
Abstract
Keywords
Introduction
In the setting of ankle fracture-dislocation, achieving timely anatomic reduction is crucial in order to alleviate pressure on soft tissues and prevent skin necrosis and infection. 19 Occasionally, displaced bony and soft tissue structures surrounding the tibiofibular joint may prevent reduction. Such described associated injuries include anterior and posterior fibular dislocation, deltoid ligament incarceration, as well as extensor digitorum and posterior tibial tendon (PTT) entrapment. 3,4,10,14 -17 In the case of PTT dislocation, the tendon more commonly dislocates anteriorly over the medial malleolus through ruptured flexor retinaculum. 9 However, there are descriptions of a dislocation of the PTT around the posterior malleolus with subsequent passage of the tendon posteriorly to anteriorly through a concomitantly ruptured and widened tibiofibular syndesmosis. 1,2,5,6,8,10 -13,17,18,20 In some instances, the tendon even extends proximally into the interosseous membrane. In such instances, the PTT may course from lateral to medial along the anterior aspect of the tibia. Such inter-positioning forces anterolateral subluxation of the talus and medial joint space widening, thus blocking closed anatomic reduction.
In recent case reports, failure to recognize trans-syndesmotic PTT dislocation at the time of definitive internal fixation has involved patients undergoing multiple revision surgeries with subsequent increased morbidity. 8 As a consequence of unrecognized diagnosis, published postoperative sequelae have included significant long-term stiffness, extensive soft tissue compromise requiring coverage, as well as equinovarus and clawtoe deformity secondary to ischemic deep posterior compartment contracture. 1,6,13,17
In this case series, recognition of trans-syndesmotic PTT dislocation was achieved at the time of initial open definitive fixation, in 1 case following external fixator removal and planned open reduction and internal fixation (ORIF), allowing for appropriate anatomic reduction and avoidance of additional operative procedures. This case series contributes to a limited body of literature describing and facilitating prompt recognition of this rare injury pattern and reinforces previous recommendations advocating for the benefits of early diagnosis and appropriate treatment.
Case 1
Patient is a 33-year-old man who sustained an open left ankle trimalleolar fracture dislocation following a motorcycle accident. The patient was initially seen at an outside hospital where the ankle was splinted in situ and patient was given tetanus and IV cefazolin. He was transferred to our institution where the left lower extremity was found to have a 7-cm open wound with extruded distal tibial plafond medially at the ankle joint and significant periosteal stripping (Gustillo Anderson Type 3A). His left lower extremity was neurovascularly intact. Fluoroscopic imaging demonstrated a trimalleolar ankle fracture with anterolateral tibiotalar dislocation (Figure 1). The ankle was reduced and splinted in the emergency department and nonweightbearing radiographs were obtained demonstrating significant improvement of alignment compared to the original injury films. However, the medial malleolus remained displaced and anterior to the tibia. He was taken to the operating room for urgent irrigation and debridement of the left ankle with application of an external fixator 5 hours after arrival to the emergency department. Maintenance of the reduction was difficult, and it was noted intraoperatively that there was a tendon interposed between the medial malleolus fracture fragment and the tibial metaphysis coursing over the anterior tibia. At the time of this initial operative procedure, the unidentified tendon was brought anteromedially through the fractured medial malleolus so that the medial malleolus could be reduced, and the external fixator was applied. The tibiotalar joint was adequately reduced with improved length and coronal alignment. The medial malleolar fracture remained nonreduced secondary to an unrecognized trans-syndesmotic PTT dislocation, having occurred at the time of injury prior to initial reduction in the emergency department (Figure 2). Postoperative computed tomography (CT) was performed for preoperative planning.

Anteroposterior and lateral views of left ankle demonstrating dislocation of the ankle mortise with comminuted fracture of the fibula, fracture of the medial malleolus, and anterolateral subluxation of the talus. Closed reduction demonstrates improved length and coronal alignment with persistent anterior displacement of medial malleolus.

Anteroposterior fluoroscopy following external fixation demonstrates improvement in ankle mortise and fibular alignment with persistent medial clear space widening and gapping at medial malleolus fracture site.
The patient returned to the operating room 8 days later for definitive fixation when soft tissue swelling allowed. The medial traumatic arthrotomy was opened and thoroughly irrigated. The tibiotalar joint was inspected, and there was no evidence of impaction fracture (Figure 3). Again, the dislocated tendon was noted at the medial malleolar fracture site. Tracing the tendon distally to the navicular bone identified it as likely the posterior tibial tendon, and the groove for the posterior tibial tendon was empty on palpation. However, the tendon was unable to be reduced by simple translation posteriorly to the medial malleolus, and it was noted that the tendon entered the operative exposure proximally on the anterior tibial surface from lateral to medial. Upon retrospective review of the CT scan obtained preoperatively, a tendon can be seen emerging through the tibiofibular interosseous space, coursing distally and medially along the anterior tibia (Figure 4). The tendon was successfully reduced by dislocating the talus laterally and bringing the PTT anterolaterally, then finally posteriorly through the disrupted syndesmosis. The tendon was frayed but intact, and damaged tendon was debrided (Video Supplementary Material). Fracture fixation then proceeded in standard fashion.

Computed tomography with bone window in coronal and sagittal planes demonstrate fractures of fibula, medial, and posterior malleoli. No evidence of impaction fracture.
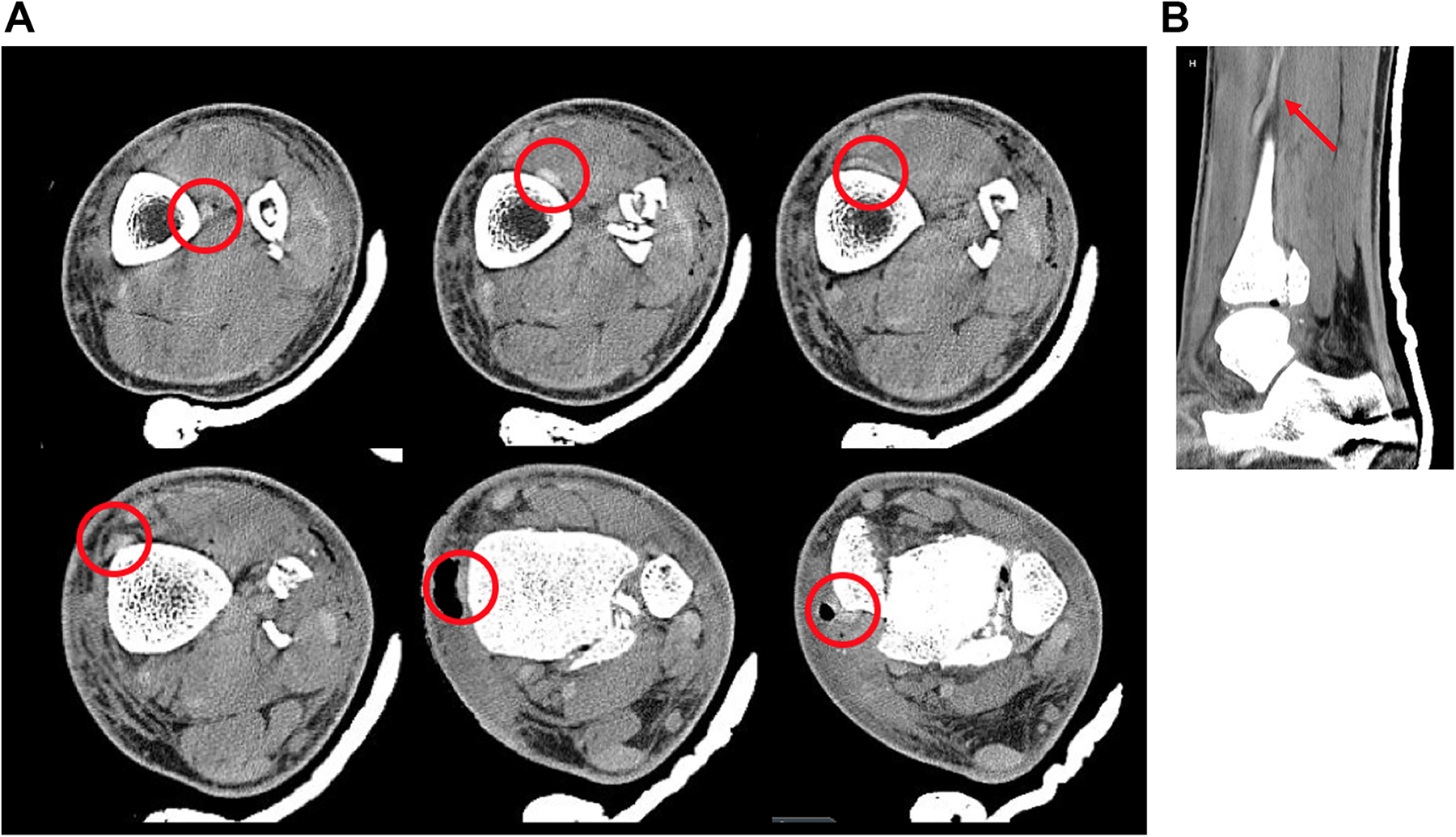
(A) Axial CT sections (proximal to distal in direction of top left to bottom right) demonstrating PTT passing through interosseous space across the anterior surface of the tibia, displacing the medial malleolar fragment anteriorly. (B) Sagittal CT section showing PTT penetrating tibiofibular interosseous space. (CT, computed tomography; PTT, posterior tibial tendon.)
At 3-month follow-up, the patient demonstrated no issues with pain control and has been weight bearing as tolerated, no longer requiring a CAM boot. Incisions were well healed with no concerns for infection. Physical examination of the ankle demonstrated 4/5 strength of the PTT, and was neurovascularly intact. Radiographs obtained in the clinic demonstrated maintained alignment of the ankle mortise, with early facture healing and no evidence of hardware failure or loosening (Figure 5).

Weightbearing anteroposterior and lateral radiographs of the left ankle 3 months following internal fixation. Fibula fracture stabilized with bridge plating and syndesmotic screws. Medial and posterior malleoli were anatomically reduced and fixed using lag screw technique.
Case 2
Patient is a 68-year-old man who fell while on his motorcycle and sustained an ankle dislocation. Closed reduction attempts in the emergency department were unsuccessful. Initial radiographs of the knee and ankle depict anterolateral subluxation of the talus with medial clear space widening, as well as a proximal fibular fracture consistent with a Maisonneuve fracture mechanism (Figure 6). The patient was brought to the operating room for open reduction. However, there was necrotic-appearing skin overlying the medial malleolus as the ankle had been dislocated for approximately 48 hours. A medial approach was performed and a tendinous structure was found coursing distal-medial to proximal-lateral over the talar dome. This tendon was irreducible from this approach; therefore, a lateral approach to the syndesmosis was performed, and the syndesmosis was found to be completely disrupted, with a tendinous structure in the syndesmosis preventing reduction. A third incision was made proximal to the necrotic tissue on the medial side, and the PTT was noted to be absent. The previously seen tendon was identified as the PTT and guided anterior to posterior through the syndesmosis, and the ankle reduced spontaneously on return of the PTT to its anatomic location. The syndesmosis was then stabilized and deltoid ligament was repaired. With the diagnosis confirmed operatively, retrospective review of CT imaging of the ankle obtained preoperatively demonstrates the posterior tibial tendon entrapped within the syndesmosis and entering the tibiotalar joint space (Figure 7).

(A) AP and lateral radiographs of the left ankle demonstrating dislocation of the tibiotalar joint with anterolateral displacement of the talus and medial clear space widening. (B) AP and lateral radiographs of the left knee and proximal tibia and fibula demonstrating proximal fibular fracture consistent with Maisonneuve fracture mechanism. (AP, anteroposterior.)

(A) Axial CT sections of ankle (proximal to distal in direction of top-left to bottom-right) demonstrating PTT within the interosseous space proximally. The tendon enters the tibiotalar joint space distally, displacing the talus anterolaterally. (B) CT in coronal plane demonstrating PTT entering the tibiotalar joint space with anterolateral displacement of the talus. (CT, computed tomography; PTT, posterior tibial tendon.)
Eight months postoperatively, the patient was doing well and demonstrated 5/5 strength of the PTT with full ankle range of motion. The ankle mortise was well maintained with no evidence of hardware loosening or failure (Figure 8).

Anteroposterior and lateral radiographs of the left ankle following open reduction and syndesmotic fixation demonstrating uniform spacing of the ankle mortise with no evidence of hardware loosening or failure.
Discussion
Dislocation of the PTT through the tibiofibular interosseous space is a rare mechanism blocking closed ankle reduction. Such an injury was first described by Böhler et al 2 in 1936. Several isolated case reports, separated by decades, have documented this same injury pattern at the time of surgery. 5,10 -12,20 Although each of these reports demonstrated timely open reduction of the ankle joint, PTT interposition in the syndesmotic joint space with associated anterolateral talar dislocation caused initial failed closed reduction.
Trividi et al 18 recognized persistent PTT dislocation on CT immediately following primary ORIF and underwent timely reoperation and successful anatomic reduction. However, other case reports have unfortunately noted delayed diagnosis of trans-syndesmotic PTT dislocation after ORIF, and reported subsequent poor outcomes and morbidity.
Heini et al 6 reported an ankle fracture requiring significant force to achieve satisfactory open reduction and fixation. Postoperative loss of syndesmotic fixation and recurrent anterolateral talar subluxation led to an intraoperative discovery of an initially unrecognized PTT coursing through the tibiofibular interosseous space, 8 months following initial injury. After PTT reduction through multiple staged revision procedures, the patient demonstrated improvement, although sustained significant long-term reduction in joint mobility.
Anderson et al 1 discovered trans-syndesmotic dislocation of the PTT at the time of salvage ankle arthrodesis surgery 1 year following initial injury. Noting severe calf atrophy, as well as equinovarus and clawtoe contracture, the author performed a deep posterior compartment exploration and discovered the tendon wrapped laterally around the tibia emerging through dense scar tissue in the syndesmosis. During the interval period, the patient had undergone multiple revisions for loosened hardware, ankle mortise widening, and talar tilting.
Lacasse et al 8 recognized the PTT coursing through the tibiofibular syndesmosis on magnetic resonance imaging (MRI) 4 months after initial ORIF. Correction required extensive debridement of the syndesmosis, including hardware removal and circumferential release of the ankle joint to allow for reduction of the PTT. Following revision surgery, pain improved but ankle dorsiflexion remained limited at 5 degrees.
In a recent case report by Thoreau et al, 17 despite extensive soft tissue repair including the deltoid ligament and syndesmosis, failure to initially recognize and reduce a PTT dislocation during primary ORIF led to reoperation 1 week later, including extensive dissection requiring a cutaneous skin flap. The PTT dislocation was ultimately visualized using CT in the setting of persistent anterolateral talar subluxation.
Most recently, Sato et al 13 described a multistage case in which recognition and reduction of a PTT trans-syndesmotic dislocation was achieved only after a third attempt at open reduction involving full operative exposure of the PTT, approximately 3 months after the initial injury. The abnormal tendon course was revealed via CT and MRI in the setting of the patient having difficulty with ankle inversion.
The location of PTT entrapment is influenced by the amount of energy associated with the injury. 1 On review of associated high-energy injuries with interosseous PTT location, Thoreau et al 17 identified common features to PTT dislocation through the ankle syndesmosis including high-energy trauma, AO fibula type C fracture, distal tibiofibular dislocation, and lateral talar translation with an increased internal clear space (or malleolar fracture). Both reported cases in our series of PTT dislocations into the syndesmosis features all characteristics formally outlined by Thoreau et al. 17
Of note in the above presented cases, attempting posterior translation of the PTT (indicated for dislocation directly anterior to the medial malleolus) was met with significant resistance. Furthermore, anatomic reduction of the medial malleolar fragment and tibiotalar joint were similarly difficult. On reduction of the PTT, subsequent medial malleolar and tibiotalar reductions required minimal exertion. We emphasize that a failed closed reduction, a persistently wide distal tibiofibular space, and/or excessive force requirements for satisfactory ankle joint reduction (open or closed) should raise clinical suspicion for possible PTT entrapment.
As demonstrated in previously mentioned case reports, CT imaging has proven diagnostic utility in troubleshooting fractures and dislocations postoperatively. Although we were fortunate to recognize and reduce both tendon dislocations intraoperatively, subsequent review of the CT imaging revealed the abnormal course of the PTT. Had we noticed the PTT dislocation on imaging at the time of external fixation during the first case, we would have more quickly achieved appropriate reduction, minimizing tourniquet and operating room time during subsequent definitive operative fixation. With heightened clinical suspicion afforded by characteristics formally outlined by Thoreau et al, 17 obtaining CT imaging proves useful in identifying PTT displacement and planning for appropriate reduction prior to definitive operative fixation. Ultrasonography and MRI represent additional imaging modalities well described for assessing tendon and ligament pathology. 7 However, MRI is less accessible and undesirable when an external fixator has been emergently placed. Furthermore, ultrasonography becomes challenging in the acute traumatic setting secondary to edema, air in the soft tissues, and compromised skin condition. 17 Such planning will aid in reducing anesthetic and tourniquet time, as well as incisional exposure and excessive soft tissue dissection. As noted previously, delayed recognition of PTT dislocation is associated with significant morbidity and repeat operations.
To our knowledge, we present the most up-to-date review of cases of irreducible ankle fractures due to PTT trans-syndesmotic dislocation reported in the literature. We highlight the morbidity associated with delayed diagnosis and emphasize the injury pattern and difficulty in reduction that should alert the orthopedic surgeon to the possibility of this diagnosis. Given the increase in reports of this relatively rare injury in the past decade, we suspect that the incidence of this injury pattern is underreported; however, recognition in the past has been low. With the increasing use of cross-sectional imaging for complex fractures and irreducible dislocations, and heightened suspicion of this injury pattern, early recognition, and the subsequent reduction in patient morbidity are achievable.
Conclusion
Irreducible ankle fractures and dislocations should raise awareness to possible tendon incarceration. Moreover, an irreducible ankle with an AO fibula type C fracture pattern and lateral talar dislocation or distal tibiofibular dislocation and lateral talar translation in a high-energy injury mechanism warrants heightened suspicion for PTT dislocation through the tibiofibular interosseous space. Reduction should be carefully performed with awareness of proper PTT position. CT imaging can facilitate identification of this injury pattern and aid in preoperative planning. Early recognition may improve patient outcomes and avoid the need for future exploratory or revision surgery.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211000297 - Irreducible Fractures and Dislocations of the Ankle Associated With Entrapment of the Posterior Tibial Tendon Within the Tibiofibular Interosseous Space:: A Case Series and Literature Review
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211000297 for Irreducible Fractures and Dislocations of the Ankle Associated With Entrapment of the Posterior Tibial Tendon Within the Tibiofibular Interosseous Space:: A Case Series and Literature Review by Eric Colomb, Stefano Muscatelli, Joel G. Morash, Eileen A. Crawford, James R. Holmes and David M. Walton in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was waived by University of Michigan Health System (UMHS) Medical School Institutional Review Board (IRBMED) because proposed case study does not constitute a systematic investigation, and is intended as an interesting example for educational purposes [HUM00187820] 9/3/2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
A supplemental video for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.