
Abstract
Background:
Diabetic patients with foot ulcers are commonly prescribed assistive walking devices to unload the affected foot and promote tissue healing. However, the effect on shear loads to the contralateral foot is unknown. This study investigated the effect of a wheeled knee walker (WKW), compared to common devices, on compressive and shear plantar forces carried by the propulsive foot during walking in patients with type 2 diabetes mellitus. A secondary objective investigated plantar forces’ correlations with body weight unloaded (BWU).
Methods:
Participants walked a maximum of 200 m per condition during normal walking or when using crutches, a standard walker, and a WKW in randomized order. Plantar forces were measured with force plates, and wireless force-sensitive pads measured BWU through the hands. The WKW was instrumented to measure BWU onto the seat and handlebars. Three-dimensional motion capture confirmed gait events.
Results:
The WKW produced the lowest vertical, braking, propulsive, and medial shear forces but the highest lateral shear force among all conditions. Using crutches or a walker had negligible medial and lateral shear (mean = −6.69 N and −7.80 N), with normal walking producing the highest medial shear. There was a poor relationship between BWU and assistive walking devices and shear force values.
Conclusion:
A WKW could be the preferred assistive device for unloading a diabetic foot ulcer. The magnitude of lateral force would need further investigation to determine ulceration risk, given patient susceptibility and neuropathy.
Clinical Relevance:
Understanding shear forces on the propulsive foot is important for minimizing contralateral limb tissue damage risk while treating an ulcer. Different assistive walking devices change walking patterns and affect shear forces on the plantar surface of the foot. Although the WKW minimizes several loading metrics, a clinical trial investigating assistive walking device compliance and wound healing in diabetic foot ulcer patients across devices is needed.
This is a visual representation of the abstract.
Introduction
Type 2 diabetes mellitus (DM) is an endocrine disorder that affects an estimated 28.5 million adults in the United States. 7 Type 2 DM can cause changes in the central nervous system, neuropathy, and loss of sensation in the foot, leading to gait abnormalities and abnormal tissue loading.5,12,18 Symptoms of type 2 DM include ulcerations of the plantar foot, with forefoot ulcerations being the most common.6,15 There is a 15% to 25% risk of developing a diabetic foot ulcer (DFU) in the lifetime of a person with type 2 DM, with neuropathy increasing this 4 times. 17 DFU treatment includes casting, removable walking boots, half-shoes, and walking devices such as crutches, walkers, and wheeled knee walkers (WKWs).3,4,15 Some of these devices unload body weight onto the hands, or hands and knee/anterior shank for the WKW, to reduce forces on the plantar surface of the foot and promote tissue healing.
Axillary crutches and walkers have been commonly prescribed because of their familiarity and availability in clinical settings. 13 Recently, WKW use has increased from perceived benefits with patient comfort and mobility.2,4,13 A WKW also allows patients to offload body weight onto the ipsilateral knee and hands and lowers the chance of crutch palsy. 14 Although assistive walking devices offload the affected foot to promote healing, the contralateral propulsive foot (unaffected limb) has increased loading exposure in healthy older adults. 11 However, shear force exposure occurring on the propulsive foot in those with type 2 DM or the applicability of loading profiles from healthy older adults representing this clinical population is unknown.
Shear forces occur on the foot from side-to-side (medial/lateral or M/L) and front-to-back (anterior/posterior [A/P], or braking/propulsive) reaction forces. Shear loading is a major risk factor for diabetic foot ulcer formation via accelerated tissue breakdown and an increased rate of callus formation.1,2,5,9 Patients with type 2 DM and neuropathy have, respectively, 20.4% and 20.7% higher lateral shear force and significantly higher peak shear load during unassisted ambulation than healthy older adults.10,17 However, foot loading changes during DFU treatment as the injured foot is offloaded, and the propulsive foot provides increased propulsive forces. Therefore, clinicians need a consistent way to offload the ulcerated foot and minimize the increase of shear force on the propulsive foot.
It is necessary to determine propulsive foot shear force exposure while using different walking devices. Our first step is an assessment of plantar loading mechanics during walking with common assistive walking devices (Figure 1). Therefore, this study aims to compare the effect of walking device use on shod (wearing shoes) propulsive foot shear forces in patients with type 2 DM without a DFU. We hypothesized that propulsive foot shear forces would differ between walking devices and normal walking, with normal being the lowest, followed by WKW, standard walker, and crutches, because of offloading to the handles and knee pad with ease of motion due to wheels. Our second hypothesis was there would be a moderate positive correlation (r = 0.3-0.5) between body weight unloaded (BWU) onto assistive devices and shear forces due to inherent variability between participant walking patterns.

Assistive walking devices used in this study: (A) Wheeled Knee Walker (Steerable Knee Walker; Elenker, Chino, CA) with red arrows indicating uniaxial strain gauges used to measure vertical forces at the handles (TAL206; HT Sensor Technology Co, China) and the knee cushion (TAL208, HT Sensor Technology Co, China). (B) Standard Walker (Deluxe Folding Walker; Drive, Port Washington, NY), and (C) crutches (Aluminum Crutches; Drive).
Methods
Participants
Twenty-four participants with type 2 DM (8M:16F) were recruited for this study (Table 1). Informed consent was obtained before data collection per our local IRB procedures. Inclusion criteria were people older than 40 years with type 2 DM, hemoglobin A1c ≤10% (≤86 mmol/mol), and self-reported ability to walk for 5 minutes at a self-selected speed without support. Exclusion criteria consisted of a history of lower extremity joint replacement or amputation, unexplained dizziness in the last 6 months, use of an assistive device during the previous 12 months, patients currently in treatment for a DFU, and body weight >136 kg (weight capacity of assistive devices).
Participant Demographics. a

Diagnosis duration (years) represents the mean time participants have been diagnosed with type 2 DM per individual medical records.
Procedure
Participants were screened for eligibility with a self-reported medical history questionnaire before data collection. Height and weight were recorded. Then, a familiarization period took place, in which crutches, a walker, and a WKW were fitted to each participant to ensure comfort and proper use. Next, participants chose their propulsive limb, which was consistent for all assistive devices. Experimental sessions included 4 walking conditions: normal walking, crutches, walker, and WKW. For each condition, participants were instructed to walk back and forth on a straight 10-m path for 200 m or until they could not continue. A total walking distance of 800 m represents typical community-based walking bouts. 16
After familiarization, the participants were instructed to walk as normally as possible across the force plates. Further, they were instructed to only place the propulsive foot on the force plates, while avoiding placing the assistive device or offloaded foot on the plates. The participants were allowed to use a self-selected gait style for comfort, as long as the simulated affected limb was nonweightbearing.
Force-sensitive insoles (Loadsol, Novel Electronics Inc, St Paul, MN) measured normal force at 100 Hz from the forefoot, midfoot, and rearfoot as previously reported. 2 Insole sizes ranged from US men’s 6-14 and US women’s 5.5-11. 2 The insoles were calibrated to each participant’s body weight before data collection following the manufacturer’s protocol. Force-sensitive pads (Loadpad; Novel Electronics Inc) measuring load at the hands were calibrated to the participant's body weight by instructing them to stand on the pad with one foot on the toes and forefoot. 2 Pads were wrapped around the handlebars of the crutches and walker to measure BWU to the assistive device at 100 Hz. 2 A custom WKW with uniaxial strain gauges (TAL206; HT Sensor Technology Co, Ltd, China) under the handlebars and knee cushion (TAL208; HT Sensor Technology Co) measured BWU at 50 Hz. Kinematic data were captured via 20 infrared cameras (Motion Analysis Corp, Ronhert Park, CA) at 100 Hz with 54 reflective markers placed on the participant’s trunk, pelvis, and lower limbs.
Data Processing
Twenty-two participants were included for data analysis as 2 subjects had inadequate force plate data because of the foot striking multiple plates throughout the trial (Table 1). Data from 8 force plates (400600HPS, AMTI Inc, Watertown, MA), pads, and WKW uniaxial strain gauges were then processed. Kinetic and kinematic data were processed using Visual3D (version 2022; C-Motion, Germantown, MD) and MATLAB (R2022b, The Mathworks Inc, Natick, MA). Forces acting on the outsole of subjects’ footwear were truncated into stance periods and normalized to 101 points (0-100% stance) for M/L and A/P shear, and vertical compression. Then, ensemble means and SDs were calculated for each walking trial in each condition. Maximum and minimum peaks for each walking condition in M/L, A/P, and vertical forces were used for statistical analysis.
During the Normal, Crutches, and Walker conditions, the insoles and motion capture systems were synchronized by stomping on a force plate at the start of each walking trial for participants 1-13. 2 The stomp produced a spike in normal insole force and force plate data, which was used to synchronize the signals to within 3 frames at 100 Hz. A pause occurred after the stomp as the participant repositioned off the force plates isolating the spike. For the WKW, a force-sensing pad was placed on the handlebars, and a strain gauge was installed under the handlebars and knee cushion. 2 Participants were instructed to slap the pad while the WKW was in line with the center of a force plate. The slap caused a spike in the force data through the pad, strain gauge, and force plate used to synchronize signals in post-processing. Data-stream synchronization required force plate data to be down-sampled to 100 Hz, with strain gauge data interpolated from 50 Hz to 100 Hz as previously described. 2 A force threshold of 50 N for instrumented insole data was used to identify when stance periods started and ended.2,10 Participants 14-24 (15 and 21 were data exclusions) had a synchronization device that used a TTL synchronization voltage from the motion capture system to mark frames in the instrumented insole data. After defining outsole stance periods, the average force per stance period was calculated and normalized to body weight for each modality. Because the insole sensors only reported normal force, data for the M/L, A/P, and vertical compression outsole stance period came from the force plates.
Statistical Analyses
Statistical analyses were completed using SPSS (version 28; IBM, Armonk, NY). To address our first hypothesis, 3 separate (M/L, A/P, vertical) 1-way repeated measures analyses of variance were used to compare each modality’s maximum and minimum peaks. Significant main effects of walking conditions were investigated using Bonferroni-adjusted pairwise comparisons. For the second hypothesis, 3 Pearson correlations assessed the relationship between BWU to the assistive device and shear forces. Correlation coefficient strengths were defined as 0-0.09 negligible, 0.1-0.29 weak, 0.3-0.49 moderate, 0.5-0.69 strong, and 0.7-1.0 very strong. 8 All statistical tests were performed with an a priori α of 0.05.
Results
Shear Forces
The 3 walking devices had significant within-subject main effects for propulsive limb shear loading (P < .001). In peak medial shear, the WKW was 5.3% (12.44/13.13), 81.1% (12.44/65.79), and 4.7% (12.44/13.05) lower than Crutches, Normal, and Walker conditions, respectively (Table 2). Post hoc tests revealed a significant (P < .001) difference between Normal and all other devices. For peak braking A/P shear (P < .001), the WKW was 90.8% (14.61/158.37), 89.4% (14.61/137.82), and 85.3% (14.61/99.29) lower on average (Figure 2). In addition, the WKW was 33.1% (−75.97/−113.61), 46.6% (−75.97/−142.27), and 21.3% (−75.97/−96.49) lower on average for peak propulsive A/P shear, with a significant difference compared with Normal and Crutches (P < .001). A significant difference (P = .033) was found between the WKW and Walker. The WKW was 43% (24.29/42.65), 42.3% (24.29/42.09), and 47.6% (24.29/46.37) lower on average for minimum vertical compression, and post hoc tests revealed a significant (P < .001) difference between the WKW and all other devices similar to our previous findings. 2
Mean (SD) and 95% CIs for Variables of Interest Across All Conditions. a
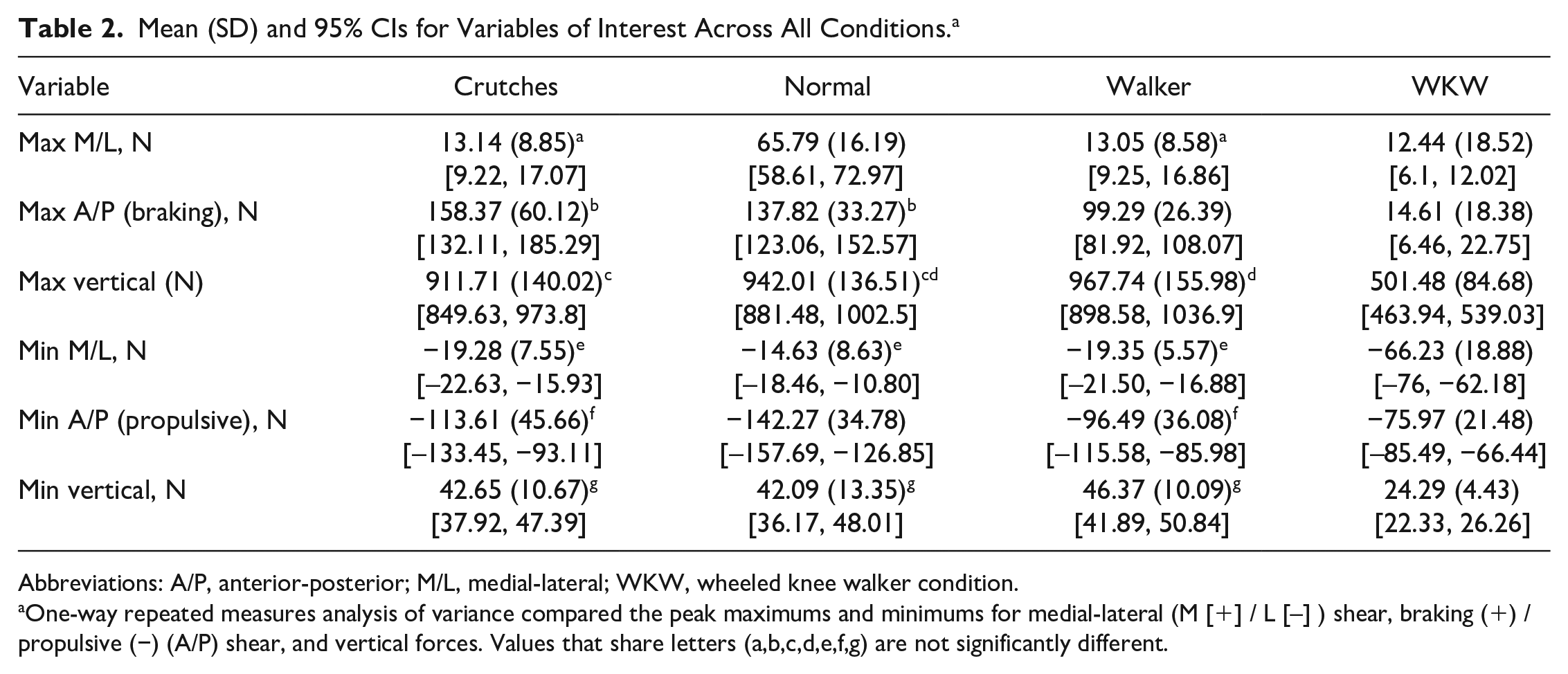
Abbreviations: A/P, anterior-posterior; M/L, medial-lateral; WKW, wheeled knee walker condition.
One-way repeated measures analysis of variance compared the peak maximums and minimums for medial-lateral (M [+] / L [–] ) shear, braking (+) / propulsive (−) (A/P) shear, and vertical forces. Values that share letters (a,b,c,d,e,f,g) are not significantly different.

Sample means for mediolateral (top), anteroposterior (middle), and vertical (bottom) forces measured from embedded force plates. Colored lines indicate crutches (red), normal walking (green), standard walker (blue), and wheeled knee walker (black) conditions. Shaded regions are 1 SD about the mean. Waveforms are normalized to 100% stance from initial to final contact on an ipsilateral limb.
Of note is the increased peak lateral shear of the WKW (P < .001), being 243.5% (−66.23/−19.28), 352.7% (−66.23/−14.63), and 242.3% (−66.23/−19.35) higher compared to Crutches, Normal, and Walker respectively (Table 2).
Compression
The WKW was 45% (501.48/911.71), 46.8% (501.48/942.01), and 48.2% (501.48/967.74) lower on average for maximum vertical compression (Table 2), with post hoc tests showing a significant (P < .001) difference between the WKW and all other devices.
Correlations
Pearson correlations showed negligible and weak correlations between BWU to the device and shear forces (Table 3). One moderate positive correlation (r = 0.357) was found between the Walker condition and maximum peak medial shear (Figure 3). There is one outlier above the threshold of 100% body weight; this could be due to artifacts in the pads or force readings from the weight loaded on top of the pad plus handgrip squeezing, which cannot be separated when assessing forces in these sensors.
Pearson Correlation Coefficient r Values for the Relationship Between Body Weight Unloaded (BWU) Onto the Assistive Devices and Shear Forces. a
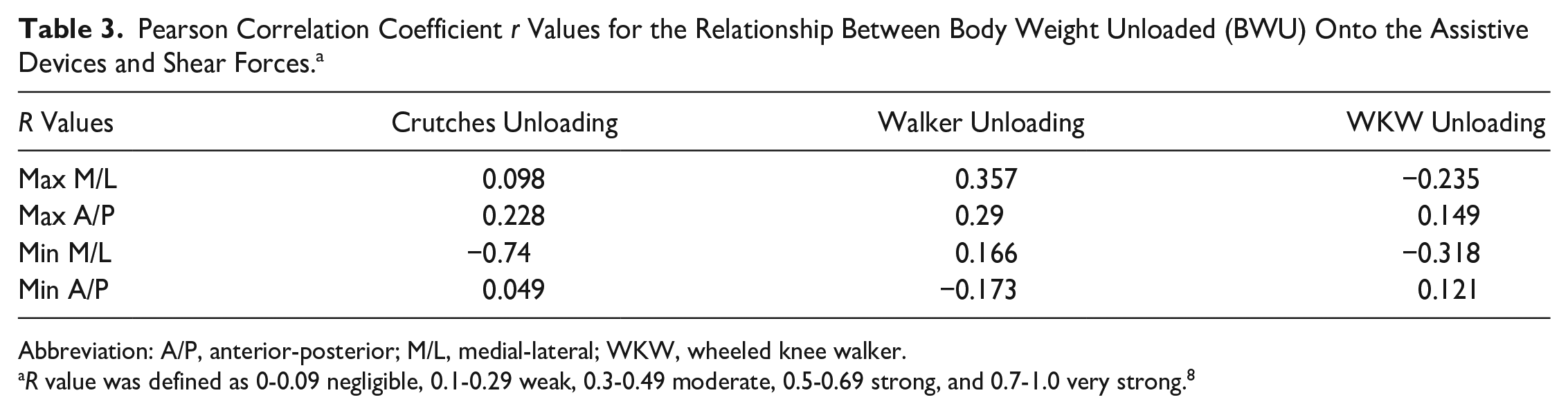
Abbreviation: A/P, anterior-posterior; M/L, medial-lateral; WKW, wheeled knee walker.
R value was defined as 0-0.09 negligible, 0.1-0.29 weak, 0.3-0.49 moderate, 0.5-0.69 strong, and 0.7-1.0 very strong. 8

Correlation between peak maximum walker medial shear (N) and walker body weight unloaded onto walking device handles.
Discussion
The purpose of this study was to compare the effect of walking device use on shod propulsive foot shear forces in patients with type 2 DM without a DFU. We hypothesized that (1) the propulsive foot shear forces would differ between walking devices and normal walking, with normal walking being the lowest, followed by WKW, standard walker, and crutches, respectively, and (2) there would be a moderate positive correlation (0.3-0.5) between BWU onto assistive devices and shear forces. Our first hypothesis was partially supported, as there was a significant difference between walking devices and normal walking. However, normal walking had the highest medial shear, propulsive shear, and vertical compression, which did not support our first hypothesis (Table 2). The WKW had significantly lower medial, braking, and propulsive shear than the other walking devices and normal walking, which partially aligned with the first hypothesis. The correlations between BWU and shear forces (Table 3) were negligible or weak except for walker and peak maximum M/L (r = 0.357) and crutches and peak minimum M/L (r = −0.74). Although the walker condition aligned with our second hypothesis, overall, our data did not support it. The WKW having lower vertical compression aligns with previous research where peak net force was 0.29 BW and 0.35 BW lower than walker and control conditions and produced 52.08%, 39.47%, and 47.73% lower peak forefoot force than Normal, Crutches, and Walker conditions.2,10
Prior work has shown older adults with type 2 DM have decreased reactive hyperemic skin response to shear forces on the forearm, suggesting that reparative mechanisms of the skin are impaired when responding to shear. 9 To our knowledge, this is the first study to investigate plantar shear forces among assistive devices in older adults with type 2 DM. Previous research investigating plantar shear force in persons with type 2 DM found that patients with neuropathy and callouses experience higher shear forces during overground gait but did not test patients while using walking devices or offloading one limb. 10 In another study, healthy older adults were tested across walking device use, with a significant difference in net vertical force on the propulsive limb. 11 The crutches were 0.04, 0.03, and 0.07 normalized body weight higher in peak net, midfoot, and rearfoot forces in the last 30-second epoch. 11 Walker use in this study also had significant (P < .01) differences in the average vertical force (967.74 N) between all the conditions, but shear forces were not reported. The handlebars and knee pad create an asymmetric loading environment that promotes more loadbearing onto the WKW than other walking assistive devices. Moreover, the vertical force created during the stance period could be less because the WKW is on wheels and only needs to maintain such forward momentum until braking is applied. Our study addresses a knowledge gap for clinical prescription of walking assistive devices by reporting significant differences in the maximum peak of M/L shear between Normal and all other devices, meaning the participants experience less medial shear force when using an assistive walking device to ambulate with one limb offloaded.
We speculate that assistive devices provide a more stable base of support, limiting the center of gravity from M/L deviations, which lowers the M/L shear produced during gait. This is supported by a significant difference between the WKW and all other devices for minimum peak M/L shear; however, the WKW had larger lateral shear magnitudes. The lateral shear generated was −66.23 N (lateral) on average, compared with the second highest condition of 65.79 N (medial) for normal walking. The Walker and Crutches conditions seemed to eliminate M/L shear from 10% to 87% stance. This could be because of the previously mentioned stability with upper body support. The lateral shear from the WKW could increase ulceration risk, but further basic science investigations would be required to determine what magnitudes are of concern for tissue remodeling for this clinical population.
The reduction in A/P shear may offset the magnitude of the lateral shear from the WKW. The WKW had significantly less average braking shear (14.61 N) than all other devices. The WKW also had a lower average propulsive shear (−75.97 N) than all other devices, suggesting lower energy to keep the WKW moving after momentum has begun. This could improve overall mobility, which is vital for older adults socioeconomically. The Walker and Crutches conditions had earlier peak braking shear and later peak propulsive shear compared to Normal walking. This could be due to the participant having to hop during locomotion, causing spikes when landing on the force plates.
Furthering our understanding of maximum and minimum peak shear forces is essential to represent how loading could harm tissue healing processes in people with type 2 DM. However, the amount of BWU onto assistive devices was poorly connected with the amount of shear forces produced by the participants. This could mean the device given and the way participants adapt their walking are independent. Each participant compensating to their body type would mean a different gait pattern. The gait patterns could lean on the arms or propulsive foot depending on assistive device and conscious choice by the participant. This means patients in clinical settings may need to be taught how to use the individual assistive devices to minimize the amount of shear put onto the propulsive foot. There would have to be a balance between the efficiency of movement and shear forces, which is why the WKW could be the way forward with the reduction in A/P shear and less vertical force.
The results of this study suggest the WKW could be the preferred assistive device for patients suffering from a DFU based on low vertical compression, medial shear, braking, and propulsive shear forces. The lateral shear magnitude during WKW use could be a risk factor for DFU development. However, further basic science research would be required to establish a magnitude of concern. Improving user technique to balance movement and shear force production efficiency should also be investigated before use in a clinical setting, but this was beyond the scope of this study. Correlation results suggest BWU and shear forces are independent. Proper training on the devices could benefit patients in understanding how to locomote with minimal shear, bringing the correlation closer together.
This study shows a need for research to be conducted on participants who experience neuropathy. The proof of concept was completed in a population with type 2 DM, but not neuropathy. The significant differences in shear forces and vertical compression could reduce the amount of skin damage seen in neuropathic patients. The research could point clinicians toward assistive devices that have wheels, or devices that allow offloading to the affected limb at the knee. This would reduce the amount of force on the propulsive foot.
There are limitations to this study, namely, that the study population was not neuropathic, participants had comorbidities, and variations in the force sensing area of the loadpads in measuring hand forces. The population studied included type 2 DM participants, but none had neuropathy. Neuropathy patients could respond differently to the devices based on their different comorbidities. The study was performed in a level and controlled laboratory space; community spaces will likely differ. Various comorbidities could affect gait patterns, which, in turn, would change shear force outcomes. The participants had good disease management and could cover the required distance for community-based walking. 2 The size of the force pads on the handlebars of the walking devices were wrapped around the handlebars, meaning extraneous grip measurements may have been measured rather than true BWU. 2
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241235911 – Supplemental material for Plantar Kinetics During Wheeled Knee Walker Use Compared to Different Assistive Walking Devices in Persons With Type 2 Diabetes Mellitus
Supplemental material, sj-pdf-1-fao-10.1177_24730114241235911 for Plantar Kinetics During Wheeled Knee Walker Use Compared to Different Assistive Walking Devices in Persons With Type 2 Diabetes Mellitus by Holton C. Gwaltney, Joseph W. Harrington, Jose G. Anguiano-Hernandez and David C. Kingston in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Informed consent was obtained before data collection per our local IRB procedures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: US Department of Health and Human Services, National Institutes of Health, National Institute of General Medical Sciences grant 5P20GM109090 (awarded to Holton C. Gwaltney, BS, Jose G. Anguiano-Hernandez, MS, and David C. Kingston, PhD); Graduate Research and Creative Activity grant 46649(awarded to Holton C. Gwaltney, BS, Jose G. Anguiano-Hernandez, MS, and David C. Kingston, PhD).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.