
Abstract
Background:
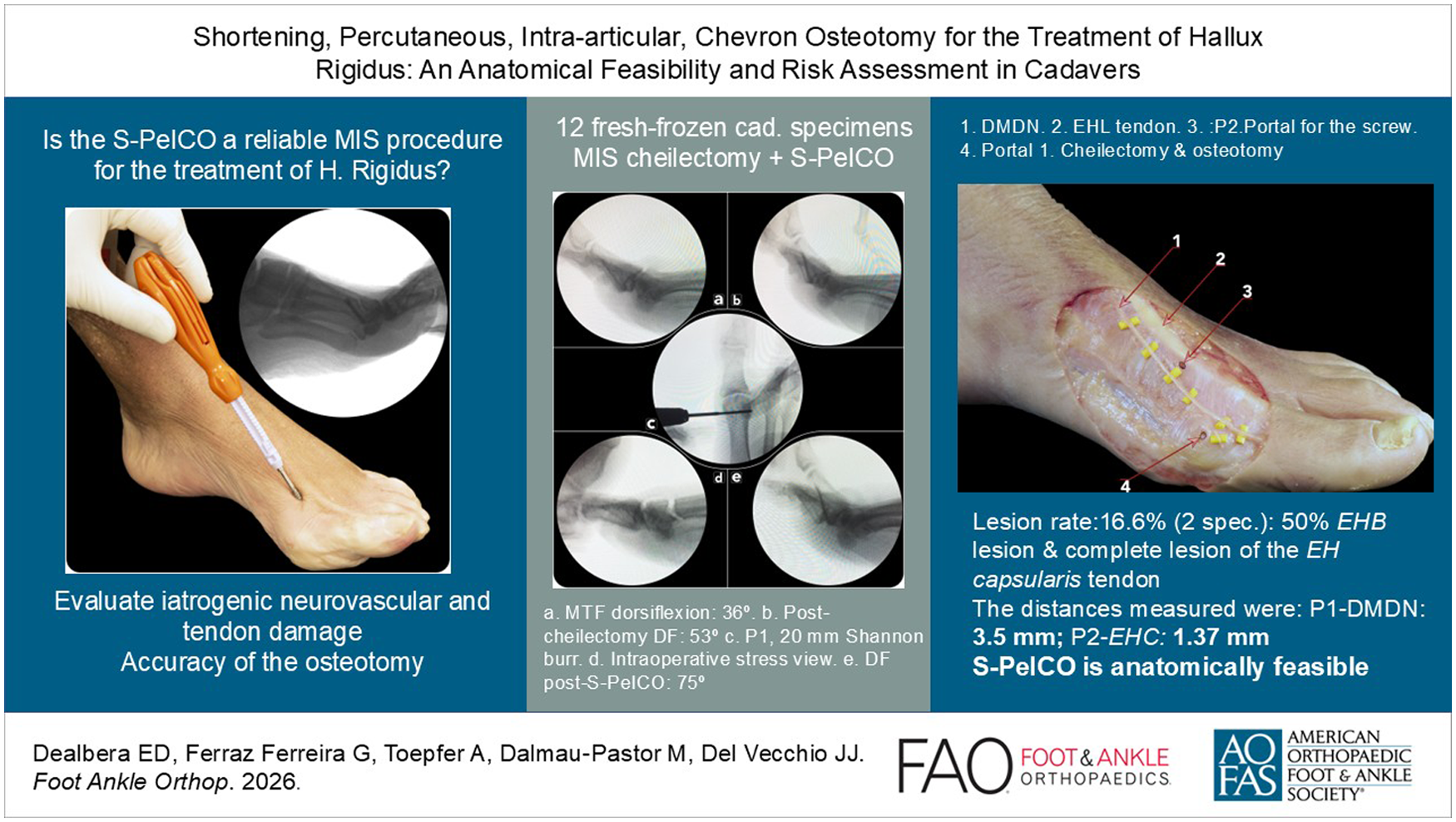
Hallux rigidus is a degenerative condition affecting the first metatarsophalangeal joint. Depending on symptoms, treatment options for symptomatic hallux rigidus include joint resection (such as arthrodesis or arthroplasty) or joint-preserving procedures (like cheilectomy or osteotomies). We present a shortening percutaneous, intra-articular, chevron osteotomy (S-PeICO) technique, which is a modification of the percutaneous intra-articular chevron osteotomy (PeICO) technique previously used to treat hallux valgus. The purpose is to evaluate iatrogenic neurovascular and tendon damage, as well as the accuracy of the osteotomy, including angulation and completion.
Methods:
Twelve fresh-frozen below-the-knee cadaveric specimens were used in this study and diagnosed with Coughlin grade I to III hallux rigidus and mild hallux valgus. To evaluate the procedure’s safety, the following data were collected: (1) distance between portal 1 and dorsomedial digital nerve, (2) distance between portal 2 and the medial border of the extensor hallucis longus tendon, (3) distance between portal 2 and the dorsomedial digital nerve, (4) distance between portal 2 and the extensor hallucis capsularis, (5) distance between portal 1 and the metatarsophalangeal joint, and (6) distance between portal 2 and the metatarsophalangeal joint. Additionally, the angulation and completion of the osteotomy in the sagittal plane were evaluated.
Results:
No significant iatrogenic injuries were detected. The occurrence of minor lesions was 16.6% (2 specimens): one showed a 50% extensor hallucis brevis lesion, and another experienced a complete rupture of the extensor hallucis capsularis tendon. The smallest average distances were observed between portal 1 and dorsomedial digital nerve (3.5 mm) and portal 2 and extensor hallucis capsularis (1.37 mm).
Conclusion:
This cadaveric study suggests that S-PeICO is anatomically feasible when performed by experienced surgeons, but narrow safety margins and the potential of tendon lesions should be considered.
Introduction
Hallux rigidus (HR) is a degenerative condition of the first metatarsophalangeal joint (MTPJ) that can cause pain, difficulty walking or playing sports, and joint stiffness.1-3 Severe symptomatic degenerative arthritis is the main reason for performing arthrodesis of the first metatarsophalangeal joint. 1 This can be done either with a percutaneous approach or through traditional open surgery.4-7 In addition to fusion, total or hemi-arthroplasty of the MTPJ has been used for the same purpose with varying results.2,8 Recently, hemiarthroplasty with synthetic cartilage implantation has shown higher failure rates and less favorable outcomes compared with fusion. 2
Joint-preserving techniques should be considered for patients with less severe symptoms and residual MTPJ motion. These techniques include cheilectomy,3,8 interpositional arthroplasty, 9 phalangeal osteotomies, 10 and shortening osteotomies.11-15
Shortening osteotomies, which aim to decompress the joint, are primarily associated with the terms of Youngswick procedure 14 or Waterman-Green osteotomy13,16 and have shown the same recommendation for intervention as cheilectomy, 31 and have achieved good to excellent clinical outcomes for the treatment of HR.11-15
Recently, some systematic reviews have concluded that percutaneous surgery is a safe and reliable method, improving clinical outcomes, particularly in function and quality of life, as a treatment option for hallux valgus (HV) deformities.17-19 Additionally, current cadaveric studies have demonstrated that percutaneous surgery is safe and effective when performed by experienced surgeons for treating hallux disorders.20-24 This also aligns with comparative clinical studies on open surgery.25-27
This study evaluates the safety and accuracy of a percutaneous shortening osteotomy of the first metatarsal called shortening percutaneous, intra-articular, chevron osteotomy (S-PeICO), which usually includes a percutaneous cheilectomy. This procedure is a modification of the PeICO technique (percutaneous intra-articular chevron osteotomy), previously developed for treating HV (the third-generation, or “3G,” procedure). 28 PeICO is safe, effective, and reliable based on clinical series and cadaveric studies.21,29 The indications for S-PeICO are HR grades I and II. 1 This innovative technique aims to restore mobility, reduce pain, and preserve the MTPJ, as demonstrated in the description of the technique and recent case series. 30 In this anatomical study, our goal is to assess neurovascular and tendon damage and to evaluate the accuracy of the cheilectomy osteotomy, including resection and angulation, respectively.
Material and Methods
This study was carried out in the Department of Anatomy at our university. We used 12 fresh frozen cadaveric specimens below the knee. Cadavers were excluded if they showed signs of additional forefoot deformities, ulcers, or previous surgical scars. Six specimens were from left feet, and six from right feet; eight were female, and four were male. The average age was 42.5 years (range, 23-63; SD, 13.2). All procedures were performed by the senior author, who has 13 years of experience in percutaneous surgery. IRB approval was obtained with institutional review board number 00003099.
The specimens were classified using a 5-grade system (0-4) based on clinical and radiographic criteria Hallux rigidus(HR) Coughlin & Shurnas (C&S) (HR C&S I and II). 1 Additionally, some cases of mild and moderate HV were included. Demographic data are summarized in Table 1.
Demographic Data.

Abbreviations: HR, hallux rigidus; HV, hallux valgus.
Surgical Technique
a. Using a No. 15 blade, a medial portal (P1) was created at the end of the proximal third of the metatarsal head (same incision point used in the PeICO osteotomy)21,29 but 2 mm dorsal to the center of rotation of the first metatarsal head. The incision point was guided with radioscopy (Figure 1). This portal allows debridement of the dorsal osteophyte and facilitates the S-PeICO.
b. A percutaneous dorsal capsular detachment (same as PeICO) was performed using a blade to create a working space (Figure 2). Then, dorsal osteophyte debridement was carried out with a wedge burr, 2.9 × 13 mm In2Bones. Finally, bone debris was cleared using a small bone rasp.
c. Then, a Shannon burr, 12 × 2 mm In2Bones, was introduced through the first metatarsal head in a medial-to-lateral direction to create the vertex of the S-PeICO. Next, the dorsal limb was established at a 10-degree angle, oriented proximally relative to the sagittal plane of the first metatarsal. Then, the plantar limb was formed with a 10-degree downward (plantar) tilt relative to the ground. This resulted in approximately 3 mm of shortening (the diameter of the Shannon burr is 2 mm) and a slight plantarization of the first metatarsal head to decompress the joint. The angle between the 2 limbs of the osteotomy was aimed to be between 90 and 100 degrees (Figure 3). Extreme caution was necessary to avoid injury to dorsomedial digital nerve (DMDN) and dorso lateral digial nerve (DLDN). To reduce soft-tissue tension and lower the risk of neurovascular and tendon injury, the procedure should be performed with a 30-degree passive metatarsophalangeal dorsiflexion using the nondominant hand.
d. Then, through a dorsomedial portal (or P2, which can be medial or lateral relative to the EHL), osteosynthesis was performed using a 3.5-mm I.B.S. neutralization screw In2Bones® from a dorsal to plantar direction at a 45-degree angle (sagittal edge) (Figure 4). To minimize risk, blunt dissection of soft tissues was performed after making both incisions.
Following the procedure, all specimens were dissected by an experienced anatomist. Special care was taken when dissecting the digital nerves, which were done using a proximal-to-distal technique, to avoid accidentally cutting any nerve branches.

(A) Location of portal 1 (P1) under radioscopy. (B) Dorsal capsulotomy.

Dorsal cheilectomy made with a wedge burr through P1.
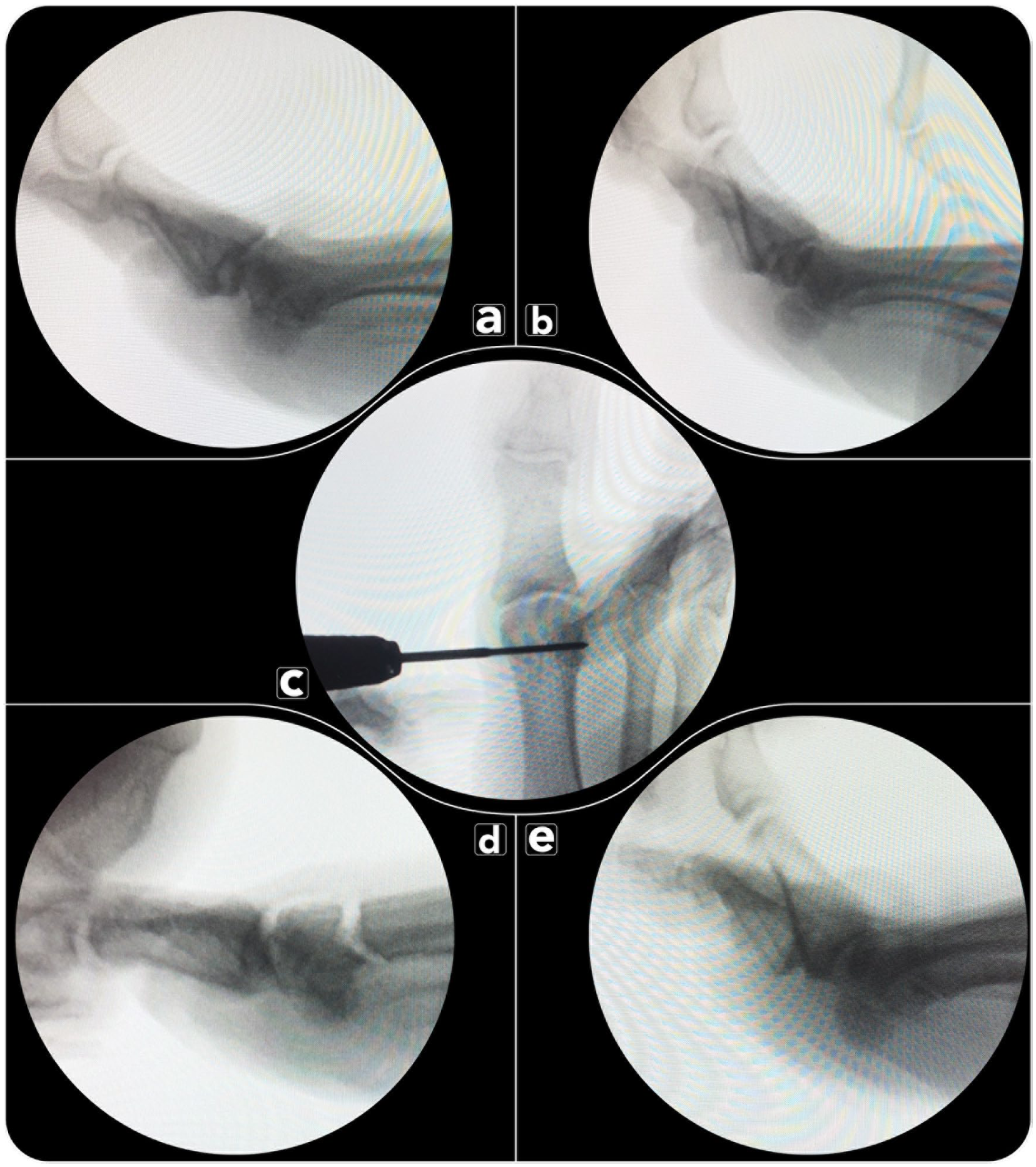
(A) Grade I HR (Hallux rigidus) C&S (Coughlin &, Shurnas). Metatarsophalangeal dorsiflexion: 36 degrees. (B) Dorsiflexion post cheilectomy: 53 degrees. (C) Location of insertion of the Shannon burr. (D) Intraoperative stress view of osteotomy. (E) Dorsiflexion post shortening percutaneous, intra-articular, chevron osteotomy (S-PeICO): 75 degrees.

A 3.5-mm compression screw is introduced through the dorsomedial osteosynthesis portal (P2; lateral to the extensor hallucis longus [EHL] tendon).
Primary Outcomes
To assess the safety of the procedure, the following measurements were recorded:
Distance between P1 and the DMDN;
Distance between P2 and the medial border of the EHL tendon.
Distance between P2 and DMDN.
Distance between P2 and extensor hallucis capsularis.
Distance between P1 and the MTPJ.
Distance between P2 and MTPJ.
Lesions of the DMDN, dorsolateral digital nerve, EHL, extensor hallucis brevis, and extensor hallucis capsularis were also assessed. A skin window was created on the forefoot to identify all structures, and any damage was measured and recorded if observed. Additionally, the angulation and completeness of the osteotomy in the sagittal plane were evaluated.
Secondary Outcomes
The osteotomy angulation in the sagittal plane (reproducibility) was measured, as well as its completion.
Additionally, the resection during cheilectomy was evaluated using the osteophyte and cheilectomy measurement (OQM). The authors created a method to assess osteophyte removal. A tangent line (T) was drawn along the dorsal cortical bone of the first metatarsal shaft, ending at the distal metaphysis. Then, 2 lines were drawn to measure the angles between them. One line connected the dorsal metaphysis and the apex of the osteophyte (preoperatively). The other was drawn from the same point to the distal border of the first metatarsal head (postoperatively).
Two independent observers (a foot and ankle surgery fellow and a 5-year-experienced foot and ankle surgeon) made all the measurements, and each observer took 2 measurements for each parameter. We considered values less than 4 mm (average or median) to be risky. 31
Statistical Analysis
A Shapiro-Wilk test was conducted to assess the normality of the data. If the data followed a normal distribution, means, ranges, and SDs were calculated. Otherwise, medians were reported. The Mann-Whitney test was used to compare both groups. Statistical analysis was conducted using R, version 3.4.3. A P value of less than .05 was statistically significant.
Results
Overall lesion rate was 16.6% (2 specimens); one presented a 50% extensor hallucis brevis lesion and one a complete lesion of the extensor hallucis capsularis tendon. No neurologic injuries were found (Figure 5). The blade could have injured both structures.

Specimen 8. No lesions were observed in the (1) DMDN, (2) extensor hallucis longus (EHL) tendon, (3) dorsomedial osteosynthesis portal (P2), and (4) P1.
No statistically significant differences were found in intraobserver measurements. However, when comparing evaluations between observers, 2 measurements showed statistically significant differences—the distance between P1 and the medial border of EHL and the distance between P2 and MTPJ. These differences were only observed at the upper end of the distance range. The smallest distances recorded were between P1 and DMDN (3.5 mm) and between P2 and extensor hallucis capsularis (1.37 mm). Results are summarized in Table 2.
Results.

Abbreviations: DMDN, dorsomedial digital nerve; EHL, extensor hallucis longus; MTPJ, metatarsophalangeal joint; P1, portal for S-PeICO (shortening percutaneous, intra-articular, chevron osteotomy); P2, portal for osteosynthesis.
Statistically significant differences were found in the distances between P1 and the medial border of the EHL, and between P2 and the MTPJ. The shortest distances observed were between P1 and DMDN and between P2 and the extensor hallucis capsularis.
Secondary Outcomes
Osteotomy angulation in the sagittal plane (reproducibility) averaged 99.2 degrees (range: 89.4-117.9; SD: 8.2), and all specimens had a complete osteotomy. The mean OQM was 6.76 degrees (SD 3.1).
Discussion
The most significant finding of this study is that the S-PeICO was technically feasible and allowed completion of the planned osteotomy in all specimens; however, tendon injuries and proximity to critical structures highlight the need for caution and further clinical validation.
S-PeICO is a variation of the PeICO technique. PeICO has a technical description linked to a case series 29 and a cadaveric study 21 for the treatment of HV. The main differences between PeICO and S-PeICO are as follows: because S-PeICO is indicated for HR, there is no need for lateral displacement of the metatarsal head; it allows shortening and plantarization of the first metatarsal head; the osteotomy portal (P1) is more dorsal, the osteosynthesis portal (P2) is medial to the EHL, and the fixation is preferably oblique, mainly in the sagittal plane.
Recently, the authors described the technique and shared preliminary results of the S-PeICO. 30 They conducted a prospective study involving 16 patients with an average age of 58.6 years (range, 35-78). The mean follow-up was 51.5 months (range, 49-77 months; SD, 5.43). The average operation time was 37.6 minutes per foot (range, 26-48; SD = 3.94). The average improvement in the passive range of motion of the first MTPJ was 34.1 degrees (preoperatively, 33.8 degrees; postoperatively, 67.9 degrees). The OQM measured 50.44 degrees. The first metatarsal shortened by an average of 4.3 mm (68.5 ± 2.01). The clinical evaluation included visual analog scale, forefoot American Orthopaedic Foot & Ankle Society, Foot and Ankle Ability Measure (FAMM), FAMM sports, and Manchester-Oxford Foot Questionnaire. The differences between preoperative and postoperative values were statistically significant (P < .0001). The overall complication rate was 12.5% (2 cases: 1 screw removal and 1 transient dysesthesia of the DMCN).
Damage to the digital nerves and ongoing sensory symptoms are the most common complications of HR (osteotomies and dorsal cheilectomy) and HV (osteotomies and bunionectomy) surgeries, according to Miller and Hartman 32 and Zdilla et al 33 respectively. The nerve injury rate in percutaneous techniques (HV and HR) can be high, ranging from 0 to 50%.21,23 The DMDN of the first toe is at the greatest risk of iatrogenic injury because of its proximity to the osteotomy portals, which are mainly located medially. Recent studies have shown significant differences between experienced and inexperienced surgeons performing percutaneous cheilectomy and Bosch procedures.23,34 McGann et al 24 recently found that the DMCN was fully transected in 4 cadavers and partially injured in 1 case (nerve partially cut) during an extra-articular chevron MIS for HV. Although the authors noted that the surgeon had prior experience with percutaneous procedures, the data are inconsistent with other published studies. 21 A recent study by Teoh et al3,34 described DMCN complications in 2 studies involving percutaneous cheilectomy. Dissection in a cadaveric study showed that the DMCN was entirely damaged in 2 specimens (15%). 3 Similarly, clinical research indicated that 2 patients (2%) experienced transient nerve paresthesia. Another 2 (2%) reported numbness in the DMCN area.3,12 None of the specimens in our study showed the damage described above. Based on published data, this could be linked to the position of the MTPJ during MIDC, although it was not specified. It appears that 0 degrees of dorsiflexion was used in Teoh et al’s study, which does not reduce tension in neurovascular structures and may increase the risk of injury. Incorrect dissection techniques and limited experience with a percutaneous burr may also contribute to this risk, as noted by Teoh et al.35,36 This increases the risk for dorsal cutaneous nerve and tendon injuries and can influence decision making, potentially preventing complications during percutaneous HR procedures. Our study showed no dorsal cutaneous nerve injuries. These promising results may be due to the 13 years of experience in MIS surgery training. However, the proximity between DMDN and P1 was among the lowest, requiring extreme caution.
Cheilectomies are recommended as a first-line treatment for HR grade I, which is usually characterized by intact cartilage.5,8 They can be combined with other procedures, such as arthroplasty and osteotomy, in more advanced stages. 3 According to several authors, 20% to 30% of the dorsal metatarsal head and dorsal osteophytes of the metatarsal head and proximal phalanx should be removed.37,38 This procedure can be performed using open surgery, percutaneous surgery, or arthroscopy. Open cheilectomy for treating HR has been reported to have satisfaction rates ranging from 40% to 100%,8,39 with failure rates of 4.9% to 8.21%.8,11,40 Our study showed that despite performing a more neutral cheilectomy, no damage to anatomical structures was observed. Undoubtedly, the benefit of this resection should be assessed within a clinical context.
Tendon (including tendon sheath) lesions after percutaneous surgery occur at a notable rate (0-56%).22,41 -43 The EHL is particularly vulnerable during dorsal capsular detachment, cheilectomy, and the dorsal limb of S-PeICO. In this study, to reduce soft tissue tension, a passive dorsiflexion force of 20 to 30 degrees was applied to minimize tissue stress during these procedures. The results showed an overall tendon lesion rate of 16.6% (2 specimens), consisting of 1 partial EHL lesion and 1 complete lesion of the extensor hallucis capsularis tendon. Although this indicates a high incidence, it may not pose a significant clinical issue. A partial EHL injury would likely heal without complications, and a complete injury to the extensor hallucis capsularis tendon can also be considered minor or irrelevant. In this study, the extensor hallucis capsularis tendon, a tendinous slip branching off the extensor hallucis longus tendon and inserting on the dorsomedial aspect of the first MTPJ capsule, was identified in all specimens, consistent with recent literature that considers it an almost constant finding.44,45 During S-PeICO, the extensor tendons are at high risk of injury when subjected to tension against the burr and percutaneous blade. Because the burr is used deeply within the capsule, we assume that no injuries related to that maneuver were observed in this study, and that the blade caused injuries during portal placement.
A recent comparative study by Stevens et al 41 found that MIS cheilectomy has a higher relative risk of requiring additional surgery, such as nerve and tendon injuries, compared to open cheilectomy. Using a paratendinous portal and sometimes an accessory portal distal to the first MTPJ may increase the risk of nerve damage, which could explain their findings. Our results suggest that a medial (3 mm dorsal) portal might help prevent both types of injuries. Another technical tip for avoiding iatrogenic damage to the extensor tendons, in addition to performing passive dorsiflexion of the MTPJ when using the percutaneous burr, is to use an auxiliary suture to elevate and lift the tendons away from the bone, creating a tentlike working space during cheilectomy. 46
Open cheilectomy for treating HR has shown satisfaction rates ranging from 40% to 100%.8,39 The failure rates have been reported to be between 4.9% and 8.21%.8,11,40 Including a decompression osteotomy may offer additional pain relief and greater improvement in dorsiflexion compared with cheilectomy alone. Recently, Cullen et al 11 reported a significantly higher revision rate in the cheilectomy group (8.21%) than in the plantarflexion decompression osteotomy group (1.22%). The S-PeICO technique, which combines a cheilectomy with a decompression osteotomy, demonstrated passive improvement in the metatarsophalangeal range of motion and, secondarily, better clinical outcomes in the first study published by Del Vecchio et al. 30
Decompression osteotomies of the head of the first metatarsal are recommended for intervention (C), similar to cheilectomy, as reported by McNeil et al. 37 They have achieved good to excellent clinical results in series for the treatment of HR.11,13,15 These procedures may involve shortening, plantarization, or both. 12 Green-Waterman’s technique, used by Dickerson et al, 13 is applied in cases of dorsal joint erosion, preserving the plantar articular surface. It allows for shortening and decompresses the MTPJ. The Youngswick osteotomy enables plantarization and shortening of the metatarsal head, reducing dorsal bone impingement, as described by Slullitel et al 14 and Youngswick. 47 It produces outcomes similar to the Green-Waterman technique but involves a 60-degree osteotomy rather than the 135-degree angle used in the Green-Waterman procedure. Cullen et al 11 showed that the revision rate was significantly higher for cheilectomy (8.21%) than for decompression osteotomies (1.22%). Recently, Cöster et al 48 found that patients with moderate HR improved within 1 year after surgery, regardless of whether they received a Youngswick osteotomy or a cheilectomy, as measured by patient-reported outcomes. The improvement was clinically relevant compared to isolated cheilectomy, according to Cöster et al. 48 Ohara et al 49 demonstrated that the elevation of the first metatarsal head gradually increased as the HR grade worsened. Therefore, plantarization osteotomies combined with cheilectomy help treat low-grade HR using S-PeICO, allowing for shortening and plantarflexion when needed while also providing passive dorsiflexion. 30 The present study on a chevron-shaped decompression osteotomy, indicated for low-grade HR.
This study has some limitations. First, we had a limited number of specimens. Second, the increased stiffness in the cadaveric specimens could have affected our results. In a clinical setting, performing an S-PeICO might be more feasible. Third, HR treatment is a controversial topic, with different surgical techniques and outcomes published. It is not possible to guarantee that a successful cadaveric procedure would also be successful in clinical practice. We emphasize that percutaneous surgery has a prolonged learning curve50,51 and, therefore, may be challenging to reproduce the results shown in this study.
Conclusion
This cadaveric study indicates anatomical feasibility of S-PeICO for HR, but does not establish clinical safety or efficacy. These findings support further investigation through prospective clinical trials before routine adoption. We emphasize that percutaneous surgery for HV and HR can involve a prolonged learning curve, requiring dedicated, structured training to consistently ensure, produce, and attain the best possible outcomes for our patients.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251412837 – Supplemental material for Shortening, Percutaneous, Intra-articular, Chevron Osteotomy for the Treatment of Hallux Rigidus: An Anatomical Feasibility and Risk Assessment in Cadavers
Supplemental material, sj-pdf-1-fao-10.1177_24730114251412837 for Shortening, Percutaneous, Intra-articular, Chevron Osteotomy for the Treatment of Hallux Rigidus: An Anatomical Feasibility and Risk Assessment in Cadavers by Eric Daniel Dealbera, Gabriel Ferraz Ferreira, Andreas Toepfer, Miki Dalmau-Pastor and Jorge Javier Del Vecchio in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
The authors express their gratitude to the donors of the Dissection Room and Body Donors Service at the University of Barcelona for their generosity.
ORCID iDs
Ethical Considerations
The Bioethics Committee of our institution approved the cadaveric study (institutional review board number 00003099). Approval from the Institutional Review Board was obtained, and in keeping with the policies for a retrospective review, informed consent was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.