
Abstract

Keywords
Introduction
There has been increasing interest and studies reporting the clinical and radiologic outcomes of minimally invasive surgery (MIS) to correct symptomatic forefoot pathology. These studies address frequent causes of foot pain such as hallux valgus and lesser toe deformities. 6 However, there are no clear standards or guidance to help surgeons optimize their operating room setup for minimally invasive foot surgery unlike other orthopaedic procedures.2,7
Optimizing the operating room setup for orthopaedic surgical procedures is essential for the safety of the patient, surgical team, and patient outcomes.5,9 Correct positioning of the surgeon facilitates better economy of movement and ergonomics, reducing discomfort and fatigue that may contribute to surgical errors.1,4 Consistent operative theater setup also reduces positioning time, which may improve operating room turnaround time.
Our aim is to share our experience and lessons learned regarding the optimal operating room setup for minimally invasive forefoot surgery (hallux valgus, cheilectomy, bunionette, distal minimally invasive metatarsal osteotomies, lesser toe correction), aiding early-stage surgeons. Figure 1 shows a diagram of the operating room setup, with an explanatory online video that we like to use.
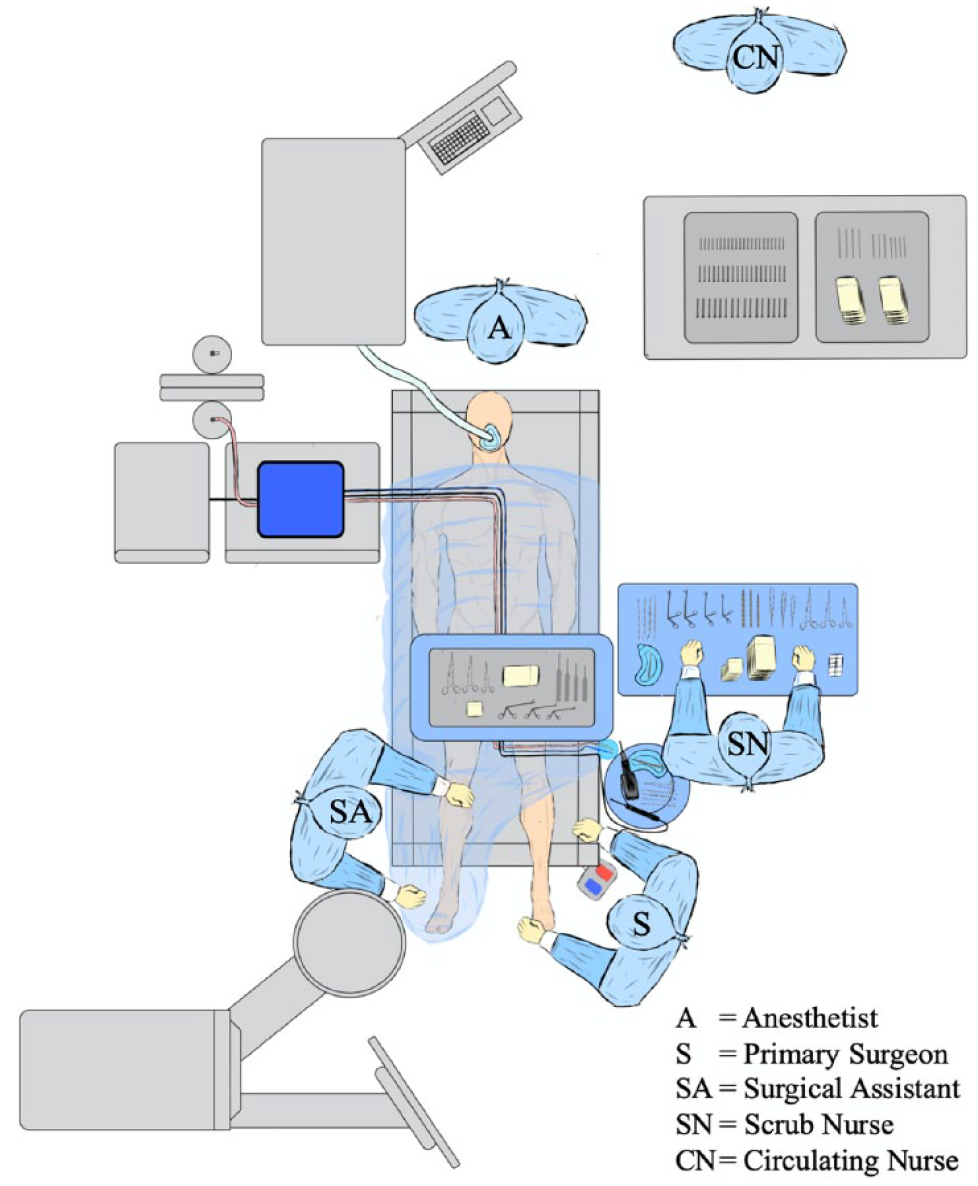
Diagrammatic representation of the operating room setup for percutaneous forefoot procedures. In this case the setup is shown for the left foot. The setup when operating on the right foot can be found in the supplemental material.
Patient
The majority of minimally invasive forefoot surgeries are easiest to perform when patients are supine, allowing easy access to the medial, dorsal, and lateral aspects of the foot.
The patient is positioned with both feet hanging from the end of the operating table by 6 inches. This allows for natural plantarflexion at the ankle and aids the surgeon to easily get a true anteroposterior image of the first ray. It is also possible to achieve a true lateral view intraoperatively by supination at the ankle. If the ankle and hip are stiff, a true lateral can be achieved by externally rotating and flexing the knee. No sandbag is used as it can hinder external rotation, which is needed to obtain a lateral radiographic image. The amount of external rotation should be checked prior to operating as surgeons who use a large c-arm may struggle to achieve a true lateral and may find a mini c-arm easier to use.
To aid patient positioning, a side support suspends the left leg (Figure 2) when operating on the right foot, creating ample working space for the surgeon between the legs and minimizing the risk of displacing the left leg from the bed. After completing the right foot procedure, the left leg can be easily returned to the bed for bilateral procedures. Another option is using a table with split leg supports to move the nonoperative leg away from the surgical field. Only the foot being operated on should be prepped and draped, and bilateral draping (as shown in the video and images) is only needed if performing bilateral surgery.

Clinical photograph demonstrating the side support to suspend the left leg to create space to operate on the right foot.
Tourniquet choice is optional and all patients should have additional warming and venous thromboembolism prophylaxis as per hospital guidance. It is important to use abundant cool saline irrigation, which is essential to reduce the risk of thermal injury. 8 It is important to protect all relevant pressure points to reduce the risk of pain and peripheral nerve injury.
Theater Team
Orientation and ergonomic positioning of the surgical team members with respect to the patient facilitates clear verbal communication during the procedure, effective division of labor, reduced risk of desterilization, and concurrent activities.
Surgeon
Surgeon positioning is very important to allow for full access to the first ray using medial incisions and puts their dominant hand in a relaxed ergonomic position to operate, allowing maximum pronation/supination and economy of movement. Surgeon positioning depends on the hand dominance of the surgeon and the operating side. Correct positioning of the table height provides proper ergonomic support and reduces the risk of occupational musculoskeletal injuries common across all surgical disciplines. 3
A right-handed surgeon should position themselves on the left side of the patient’s foot when operating. For left foot hallux valgus surgery, the surgeon stands to the left of the patient. However, for right foot surgery, it is best for the surgeon to position themselves between the patient’s feet, allowing their dominant hand to work comfortably. Standing on the left side benefits the right-handed surgeon, as it frees their dominant hand to fix the osteotomy while using the left hand to correct the deformity.
When a surgeon is performing DMMO, or lesser toe corrections, then it is easier to stand at the end of the patient facing the foot, and the surgeon should stand wherever is most ergonomic to complete the procedure. We recommend standing to perform MIS forefoot surgery; however, we acknowledge that some surgeons may prefer to sit down, and this setup can be used with a sitting surgeon.
Surgical Assistant
The surgical assistant stands on the right-hand side of the patient next to the waist/thigh region. This facilitates access to the power instruments that are used to manipulate K-wires without impeding the primary surgeon’s access.
Scrub team
The scrub team have their primary tray at 90 degrees to the operating table at the level of the patient’s waist and face toward the feet. An adjustable Mayo stand is placed over the patient’s thighs at a suitable height for the surgeon, as depicted in Figures 3 and 4. We use a large standard hip replacement Mayo stand, which enables the scrub team easy access to the primary surgeon and surgical instruments.

Clinical photograph of the operating room setup for percutaneous forefoot procedures.

Clinical photograph of commonly used percutaneous surgery instruments.
The Mayo stand should have the most frequently used instruments, which include the beaver blade, range of periosteal elevators and reduction instruments, and artery clip to protect the skin during insertion of the burr or power instruments.
A sterile surgical bowl should be placed between the Mayo stand and the surgeon at hip height to store the power instruments such as wire drivers and burr handpiece. This also safeguards against falling off the bed, inadvertent activation, or bowl perforation, which could compromise the surgical field’s sterility.
Facilitating Teaching
Optimizing teaching and facilitating learning for trainees and fellows is particularly important for MIS given the recognized challenges associated with developing these surgical skills. When teaching MIS procedures, we suggest the trainee stand to the right-hand side of the surgeon to facilitate optimal access to the foot and vision of the operative field.
Anesthetist
The anesthetist and all associated equipment should be positioned by the patient’s head, with adequate clearance to the scrub nurse to reduce the risk of contamination. For forefoot surgery, it is essential that the foot and surgical instruments are well within the laminar flow box.
Equipment
Location of the ancillary equipment is important to facilitate use of the power instruments and burr, optimize surgical team ergonomics, reduce risk of tangled cables, and reduce risk of inadvertent desterilization.
Figure 1 demonstrates that the power consoles for the burr and the handsets are located to the right of the patient at the shoulder level. The cables for the burr and handsets should be run at 90 degrees to the patient's sternum and then clipped longitudinally along the midline underneath the Mayo stand, before being stored in a sterile bowl to the left of the patient between the scrub nurse and the surgeon.
High-intensity lighting is not required for percutaneous surgery, and conversely the bright pendant lights can interfere with image intensifier positioning and laminar air flow. Standard lighting is usually enough to mark skin and make incisions allowing the pendant lights to be positioned away from the surgical area, preventing interference and glare.
Surgical implants and instruments such as screws and K-wires are positioned outside the sterile field in an easily accessible fashion in order to reduce delays associated with finding and opening. This also reduces footfall entering and leaving theater, which has been associated with disruption of laminar air flow and increased risk of infection.
Fluoroscopy
The ability to consistently achieve anteroposterior and lateral radiographs is essential for MIS forefoot surgery. A mini c-arm is positioned to the right of the patient's foot, with the plate/drum serving as a table for the forefoot. Bringing it in from the right maintains a safe distance from the surgeon, ensuring ergonomic comfort. This setup allows the surgeon to freely move around the foot and access all necessary areas according to the operative plan. Alternatively, the same imaging can be obtained using a conventional C-arm as per Figure 5. We preferentially use a mini c-arm for all minimally invasive forefoot procedures as it is easier to manipulate and provides lower radiation exposure to the patient and theater team.

Clinical photographs demonstrating the positioning for intraoperative fluoroscopy using (top) a mini c-arm or (bottom) conventional c-arm.
The screen should be positioned at the foot of the bed so that it is clearly visible to the surgeon in all positions. At the start of the procedure, the image should be correctly orientated, mirrored and magnified and, ideally, very little movement of the machine should be required to gain anteroposterior and lateral images throughout the case.
Conclusion
Optimal operating room setup and positioning for minimally invasive surgical procedures may positively impact surgical efficiency, utilization time, surgical team ergonomics, and patient outcomes.
Supplemental Material
sj-jpg-2-fao-10.1177_24730114231198235 – Supplemental material for Optimizing the Operating Room Setup for Minimally Invasive Forefoot Surgery: Technical Tip
Supplemental material, sj-jpg-2-fao-10.1177_24730114231198235 for Optimizing the Operating Room Setup for Minimally Invasive Forefoot Surgery: Technical Tip by Thomas L. Lewis, Yousif Alkhalfan, Gabriel Ferraz Ferreira, Gustavo Araujo Nunes, Peter Lam and Robbie Ray in Foot & Ankle Orthopaedics
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231198235 – Supplemental material for Optimizing the Operating Room Setup for Minimally Invasive Forefoot Surgery: Technical Tip
Supplemental material, sj-pdf-1-fao-10.1177_24730114231198235 for Optimizing the Operating Room Setup for Minimally Invasive Forefoot Surgery: Technical Tip by Thomas L. Lewis, Yousif Alkhalfan, Gabriel Ferraz Ferreira, Gustavo Araujo Nunes, Peter Lam and Robbie Ray in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
A supplement video for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.