
Abstract
Background
As walking abilities are widely affected among the aging population, investigating the effectiveness of wearable device-based walking programs is essential. The intentions of this meta-analysis were to investigate their effects on gait speed among older adults, as well as to include subgroup analysis to evaluate potential effects on individuals with aging-related conditions such as Parkinson’s disease (PD) and stroke.
Methods
Systematic retrieval of Pubmed, The Cochrane Library, Embase and Web of Science databases were searched up to February 2024. Outcomes such as gait speed, balance, cadence, and stride length were extracted and analyzed. Study quality was evaluated using the Rob 2 tool and heterogeneity was tested using I2 statistics through STATA 16.
Results
Nine studies with 284 participants were analyzed. The intervention group showed a significant improvement in gait speed (weighted mean difference (WMD) 0.12; 95% CI 0.03 to 0.21). There is a subgroup analysis suggesting differential effects: significant improvements in PD and stroke subgroups, but not in the normal aging group. Balance (WMD: 1.93; 95% CI: 0.20 to 3.66) and stride length (WMD: 8.58; 95% CI: 3.04 to 14.12) were also shown to improve, but the heterogeneity across the studies was moderate (I2 = 63.91%). No significant changes were observed in the Timed Up and Go test, Gait Variability, and Step Width.
Conclusions
Wearable device-based walking programs improve gait speed in older adults, with top notch advantages in the ones tormented by PD or stroke. These findings advocate that such interventions can be a valuable part of individualized treatment strategies in geriatric care, aiming to enhance mobility and usual satisfactory of existence.
Introduction
Recently, significant declines were reported in several gait parameters like walking speed, stability, step frequency, and stride length, as age advances, commonly influencing the mobility and quality of life in old people. 1 These age-related changes are influenced by the high prevalence of geriatric conditions, such as Parkinson’s disease (PD) and stroke, which have their own significant effects on gait characteristics. Individuals with other neurologic conditions may demonstrate gait abnormalities such as festination and shuffling related to the progressive loss of dopamine in the basal ganglia, or individuals with a history of stroke may present with hemiplegic gait patterns, marked by asymmetry and reduced weight-bearing on the involved side.2-5
Since the role of gait problems in daily life functioning and risk of falling is substantial, training gait may be considered an important part of comprehensive fall prevention strategies.6,7 Rehabilitation has been central in addressing these gait and balance impairments over the years, with several studies supporting that rehabilitative treatments are beneficial in the improvement of these conditions.8-10 Nonetheless, the development of wearable sensor technology, embedding state-of-the-art inertial sensor technology and convenient wireless communication interfaces, has brought new possibilities to gait rehabilitation, enabling training machines to be more accurate, effective, and personalized.11,12
These wearable technologies allow for continuous monitoring and live feedback of physiological and kinematic data and, therefore, suggest a potentially fruitful path for improving the traditional methods used in rehabilitation. Their use has been positively affected in a number of different patient groups, such as people with cerebral palsy and chronic stroke, where they have shown muscle strengthening and improved walking and mobility, emphasizing the potential of these interventions to revolutionize rehabilitation practice.13-15 In addition, new ways of applying the technology exist, as virtual reality reflex therapy has shown better results than traditional physiotherapy in lower limb movement rehabilitation treatment, which indicates an increasingly wide variety of tools to be used during treatment. 16
In the midst of an aging global population and rising healthcare needs, we are very much in dire straits of implementing innovative gait rehabilitation solutions. The goal of this meta-analysis was to summarize the existing literature within the context of wearable technology-based treatments for gait enhancement in older adult populations in order to determine what interventions have the potential to replace and/or add to conventional care methods.
Methods
This systematic review was conducted following the guidelines outlined in the Cochrane Handbook for Systematic Reviews and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Literature Search
We systematically searched through four major databases (Cochrane, Embase, PubMed, and Web of Science) and used a wide range of keywords, including ‘wearable devices’, ‘gait’, and ‘elderly people’, to find relevant studies. Our search was limited to English-language, peer-reviewed journal articles published up to February 2024. Table S1 shows the detailed search strategy for each database to ensure reproducibility and scrutiny.
Inclusion and Exclusion Criteria
Two reviewers independently screened titles and abstracts of studies that met our predefined inclusion criteria: (1) studies with elderly participants (mean age ≥60); (2) studies focusing on gait-specific wearables; (3) studies reporting quantitative gait parameters such as speed, cadence, and stride metrics. Exclusion criteria selected studies of an editorial or commentary nature, studies that did not present important data, or studies with a general emphasis on other medical conditions. Disagreements among the researchers were solved by discussing with a third reviewer.
Data Extraction and Quality Assessment
We used standard templates to systematically extract essential data including study ID, location, sample characteristics, intervention specifics, and outcomes. The authors of the original studies were contacted for clarifications or missing details. Two reviewers assessed the risk of bias independently using the Cochrane Risk of Bias 2.0 tool, with disagreements resolved by consensus. 17
Statistical Analysis
This study, using Stata 16.0 software, was able to compile a meta-analysis using a random-effects model with the effect sizes, as well as 95% confidence intervals (CI), across the studies in the form of weighted mean difference (WMD) for continuous outcomes. We assessed heterogeneity using the I2 statistic and τ2 value, and performed subgroup analyses to explore the data in greater detail, in order to provide a thorough look at the complexities surrounding our findings. It also evaluates potential publication bias to provide the robustness and credibility of our conclusions, using funnel plots and Egger’s tests.
Results
Literature Search
Searching in PubMed, Web of Science, Cochrane Library, and Embase resulted in 470 records. Then after de-duplication and the exclusion of studies using automation, 177 titles remained. A screening of the titles and abstracts bracketed the number down to 32 papers for full-text review. We then excluded 23 reports, including 22 for insufficient data and one for limited sample size, and reserved 9 reports for further evaluation and pooling, as displayed in Figure 1.18-26 Flowchart for study screening and selection process according to the PRISMA guidelines.
Characteristics of Qualified Research
The Baseline Characteristics of the Studies Included in the Meta-Analysis.
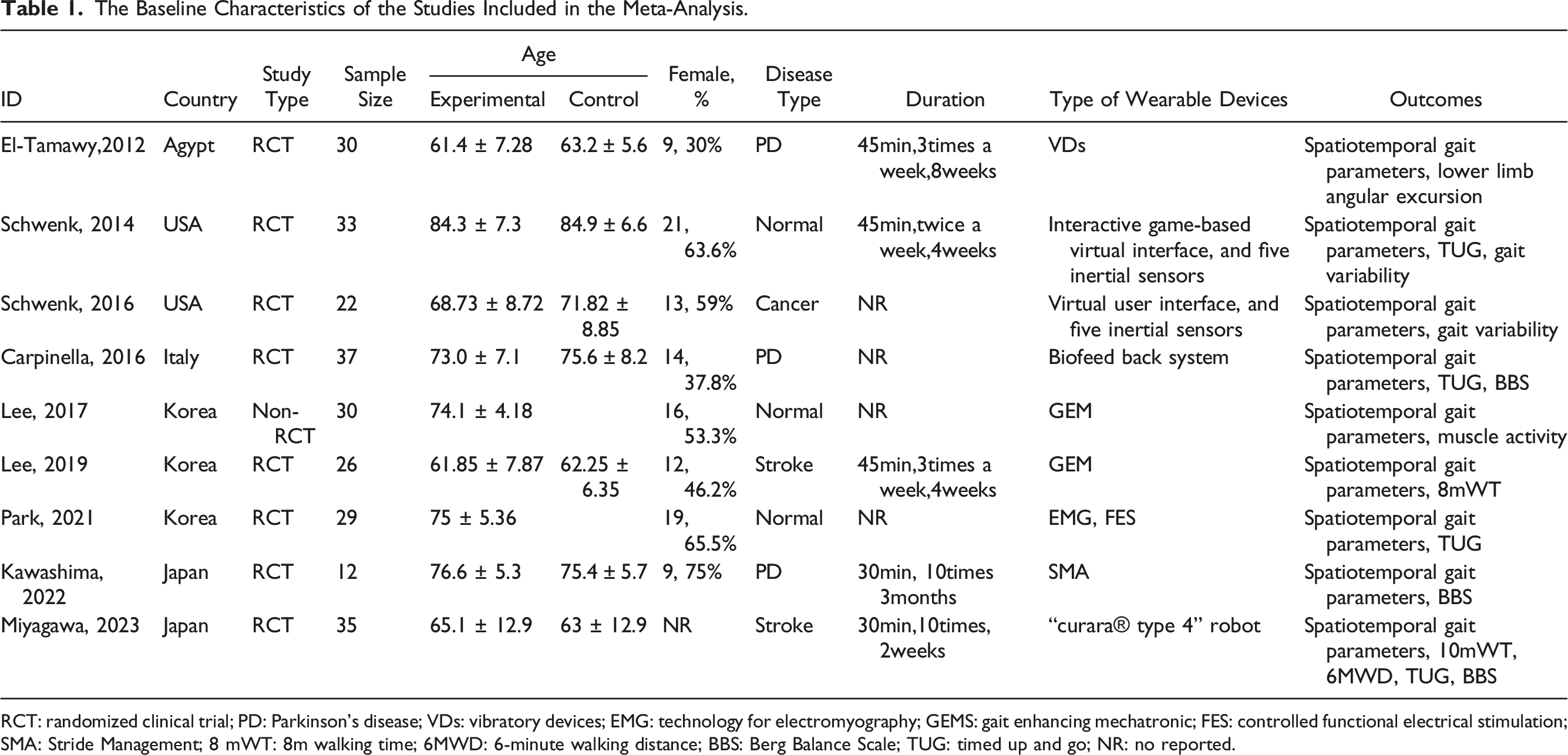
RCT: randomized clinical trial; PD: Parkinson’s disease; VDs: vibratory devices; EMG: technology for electromyography; GEMS: gait enhancing mechatronic; FES: controlled functional electrical stimulation; SMA: Stride Management; 8 mWT: 8m walking time; 6MWD: 6-minute walking distance; BBS: Berg Balance Scale; TUG: timed up and go; NR: no reported.
Quality Evaluation
The risk of bias (RoB) assessments of the studies, shown in Figure 2 and S1, suggested good quality across the included RCTs. Eight studies met at least four or all methodological criteria, implying a low risk of bias. Only one study presented indeterminate results due to incomplete outcome data and was rated as having moderate risk. Summary for the risk of bias in each study.
Overall Meta-Analysis
The meta-analysis estimated an overall pooled WMD of 0.12 (95% CI: 0.03 to 0.21, z = 2.66, P = 0.008), which suggests that, on average, wearable device-based walking programs could improve gait speed in older adults (Figure 3). Nevertheless, an I2 of 84% suggested considerable heterogeneity across the studies. Forest plot of wearable device-based walking programs on gait speed in older adults.
Subgroup Analysis
Results of Subgroup Analysis Based on Disease Type, Study Region, and Training Status.

WMD: Weighted mean differences; CI: confidence intervals.
Publication Bias
Funnel plot analysis indicated some asymmetry, yet Egger’s test (P = 0.95) suggested no significant publication bias, as demonstrated in Figure 4. Funnel plot of studies analyzing the impact of wearable device-based walking programs on gait speed in older adults.
Secondary Outcomes
For the Timed Up and Go test (TUG), the analyses showed non-significant reductions in TUG time (WMD: −2.83; 95% CI: −6.08 to 0.42) and no meaningful impact on gait variability (WMD: 0.26; 95% CI: −1.05 to 1.57) or step width (WMD: −0.36; 95% CI: −1.46 to 0.75). In contrast, positive effects of the wearable interventions were observed for balance (WMD: 1.93; 95% CI: 0.20 to 3.66), cadence (WMD: 6.31; 95% CI: 0.62 to 11.99), and stride length (WMD: 8.58; 95% CI: 3.04 to 14.12), highlighting the nuanced benefits of wearable interventions on various gait metrics (Figure 5). Forest plot on the impact of wearable device-based walking programs on (A) timed up and go test, (B) balance, (C) gait variability, (D) cadence, (E) step width and (F) stride length.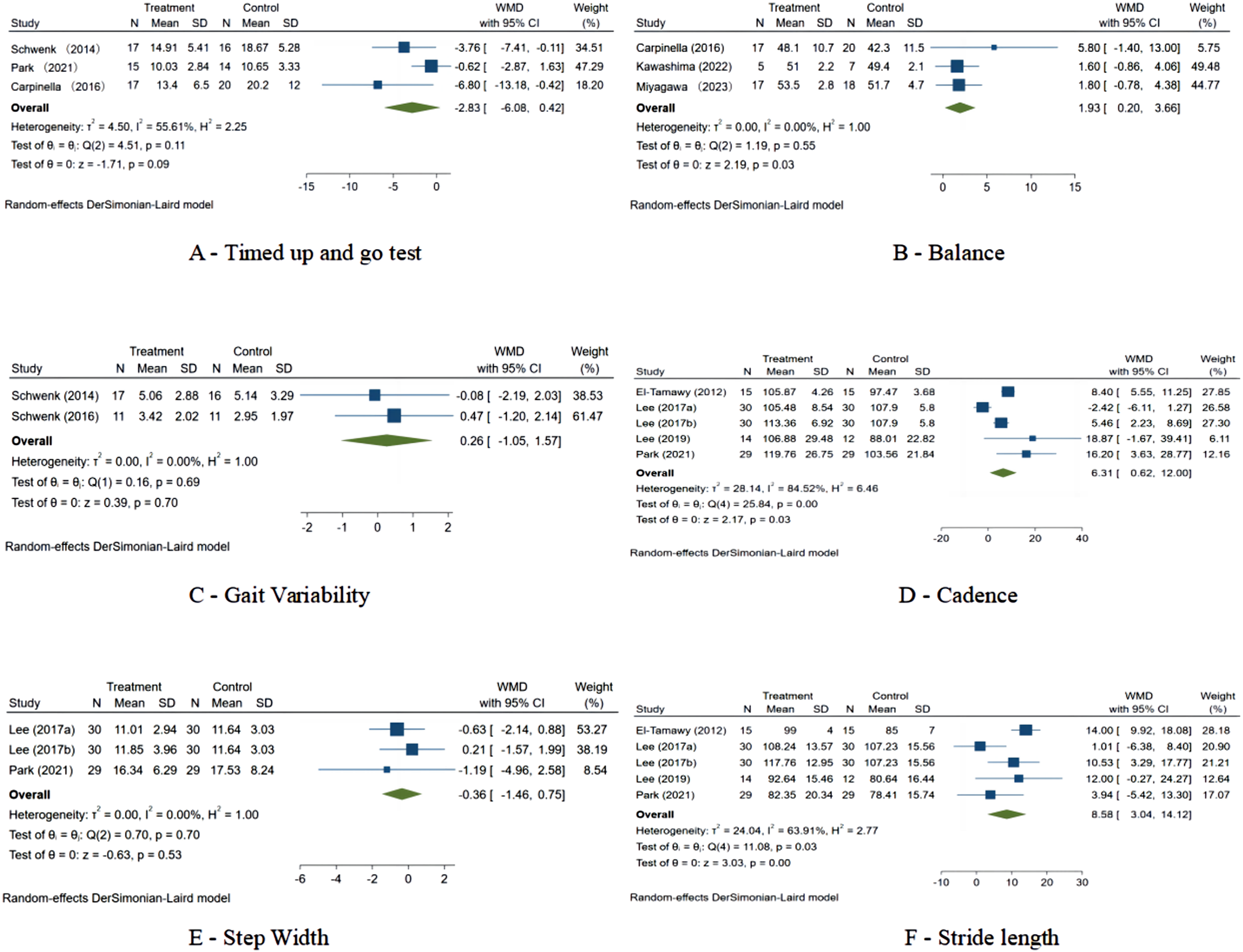
Discussion
We performed a systematic review and meta-analysis of wearable device-based walking programs on gait speed and various secondary outcomes in older adults, which demonstrated heterogeneous effects in different subgroups. In our primary analysis, we found a significant improvement in gait speed, but substantial heterogeneity indicated that effectiveness of the interventions varied. Additional subgroup analyses clarified these observations by revealing substantial advantages in people with PD and stroke, but less consistent effects in cancer patients or apparently healthy individuals. The results also varied depending on geography, and Afro-Asians improved much more than their Euramerican counterparts. Furthermore, the necessity of active participation in the training was emphasized as a key factor for reaping the benefits of such interventions. Secondary outcomes supported these findings, with stride length demonstrating significant improvements and step width non-significant changes, further emphasizing the multifaceted influence these programs have on ambulatory behavior. Despite the variability of results between studies, we are confident in concluding that wearable device-based programs show potential in improving gait and mobility in older people with no significant evidence of publication bias, especially when individualized to the participants executing the intervention.
We found that wearing these wearables and engaging in a walking program in comparison to no intervention may increase walking speed (WMD 0.12, 95% CI 0.03 to 0.21). This finding corroborates a prior report among rural older adults that found superior physical function outcomes in those exposed to a similar intervention. 27 Nonetheless, a trial involving participants with peripheral artery disease who walked more in the wearable condition demonstrated that benefits were not limited to those groups and could hypothetically be applied to a broad range or populations of older adults. 28 Furthermore, the lack of any substantial change in step width in our results differs from the broader mobility benefits, where wearable technology predicted fewer prospective falls, underlining the multifactorial influence of these interventions on multiple components of mobility beyond just gait speed. 29 Changes in both static and dynamic balance detected via wearable sensors have had a good agreement between multiple other studies when comparing across age groups, health statuses, and fall risk categories. They report significant improvements not only in static postural balance but also in some gait parameters after interventions based on wearable sensors. The clinical benefits of using wearable exoskeletons for post-stroke gait rehabilitation include mobility and walking speed improvements, motor function, balance, and endurance, which highlight the wide therapeutic potential of these technologies.30-32 Moreover, some instruments allow an extensive kinematic analysis during the capture of three-dimensional motion data, necessary to evaluate gait speed, rhythm, and stride length. They use real-time feedback systems to monitor and alert the user to deviations from the ideal gait pattern by vibration or tone, enabling ongoing correction and learning during walking practice.33-35 Advanced devices also sync with mobile apps and cloud-based platforms for constant monitoring and analysis of data. This enables the creation of individualized gait training programs that can be modified according to the recorded data, serving the ultimate goal of therapeutic outcome optimization for the user. 36
Previously, a network meta-analysis was reported on the benefit from exergaming with motion capture on functional mobility in the larger context of gerontology research which, despite being of little meaningful benefit, indicates an innovative pathway for geriatric care of the future using interactive technology. 37 Concurrently, post-stroke rehabilitation research further suggests wearable technologies as a crucial component in the surveillance and support of gait and mobility and strongly advocates their use in personalized clinical intervention. 38 The study on predictive analytics based on wearable technology for fall identification, and its corresponding fall risk prognostication, clearly implies the shift towards proactive geriatric care with a bunch of hidden risks which can be uncovered and neutralized and thereby delivers a health maintenance paradigm for preventive healthcare. 39 Furthermore, research on wearable sensor-based devices providing gait analysis in patients with dementia indicates that these tools can be used more universally to target a wide range of age-related mobility concerns and also holds the promise for early-stage disease detection and multidisciplinary management interventions. 40
This is supported by recent studies highlighting how wearable technologies are changing the landscape of healthcare, particularly the importance of healthcare wearables for patient care, monitoring, and intervention strategies, especially for the elderly. A further example is provided by a study characterizing the role of wearables in integrated care systems, showing how these devices, in combination with health coaching and digital education, are associated with significant improvements in outcomes for patients and in fostering more effective clinician-patient communication. 41 Another research document discusses the IoT and usage of wearable sensors for eldercare, and how they can be employed to continuously and reliably monitor key parameters required for the treatment of aging diseases and to promote active aging. These factors are key to problems including data quality and interoperability: the need for high-quality data standards and the impact of integrating data from wearable technology on healthcare equity and policy.42,43 Additionally, one study has described the importance of nurses in the implementation and evolution of wearable technology as well as the potential impact of nursing professionals on the development and implementation of these technologies to promote patient care and healthcare services. 44 The insights collectively call for a strategic integration and well-thought-out policy development regarding wearable technologies in healthcare, featuring multidisciplinary collaboration and ongoing studies to maximize the opportunities in enhancing patient care and clinical outcomes.
Although our study offers important new information on the effect of wearable device-based walking programs on gait speed in older adults, it is not without limitations. The specific demographic characteristics and health conditions of the participant population may limit the extent to which the findings can be generalized. This could potentially impact the results due to individual variances in technology familiarity and acceptance among participants as well. Furthermore, the range of wearable device types, intervention durations, and program intensities among included studies could lead to heterogeneity and affect the generalizability of pooled results. Publication bias might be introduced by the fact that most individual studies that formed the basis of this study rely on results published in the literature, and studies without significant results are less likely to be accepted for publication. Moreover, the long-term follow-up was not applicable for most of the studies included and this at least limits the concept concerning the enduring beneficial effects of these interventions. On the other hand, the influence of precise quantification of adherence to wearable device-based programs and its effect on outcomes was reported not in a consistent manner that could produce biased efficacy results.
Conclusions
Our findings display that wearable device-based walking programs are effective in improving gait speed amongst older adults, mainly in those with PD or stroke. This improvement underscores the potential of personalized, technology-enhanced interventions in geriatric rehabilitation. While the consequences imply sizeable heterogeneity, in all likelihood due to varying intervention protocols and demographic characteristics, they support the necessity of tailoring those interventions to individual health profiles to maximize their effectiveness. Further research must explore the precise mechanisms using the differential responses amongst subgroups, aiming to optimize intervention strategies for diverse growing old populations.
Supplemental Material
Supplemental Material - Impact of Wearable Device-Based Walking Programs on Gait Speed in Older Adults: A Systematic Review and Meta-Analysis
Supplemental Material for Impact of Wearable Device-Based Walking Programs on Gait Speed in Older Adults: A Systematic Review and Meta-Analysis by Ping Lai, Jing Zhang, Qing Lai, Jinfeng Li, and Zhengbo Liang in Geriatric Orthopaedic Surgery & Rehabilitation.
Footnotes
Author Contributions
All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. ZL conceived and designed the study. PL and JL retrieved literature. PL and JZ acquired the data. QL analyzed the data. ZL interpreted the study result. PL drafted the manuscript. All authors revised the manuscript and approved it for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has received the Sichuan Society of Gerontology Research Project (24SCLN062)
Registration
The study has been registered on the international prospective register of systematic reviews under registration number CRD42024519417.
Ethical Statement
Data Availability Statement
The data supporting the results of this study can be obtained from the corresponding authors upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.