transferred to a Level 1 trauma center for a multidisciplinary team consultation including orthopaedic, plastic, and vascular surgery.
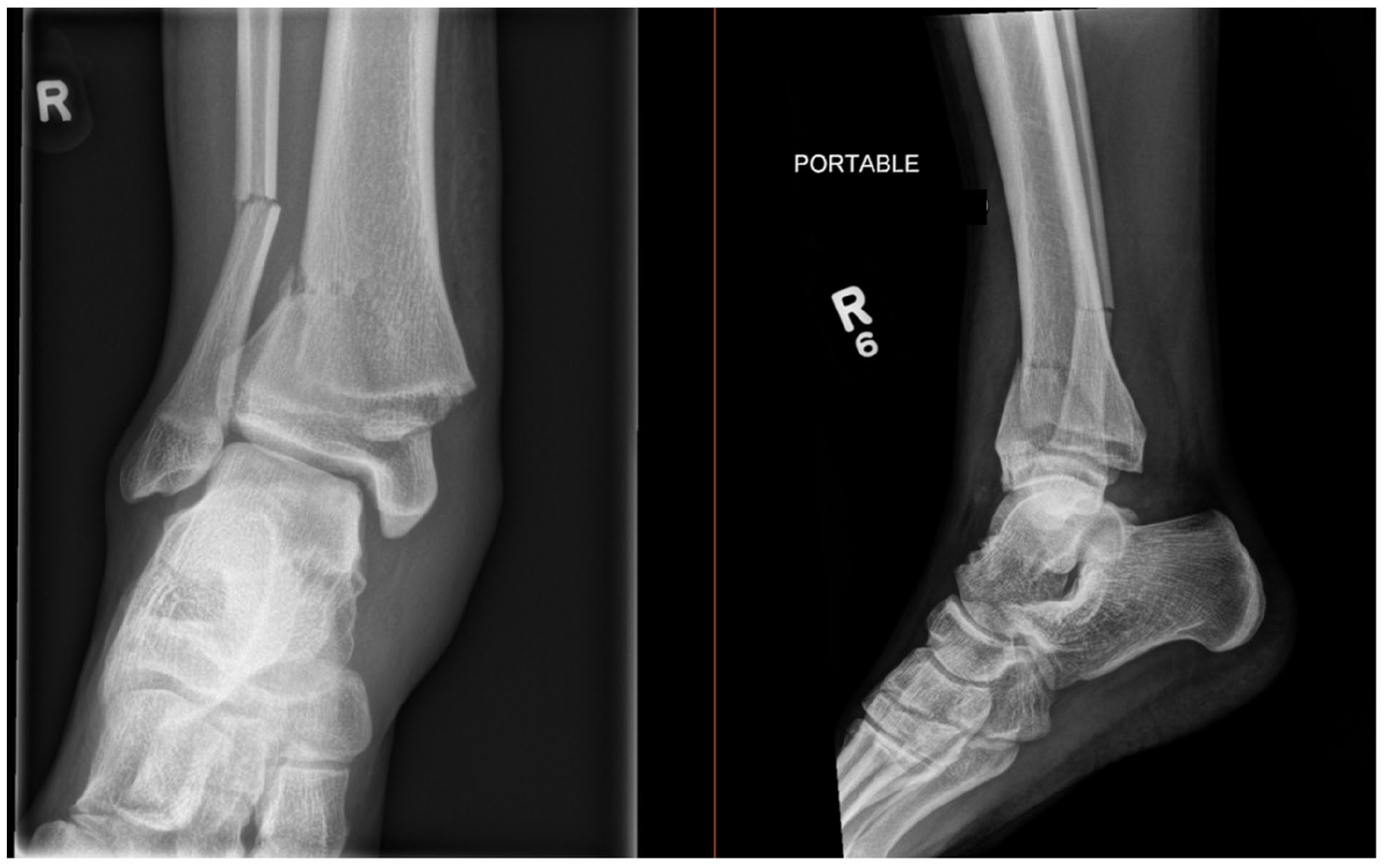
Initial plain radiographs showing injury pattern.

Post reduction plain radiographs demonstrating worsening in anterior displacement of the distal fracture segment.

(A) Selected sagittal and coronal cuts showing the fracture line propagating in the coronal, axial, and sagittal planes. (B) Three-dimensional (3-D) volume rendering computed tomographic (CT) scan cuts showing the fracture geometry. Selected cuts are anterior, posterolateral, and anteromedial. (C) Postreduction CT scan showing tibialis posterior (TP) and flexor digitorum longus (FDL) tendons in the fracture site. The neurovascular (NV) bundle is stretched at the periphery of the fracture site.
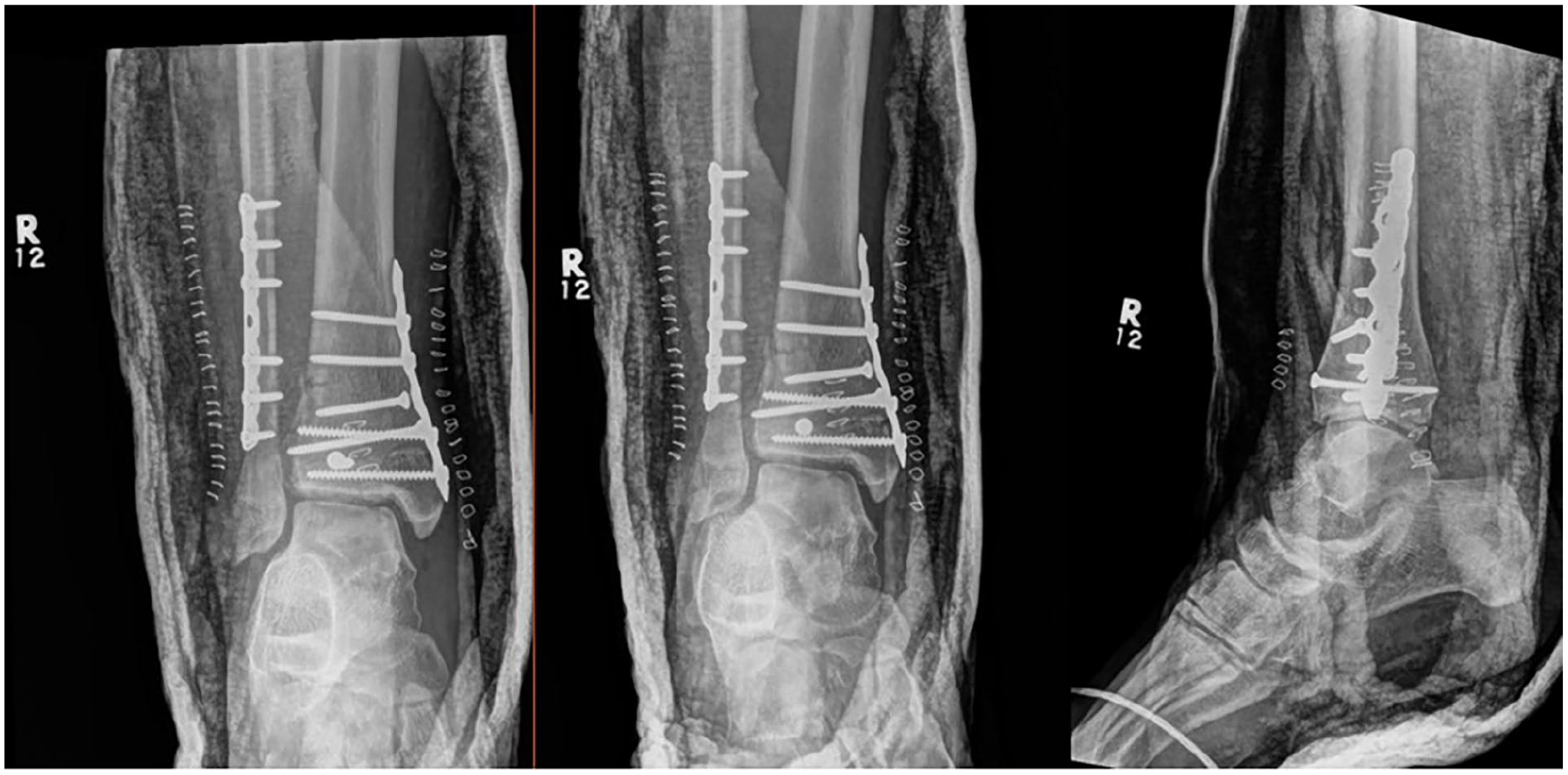
Plain radiographs after the first open reduction internal fixation.

Postoperative computed tomographic angiogram. Red arrows showing the tortuous course of the posterior tibial (PT) artery.
At the accepting center, the foot was tensely swollen with blisters (Figure 6). The patient had severe pain requiring ketamine infusion and had no sensation on the plantar forefoot with reduced sensation dorsally. Doppler signals were absent in PT and DP arteries. Based on these findings, a foot compartment syndrome diagnosis was made by the orthopaedic surgeon on call. The patient underwent urgent foot fasciotomies with 2 dorsal incisions.

Clinical image showing the medial, and to a lesser extent, the anterior wounds at the time of initial presentation to the trauma center. Medial-sided ankle and hindfoot swelling and blistering can be appreciated. This image was before the foot fasciotomy procedure.
Postoperatively, the patient continued to require ketamine infusion for pain. His sensory examination was unchanged. Further consultation with the orthopaedic trauma foot-and-ankle service was obtained and based on a retrospective review of the scans, it was believed that the medial tendinous/neurovascular structures (PT vessels, tibial nerve, and tibialis posterior [TP] and flexor digitorum longus [FDL] tendons) were entrapped in the fracture site (Figure 3, C). The patient went back to the operating room on an urgent basis (postinjury day 3) for exploration of the medial structures, and revision of fixation. The medial and small anterior ankle incisions were opened, and the hardware was removed. The posteromedial structures were absent from the area posterior to the tibia just above the ankle joint and replaced with blood clot (Figure 7, A). These structures were identified at the distal aspect of the tarsal tunnel with release of the flexor retinaculum and were traced proximal to the fracture (Figure 7, B). After distracting the fracture, the tendons of TP and FDL were found to be entrapped in the fracture site. The neurovascular structures (PT vessels and tibial nerve) were stretched and pulled over at a 90-degree angle at the fracture site but were not in the fracture site. An intraoperative Doppler examination of the PT artery showed a loss of signal at the fracture site. Intraoperative vascular consultation advised that the PT artery did not require exploration as the foot had adequate collateral circulation from the intact anterior tibial and peroneal arteries. The posteromedial structures were then reduced to the tarsal tunnel (Figure 7, C). The fracture was then reduced and fixed with 2.7-mm lag screws (Figure 8). A Hemovac drain and incisional vacuum-assisted closure were applied. The foot fasciotomy wounds were closed primarily. The ankle was splinted for 2 weeks. At 6 months postoperatively, the patient had a palpable DP pulse, regained normal sensation to the dorsum of his toes, improving motion of his ankle and toes, and subjective improvement in sensation on the plantar aspect of the forefoot. The tibial hardware was removed because of concern for infection; however, the intraoperative cultures came back negative. His fracture is healed (Figure 9).

Clinical images of the medial wound from the revision surgery after hardware removal. In all 3 images, north is anterior, south is posterior, right is cranial, and left is caudal. In image A, the Adson forceps point to a “bare area” posterior to the medial malleolus that is void of the medial structures. In image B, the Steven scissors point at the medial neurovascular bundle, which is heading distally. In image C, the arrow shows the medial tendons (tibialis posterior and flexor digitorum longus) after being reduced to their anatomic location posterior to the medial malleolus in the tarsal tunnel.
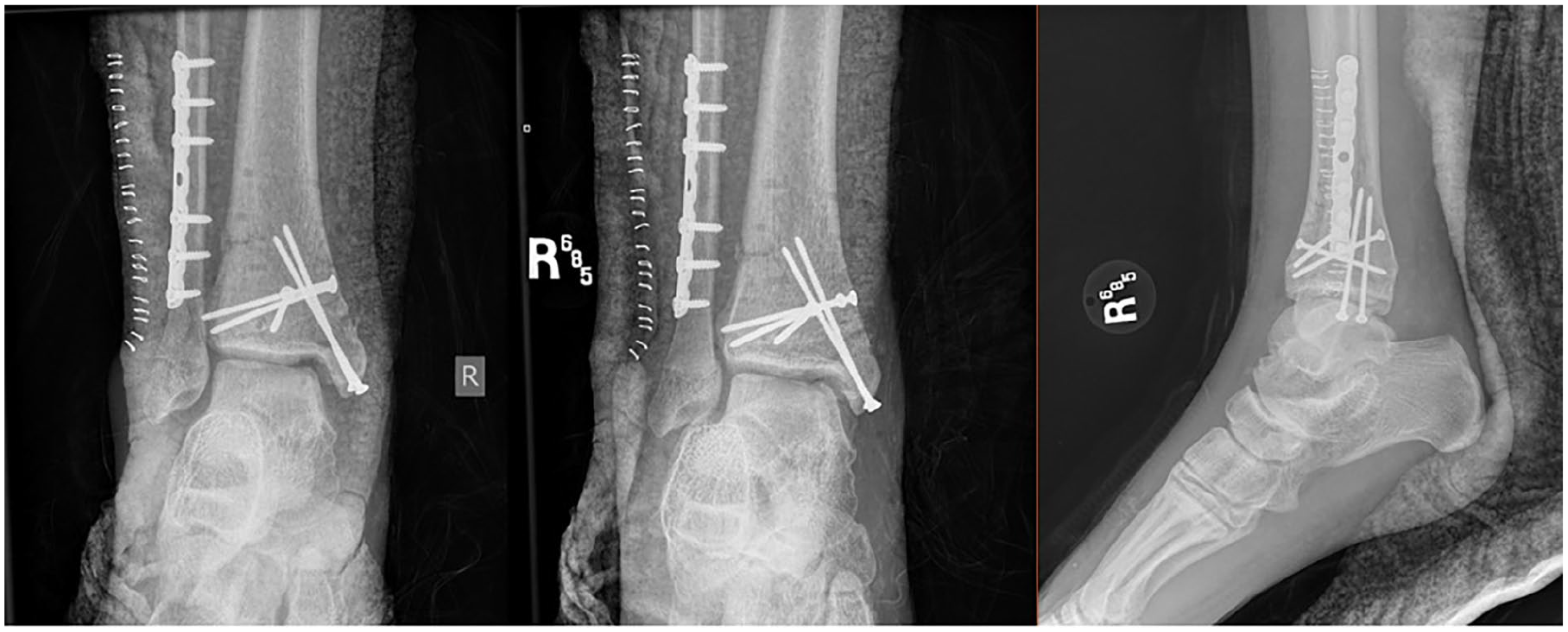
Plain radiographs showing the revision open reduction and internal fixation.
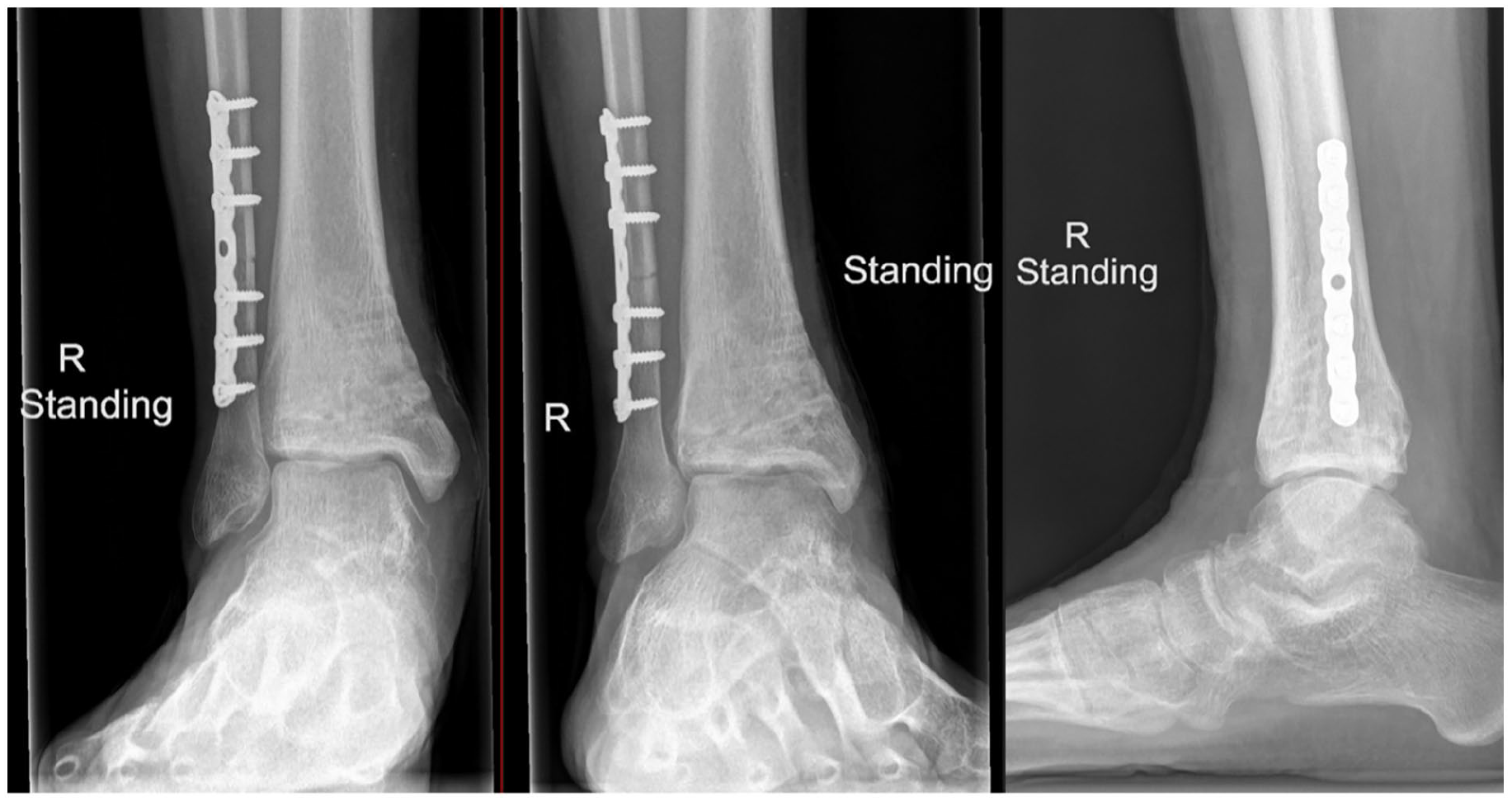
Plain radiographs showing union of the tibia fracture at 6 months postoperatively.
Discussion
This case report highlights the importance of a meticulous review of preoperative imaging, including CT soft tissue windows. Although entrapped periosteum is common in adolescent distal tibial physeal fractures, it is crucial to assess the other soft tissue structures that could potentially be involved. 6 In this case, TP and FDL tendons were caught in the fracture laterally, as well as pulling the tethered neurovascular bundle with them, causing traction neuropraxia and likely direct injury to the vessels, causing clot formation. In adults with similar injuries, neurologic symptoms substantially improved at 6 months but with some degree of altered plantar sensation. 2
The incidence of compartment syndrome of the foot after a pediatric ankle fracture fixation is unknown. Although others have reported this complication in skeletally mature patients, to our knowledge, no reports have described this phenomenon in skeletally immature patients.3 -5 Notably, in one report, the foot compartment pressures fell dramatically after opening the previous ankle wound and removing the subcutaneous sutures without the need for formal foot fasciotomy. 3 This suggests that tight closure of the soft tissue may play a role in venous occlusion with subsequent elevation in foot compartment pressures distally.
It is also worth noting that with marked bony injury, the soft tissue component can be overlooked. In a retrospective study of pilon fractures, only 20% of cases with soft tissue entrapment were identified by the attending radiologist. 2
Conclusion
Triplane ankle fractures typically occur in adolescents before physeal closure. Tendon and/or neurovascular entrapment may occur after a closed reduction of a displaced fracture. This may cause indirect traction injury to the neurovascular bundle. It is crucial to recognize this when analyzing preoperative imaging.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241310426 – Supplemental material for Neurovascular Compromise Post Triplane Fracture: A Case Report
Supplemental material, sj-pdf-1-fao-10.1177_24730114241310426 for Neurovascular Compromise Post Triplane Fracture: A Case Report by Humood Boqambar, Martin Kelly and David Stephen in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study because it is a case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.