
Abstract
Background:
Total ankle arthroplasty (TAA) is an effective treatment for severe end-stage ankle osteoarthritis (AO). Despite satisfactory results, range of motion (ROM) is still suboptimal compared to healthy ankles. This issue may stem from different conditions, and the difficulty in accurately restoring the height of the joint line may be one of them. Recent studies in TAA have demonstrated that an elevated joint line is associated with reduced postoperative ROM and poorer functional scores. To improve the accuracy of bone resection and implant positioning, the use of patient-specific instruments (PSIs) has been proposed. The aim of this study is to compare joint line height, ROM, and functional clinical outcomes between standard TAA and TAA using PSI.
Methods:
A retrospective analysis was conducted on a consecutive cohort of patients who underwent standard TAA and TAA with PSI between January 2020 and December 2022. Radiographic assessments, including measurement of joint line height ratio (JLHR) and ROM, were performed. The clinical outcome was assessed using the Forgotten Joint Score.
Result:
Fifty-one patients underwent standard TAA, whereas 13 received TAA with PSI. The mean JLHR preoperatively was 1.51 ± 0.24 and postoperatively was 1.56 ± 0.23 in the standard TAA group (P = .056). Conversely, the mean JLHR of PSI TAA group passed from 1.52 ± 0.19 to 1.41 ± 0.21 after TAA (P < .05). Although the postoperative joint line level in the PSI TAA group was lower compared with both the preoperative levels and the postoperative standard TAA group (P < .05), no significant differences were observed in ROM or clinical outcome scores at the mean 1-year follow-up.
Conclusion:
This study suggests that PSI may improve the accuracy of reestablishing this implant’s alignment closer to the native joint line. However, contrary to the study’s initial hypothesis, PSI was not associated with any difference in ROM or clinical outcomes compared with standard TAA technique. Additional factors including the prosthetic implant design, presence of heterotopic calcifications, soft tissue contracture, surgical technique, post-TAA tibial slope, and preoperative ROM may have a greater impact than joint line level.
Level of Evidence:
Level III, retrospective cohort study.
This is a visual representation of the abstract.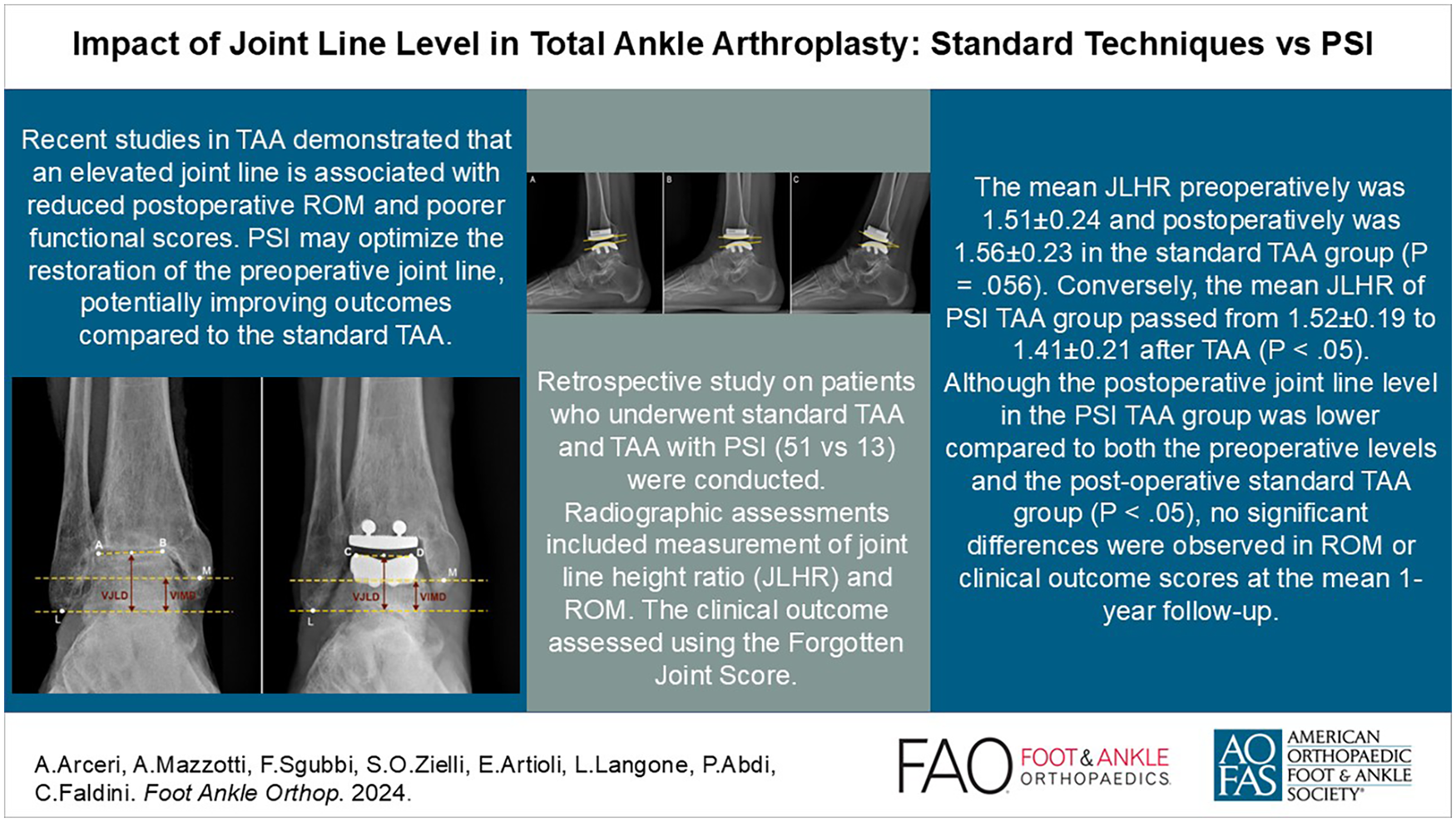
Introduction
Total ankle arthroplasty (TAA) is a well-established solution for the treatment of severe end-stage ankle osteoarthritis (AO). Although results are generally satisfactory in terms of pain relief, functional outcomes are still somewhat limited, particularly with regard to restoration of range of motion (ROM).1,3,8 This may be due to several conditions, including the challenge of restoring the correct center of rotation and joint line height, which are not systematically considered in planning with current prosthetic models and available instrumentation.
The importance of restoring the native joint line is recognized in various anatomical sites. As reported in the knee arthroplasty literature, it correlates with improved ROM and favorable clinical outcomes.5,15,24 In contrast, this concept is still getting started in TAA, with only a few limited studies addressing this topic.11,20 Current studies are aimed at finding a method to determine the height of the joint line in order to have a reference for restoring the native joint line. These radiographic measurement methods rely on anatomical landmarks in the ankle that remain consistent both before and after TAA. The simplest and most efficient method of assessing joint line height on radiographs is through the joint line height ratio (JLHR). 13
Existing literature suggests that ankles affected by end-stage OA are almost always posttraumatic23,25 and often exhibit an elevated joint line due to bony erosion, which persists after TAA as the degenerated joint line is used as a reference during bone cutting. 13 In support of this speculation, recent studies have shown that an elevated joint line is associated with reduced postoperative ROM and poorer functional scores.11,20
Theoretically, patient-specific instruments (PSI) application should improve accuracy in bone resection and implant positioning, then also optimize restoring the native joint lines by using a representation of the patient’s bony anatomy that enables the identification of osteophytes and the presence of bone deficits. This can facilitate planning the desired position and size of final implants based on constant anatomical landmarks, accounting for preoperative deformities. 16 Currently, there are no studies that have evaluated the joint line height of TAA with PSI.
Therefore, we hypothesized that the application of PSI in TAA, which potentially may optimize the restoration of the preoperative joint line, may lead to improved ROM and superior clinical outcomes compared with the standard TAA technique. The purpose of this study is to evaluate the joint line height in standard TAA vs TAA with PSI, comparing its impact on ROM and clinical outcomes.
Methods
With institutional review board approval (protocol no. 0000084), a retrospective study was conducted using our institutional database of all patients who underwent standard TAA or TAA with PSI from January 2020 to December 2022. As a result, 2 groups were formed for comparison purposes. The study followed the STROBE statement and checklist for retrospective studies. 26
Patient Selection
Patients undergoing TAA with at least 1 year of radiographic follow-up were included. The minimum radiographic follow-up selected was based on previous research suggesting that there is no substantial improvement in ROM beyond 6 months post-TAA. 1
Exclusion criteria included conditions or procedures potentially affecting bony landmarks for JLHR calculation, such as bony defects of the malleoli, radiographic component loosening, cases with severe varus/valgus deformities (more than 10 degrees) affecting the tibial plafond, and in the presence of tibiotalar incongruence. Cases with less than 1 year of follow-up, incomplete radiographs, and tendon-lengthening procedures that could influence ROM assessment were also excluded.
All patients gave written informed consent, and the study adhered to the tenets of the Declaration of Helsinki.
Surgical Technique
All TAAs were performed by 2 experienced foot and ankle orthopaedic surgeons, with one exclusively using the standard technique and the other using only the PSI approach. Because of the nature of the procedures, the surgeons were necessarily aware of the technique they were applying, but efforts were made to maintain masking in the scoring process. Radiographic assessment was performed twice by an independent trained foot and ankle orthopaedic surgeon and a resident orthopaedic surgeon who were not the surgeons for the 2 patient cohorts, and clinical scoring was performed by orthopaedic residents, both masked to the surgical technique used. This strategy was implemented to ensure an objective comparison of the outcomes between the 2 surgical techniques.
Standard TAA was performed using mobile bearing FAR prosthesis (AdlerOrtho, Milan, Italy) through an anterior approach. The talar and tibial resection was performed using conventional tibial alignment jig and cutting blocks, followed by the insertion of cementless talar and tibial components, along with the ultrahigh-molecular-weight polyethylene meniscus. In the standard TAA technique, the primary goal was to achieve proper alignment and minimize bone resections, essentially functioning as a resurfacing procedure. However, the intraoperative reference points were largely operator-dependent, relying heavily on visual orientation using conventional tibial alignment jig. Additionally, the preoperative planning could not be accurately translated into reproducible landmarks using the standard instrumentation, which limited the precision of the joint line determination and implant positioning.
TAA with PSI, using the same implant, required preoperative images from a CT scan to create a 3D model of the ankle. Using a 3D CAD software the mechanical axis of the leg, from the tibial tubercles down to the center of the tibiotalar joint, was identified, and based on this axis, the anteroposterior and midlateral planes was determined. Virtual TAA was then performed by aligning the tibial component in the coronal and sagittal planes. The implant was positioned to match the medial corner of the tibial groove while preserving the medial and lateral malleoli. The talar implant was set to follow the curvature of the talar dome, maximizing bone coverage without overhang, and ensuring a minimum resection depth of 4 mm. Once the correct positioning has been established, custom cutting guides were designed based on these parameters and the patient’s anatomy to ensure precise and safe bone cuts during surgery. The surgeon then reviewed the report and could approve or request changes before the cutting guides were manufactured. The implant was set using the cutting guides via an anterior approach, preserving necessary osteophytes to follow the tactile feedback. Distal tibial and talar resection was executed using patient-specific guides.9,10 The joint line height in the PSI approach was defined indirectly, with the preoperative planning aiming for the same goals as the standard technique—correct alignment and minimal bone resection.
In both cases, the ankle was immobilized in a plaster cast for 3 weeks, and no weightbearing was allowed. After cast removal, progressive weightbearing in a walking boot was allowed and active and passive flexion-extension mobilization of the ankle within pain-free limits was encouraged. 17 A physical therapy protocol was then initiated, focusing on restoring functional ROM, ankle stability with balance and proprioception training, strengthening the operated ankle, and reeducating the patient on proper gait mechanics.
Radiographic Assessment
Each patient underwent routine pre- and postoperative weightbearing anteroposterior and lateral radiographs. In addition, postoperative lateral radiographs in maximum ankle flexion-extension were performed for all patients. Radiographic assessments were performed twice by a trained foot and ankle orthopaedic surgeon and a resident orthopaedic surgeon, using the hospital’s imaging archiving system.
The JLHR was calculated on weightbearing anterior-posterior ankle radiographs, before and after surgery (Figure 1), employing a methodology outlined in previous literature. 13 Elevated JLHR values correspond to an elevated joint line level.
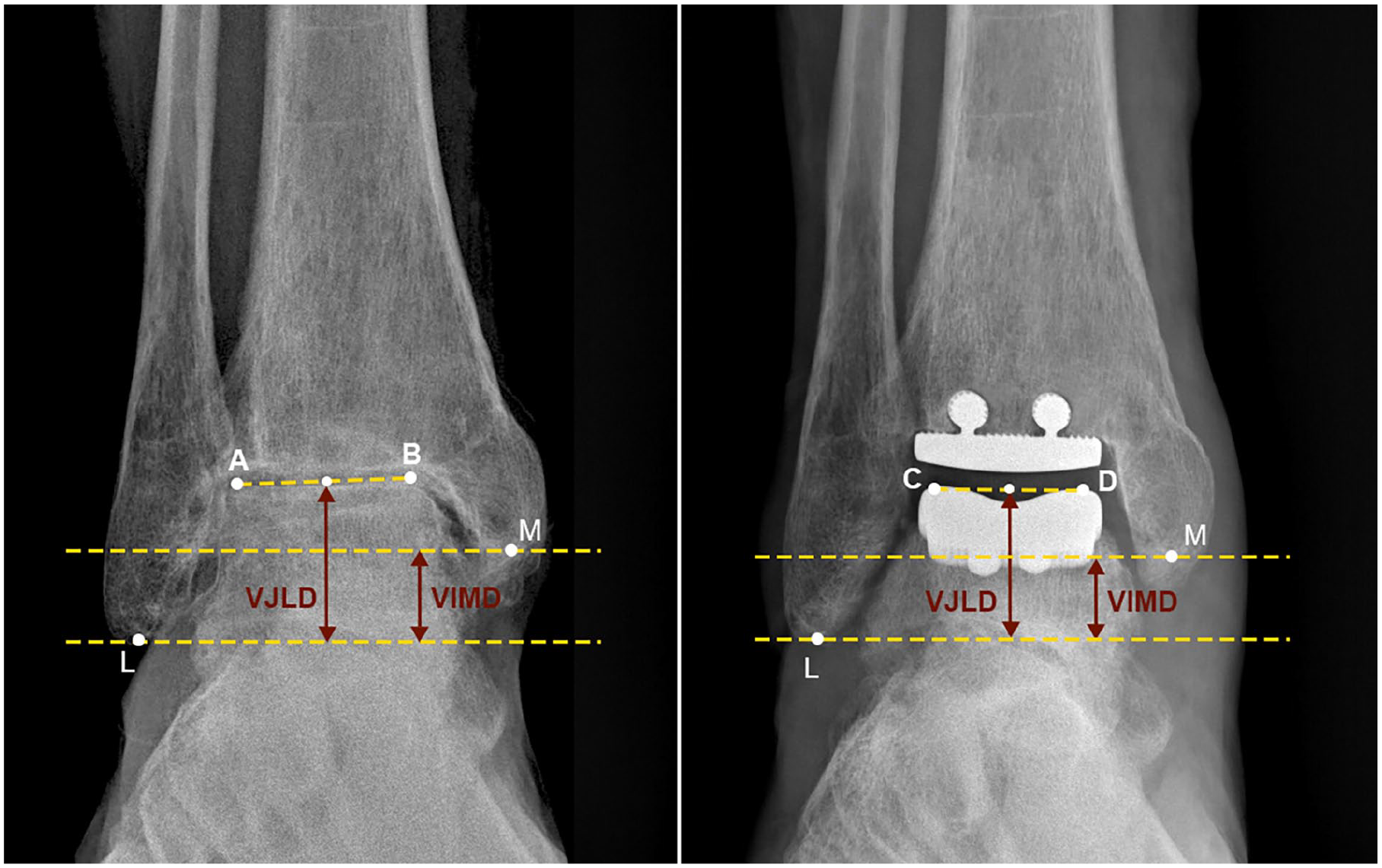
Measurement of the joint line height ratio (JLHR) on anteroposterior radiographs involves calculating the ratio of the vertical joint line distance (VJLD) to the vertical intermalleolar distance (VIMD). The VJLD is determined by drawing a horizontal line from the tip of the fibula (L). Another line is drawn between the most lateral (A) and medial (B) points of the talar trochlea preoperatively, or the uppermost points (C and D) of the talar component postoperatively. VJLD is the length of the perpendicular line drawn from the midpoint of AB to the intersection of the line passing through L. VIMD is the length of the perpendicular line connecting 2 horizontal parallel lines, one passing through L and the other passing through the posterior colliculus of the medial malleolus (M).
The tibial lateral surface (TLS) angle was also measured on lateral radiographs using a method validated in the literature, 18 with the aim of incorporating it as a parameter in the multivariate linear regression analysis. The TLS angle is defined as the intersection of the distal tibial mechanical axis and the line passing through the flat portion of the tibial component. The distal tibial mechanical axis was measured with 2 circles fitting between the anteroposterior tibial cortices 5 and 10 cm above the joint line and a line was drawn to connect the centers of both circles, extending distally to the most distal point of the component. The second line was drawn across the top of the tibial component baseplate.
Postoperative ankle ROM, including maximum dorsiflexion, maximum plantarflexion, and total ROM, was assessed using established methods. 6 Specifically, the Cobb angle was measured between a line drawn across the top of the tibial component baseplate and a second line drawn beneath the anterior and posterior aspects of the talar component on lateral radiographs (Figure 2).

Measurement of postoperative (A) dorsiflexion, (B) neutral position, and (C) plantarflexion on lateral view radiographs to calculate the total tibiotalar range of motion.
Clinical Outcomes Assessment
Patient demographics and surgical details were extracted from the medical records by manual review. Demographic information included age, gender, OA etiology, and OA onset, whereas surgical details included the type of implant and the use of PSI.
OA onset was defined as the time that elapsed between the onset of functionally limiting ankle symptoms and TAA surgery.
Before surgery and during follow-up visits, all patients completed the Forgotten Joint Score (FJS), a patient-reported outcome measure developed to assess joint awareness following joint replacement surgery. Originally validated for hip arthroplasty, the FJS has recently been validated for use in ankle arthroplasty as well. 19 Unlike traditional outcome measures that focus solely on pain and function, the FJS evaluates the patient’s ability to forget about their replaced joint during daily activities, indicating a high level of satisfaction and function. The FJS consists of a series of 12 questions that inquire about the patient’s awareness of their replaced joint during various activities, such as walking, standing, climbing stairs, and doing household chores. Patients rate their responses on a Likert scale ranging from 0 to 100, with higher scores indicating a greater ability to forget about the replaced joint and, consequently, better function and satisfaction. 19
Statistical Analysis
Data collection was carried out using Microsoft Excel 365 (Microsoft Corporation, Redmond, WA) for Windows 11 and statistical analysis was performed using the software Jamovi project (2022), version 2.3.
The calculation of the sample size was not feasible because of the lack of direct comparative studies in the literature addressing joint line levels specifically for the PSI group.
Information retrieved from patient, operative, and outcomes were reported using descriptive statistics. Continuous variables were reported as mean and SD. The Shapiro-Wilk test was used to analyze variables for normality. The agreement between 2 graders for JLHR measurements was assessed using the intraclass correlation coefficient (ICC) with a 2-way random effects model. The ICC was 0.78 (95% CI: 0.75-0.81), indicating good interobserver reliability. Although this value does not reach the level of “excellent” reliability (commonly ICC > 0.90), it demonstrates a substantial level of consistency between the 2 observers. Given this, the average of the 2 raters was used for further analysis to ensure robust estimations of the JLHR measurements.
Differences in continuous variables between pre- and post-TAA JLHR and clinical outcomes were analyzed using a paired Student t test, whereas the independent Student t test was used to analyze changes in continuous variables between the 2 groups (standard TAA and TAA with PSI). The correlation between post-TAA JLHR with post-TAA ankle total ROM, dorsiflexion, plantarflexion, and 1-year postoperative FJS was assessed using the Pearson correlation coefficient (rho). Moreover, the same method was used to perform a correlation analysis between post-TAA ROM, dorsiflexion, and plantarflexion with 1-year FJS scores.
Multivariable models were used to investigate the association of post-TAA total ROM, dorsiflexion, and plantarflexion as outcome, respectively, for postoperative JLHR and potential confounding factors such as age, etiology, TLS, and OA onset.
Statistical significance was set at P value less than .05 per standard convention.
Results
Population
From a chart review, 122 patients who had undergone TAA were identified. Out of these, 64 patients fulfilled the selection criteria and were included in the study (Figure 3). Of the 58 excluded patients, 24 had malleolar bone defects, 12 had undergone concomitant Achilles tendon lengthening, 17 had severe deformities or tibiotalar incongruence, and the remaining 5 cases met multiple exclusion criteria simultaneously.

Flow diagram of the study cohort.
The study involved 64 patients who underwent TAA. Out of these, 51 patients received standard TAA, whereas 13 patients underwent TAA with PSI. No patients were lost to follow-up. There was no significant age difference between the standard TAA group and the PSI group (59.9 ± 10.3 years vs 55.6 ± 12.1 years, P = .344). Both groups had a higher proportion of females (34 of 51 in the standard group, and 8 of 13 in the PSI group). Most cases were secondary OA (47 in the standard group and 11 in the PSI group), with only a few cases of primary OA (2 in the standard group and 1 in the PSI group) or rheumatoid arthritis (1 in each group). There was 1 case of OA secondary to clubfoot in the standard TAA group. No significant difference in OA onset was observed between the 2 groups (5.6 ± 4.7 years vs 6.7 ± 4.5 years, P = .543). The mean follow-up was 29.5 ± 11.6 months.
Comparison of Standard and TAA Using PSI Related to JLHR, ROM, and Clinical Outcomes
The analysis showed a statistically significant change in the postoperative JLHR only in the PSI group, demonstrating a significantly lowered joint line compared with the standard TAA group (Table 1). A lowered joint line was observed in 24 of 51 patients (47.1%) in the standard TAA group and in 10 of 13 patients (76.9%) in the PSI TAA group. No other significant differences regarding ROM and FJS outcomes were found (Table 1).
Comparison of Standard and PSI TAA Regarding ROM and FJS Outcomes.

Abbreviations: FJS, Forgotten Joint Score; PSI, person-specific instruments; JLHR, joint line height ratio; ROM, range of motion; TAA, total ankle arthroplasty.
Statistical significance (P < .05).
Preoperative and Postoperative JLHR and Clinical Outcomes
In the standard TAA group, the mean JLHR was 1.51 ± 0.24 preoperatively and 1.56 ± 0.23 postoperatively (P = .056). In contrast, the PSI TAA group exhibited a mean JLHR of 1.52 ± 0.19 preoperatively and 1.41 ± 0.21 postoperatively (P < .05) (Table 2). Additionally, significant differences were observed in the mean FJS values between the preoperative and postoperative periods in both groups (Table 2).
Comparison of Preoperative and Postoperative JLHR and FJS Outcomes.

Abbreviations: FJS, Forgotten Joint Score; JLHR, joint line height ratio; PSI, person-specific instruments; TAA, total ankle arthroplasty.
Statistical significance (P < .05).
JLHR, ROM, and Clinical Outcomes Correlation
No correlation was found between post-TAA JLHR with post-TAA total ankle ROM, dorsiflexion, plantarflexion, and 1-year postoperative FJS scores. Similarly, no correlation was observed between post-TAA ROM, dorsiflexion, and plantarflexion with 1-year FJS scores in either the standard TAA group or the PSI group (Table 3).
JLHR, ROM, and FJS Pearson Correlation for Standard TAA and PSI.

Abbreviations: FJS, Forgotten Joint Score; JLHR, joint line height ratio; PSI, person-specific instruments; ROM, range of motion; TAA, total ankle arthroplasty.
Multivariable Linear Regression Model
Regression analysis revealed no association between postoperative JLHR with post-TAA total ROM, dorsiflexion, and plantarflexion (Table 4). Conversely, an association was identified between post-TAA total ROM and plantarflexion with TLS and also with OA onset (Figure 4).
Multivariable Linear Regression Models With Postoperative Ankle Total ROM, Dorsiflexion, and Plantarflexion.

Abbreviations: JLHR, joint line height ratio; PSI, person-specific instruments; ROM, range of motion; TLS, tibial lateral surface angle.
Statistical significance (P < .05).

Scatterplots with postoperative ROM as the outcome. (A) No association was found between postoperative total ROM and postoperative JLHR. An association was found between post-TAA total ROM and both (B) TLS and (C) OA onset. (D) In addition, post-TAA plantarflexion was associated with TLS. JLHR, joint line height ratio; OA, osteoarthritis; ROM, range of motion; TAA, total ankle arthroplasty; TLS, tibial lateral surface angle
Discussion
This study aimed to evaluate the joint line height in standard TAA vs TAA with PSI, comparing them with ROM and clinical outcomes.
The introduction of the JLHR has provided a reliable measurement technique for assessing the height of the ankle joint line on commonly available standard ankle radiographs using consistent bony landmarks. The main advantage is that measurements are expressed as ratios without requiring calibration markers, rather than as absolute values. This helps to minimize potential discrepancies arising from magnification effects. 13 In addition to recognized limitations such as malleolar bone defects and its challenging clinical interpretation, which does not offer a directly actionable measurement during surgery, this measurement has other limitations not addressed in previous studies, specifically in cases of severe varus and valgus deformities affecting the tibial plafond and in the presence of tibiotalar incongruence, which prevented us from calculating the joint line height. These conditions can distort the anatomy and create anatomical heterogeneity within the sample, making it difficult to measure the joint line height accurately. In particular, severe deformities and talar tilt can significantly influence postoperative outcomes because of the increased surgical complexity they present. These cases often require additional procedures such as tendon lengthening, osteotomies, or ligament rebalancing, which could affect postoperative ROM. Therefore, excluding these variables allowed us to minimize confounding effects and focus on the direct relationship between joint line height and functional outcomes, improving the validity of the study’s findings.
After TAA, the postoperative joint line level was significantly lower in the PSI group compared with the standard TAA group. Consequently, the joint line was higher in the standard TAA group, and although the mean change in joint line level from pre- to postoperatively approached significance, it was not statistically significant. These findings suggest that PSI may improve adherence to preoperative planning, potentially leading to greater accuracy in prosthetic positioning and preservation of the preoperative joint line. However, it is essential to recognize that the joint height of an arthritic ankle tends to be always higher compared with the healthy contralateral ankle. 13 Theoretically, CT scan of the healthy contralateral ankle as a reference for the TAA on the affected side could potentially allow the native joint line to be restored. In this context, lowering the joint line level to restore the native joint line is a challenging task. The arthritic process develops over years, and the soft tissues adapt to the evolving condition, often resulting in contractures in muscles, tendons, ligaments and capsules that complicate any lengthening attempts and may contribute to postoperative stiffness and reduced joint ROM. 20
Despite this speculation, the literature suggests that a higher joint line correlates with limited dorsiflexion and total ROM.11,20 A plausible explanation for reduced dorsiflexion following joint line elevation could be attributed to dysfunction of the preload mechanism due to redundant and inefficient tendons, limiting their ability to generate force. This could be true for active dorsiflexion but given the current method of motion measurement used in these studies, where passive ROM was calculated, this relationship is still unclear, as is why dorsiflexion was influenced by JLHR. The results from our cohort study supported this critique and, conversely with previous studies, revealed no correlation between higher joint line and limited dorsiflexion. Actually, the standard TAA group was characterized by a higher joint line level compared to the PSI group, which was lower and then closer to the native joint line level, but no correlation with postoperative ROM or outcomes was detected in either the standard TAA group or the PSI group. To date, comparative studies regarding ROM between standard TAA and PSI TAA are lacking, making it challenging to draw definitive conclusions based exclusively on these findings.
Furthermore, although there was a correlation between joint line height and ROM in previous studies, regression analysis of these papers suggest only a modest association between JLHR and postoperative dorsiflexion: post-TAA dorsiflexion was 0.5 degrees lower in a patient for a 0.1-unit increase in JLHR. 20 This suggests that although joint line is a potential factor influencing ROM, additional factors such as prosthetic implant design, 21 reduced radius of curvature compared to the arthritic talus, 27 heterotopic calcifications, 4 soft tissue contracture, 2 and surgical approach 14 could play a more significant role; thus, further investigation of these numerous other variables is warranted.
Our study reported that the TLS can influence total ROM, particularly plantarflexion. This is likely because an excessive tibial slope after the tibial cut can result in posterior mechanical obstacle, limiting plantarflexion. Additionally, the association between ROM and the AO onset supports the hypothesis that joint disuse leads to tendon retraction and muscle atrophy, which subsequently affect residual ankle movement after TAA implantation. This observation indirectly confirms that TAA has limited potential to improve preoperative ankle motion, as the outcome is highly dependent on the preoperative range of motion, 22 as also demonstrated in Palma’s multivariate analysis. 20
Postoperative ROM following TAA showed a correlation with clinical outcome scores.3,7 The current literature is poor on the comparison of clinical outcomes between standard TAA and PSI.2,12,28 Although the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score is not a validated scoring system, it is the most commonly used, but results based on this score have been inconsistent in the literature: one study reported a slight improvement in AOFAS scores for the PSI group, 12 whereas another study found no significant difference in AOFAS scores between the 2 cohorts. 2 Furthermore, no significant differences were observed in Manchester-Oxford Foot Questionnaire, Ankle Osteoarthritis Scale (AOS), or EuroQol–5 Dimensions scores. 28 Our study showed no differences in FJS between the 2 groups. Given the wide variability of clinical and functional scores used in the literature, making comparisons with existing studies proves challenging.
Hence, TAA with PSI, which, on average, was associated a lower joint line level compared with standard TAA techniques, demonstrated potentially better accuracy in bone resections, and improved bone preservation, superior resurfacing attitude, and more precise implant positioning. This brought the implant closer to the preoperative joint line, potentially approximating the native joint line. However, contrary to the study’s initial hypothesis, the effects on ROM and clinical outcomes were nonsignificant, raising questions about the value of restoring joint line height.
There are some limitations, including the absence of preoperative ROM data, unequal sample size, relatively small sample size in the PSI group. This was largely because of the low frequency of these specialized procedures. Although 2 different surgeons performed the 2 procedures, it is important to note that both surgeons trained at the same institution, have a comparable volume of experience, share the same surgical goals and techniques, and use the same implant. Thus, any potential bias related to the involvement of different surgeons is mitigated by their closely aligned approaches. Furthermore, our study used stringent inclusion and exclusion criteria to minimize confounding factors and increase the reliability of the results. The smaller sample size reflects both the rarity of the procedure and our commitment to maintaining rigorous methodologic standards. However, we acknowledge the potential limitations in statistical power. Moreover, cases with more severe deformities (less than 10 degrees in any case, respecting the exclusion criteria) were treated with PSI, potentially leading to a nonhomogeneous patient sample. In light of these limitations, the current findings do not allow for definitive conclusions and should be interpreted with caution. Despite these limitations, the study methodology included strict patient selection criteria to mitigate the influence of potential confounders and eliminate several confounding variables that may have influenced previous studies results, such as severe deformities, tibiotalar incongruence, and variability in implant types.
Conclusions
This study suggests that PSI may improve the accuracy of reestablishing this implant’s alignment closer to the native joint line. However, contrary to the study’s initial hypothesis, PSI was not associated with any difference in ROM or clinical outcomes compared with standard TAA technique. Additional factors including the prosthetic implant design, presence of heterotopic calcifications, soft tissue contracture, surgical technique, post-TAA tibial slope, and preoperative ROM may have a greater impact than joint line level.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241303474 – Supplemental material for Impact of Joint Line Level in Total Ankle Arthroplasty: Standard Techniques vs Patient-Specific Instruments
Supplemental material, sj-pdf-1-fao-10.1177_24730114241303474 for Impact of Joint Line Level in Total Ankle Arthroplasty: Standard Techniques vs Patient-Specific Instruments by Alberto Arceri, Antonio Mazzotti, Federico Sgubbi, Simone O. Zielli, Elena Artioli, Laura Langone, Pejman Abdi and Cesare Faldini in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval and informed consent statements
Ethical approval for this study was obtained from Institutional Review Board CE AVEC 370/2022/Oss/IOR (Rizzoli Orthopaedic Institute, Bologna, Italy)—protocol number: 0008996—approval date May 31, 2022. The study was conducted according to the guidelines of the Declaration of Helsinki. All patients gave a written consent to participate.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication has been financed with the support by Ministero della Salute 5×1000 fund raising campaign 5xmille 2021 contributions to the IRCCS, Istituto Ortopedico Rizzoli.
Consent to publication
All the patients provided their written informed consent at admission on data collection.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.