
Abstract

Introduction
Ankle and hindfoot fractures can result in tendon tears, entrapment, or dislocation. Unrecognized, it may lead to irreducible ankle fracture-dislocations, multiple unnecessary surgeries, and poor outcomes, such as persistent pain, deformity, and arthritis.1,2 Although posterior tibia tendon (PTT) dislocation/entrapment with ankle fractures has been previously described in the literature, many cases are likely undiagnosed. A total of 21 cases have been reported in the literature, most involving intrasyndesmotic entrapment. Intra-articular dislocations, such as in the present case, are rarer. 2 In most cases, PTT entrapment presented as persistent ankle and talar subluxation, often associated with medial clear space widening. Treatment was delayed in approximately half of the cases, requiring additional revision surgery.
We report a case of intra-articular PTT dislocation associated with an ankle fracture that mimicked syndesmotic malreduction. PTT entrapment was only identified after failed revision surgery focusing on syndesmotic reduction. Successful outcomes were achieved after the second revision surgery, which entailed tendon excision/reconstruction and flexor digitorum longus transfer.
Case Report
The patient is a 22-year-old man without prior surgical history who presented to the emergency department after sustaining a closed ankle fracture-dislocation from jumping and landing on his left foot. On physical examination, he was neurovascularly intact with a visible ankle deformity, diffuse swelling, and tenderness to palpation. Radiographs revealed a dislocated pronation external rotation type bimalleolar ankle fracture with syndesmotic widening (Figure 1). Closed reduction and splinting resulted in partial improvement (Figure 1).

Initial left ankle radiographs demonstrating a pronation-external rotation stage III injury according to Lauge-Hansen classification: (A) anteroposterior view, (B) lateral view. Postreduction radiographs show improved but suboptimal alignment: (C) anteroposterior view, (D) lateral view.
The patient underwent open reduction and internal fixation the following day. The medial malleolus was fixed with 2 screws, the fibula with a lag screw and a one-third plate, and the syndesmosis stabilized with a suture-button device (Figure 2).

Intraoperative (A) anteroposterior view and (B) lateral view. Postoperative left radiographs showing an adequately placed hardware with persistent anterior talar subluxation: (C) anteroposterior view, (D) lateral view, also demonstrating anterior fibular translation (*).
At the 2-week follow-up, radiographs revealed persistent anterior talar subluxation (Figure 2). Ankle computed tomography (CT) confirmed this along with an anteriorly malreduced fibula within the incisura (Figure 3). Revision surgery was undertaken for presumptive syndesmotic malreduction. The suture-button device was removed. Alignment improved following repeated manipulation, with closed syndesmotic reduction, and a new suture-button device was placed.

Bilateral ankle computed tomographic scan. (A) Axial view showing malpositioning of the left fibula within the incisura, mimicking syndesmotic malreduction. (B) Sagittal view showing anterior translation of the talus relative to the tibia.
At 6 weeks, radiographs showed persistent anterior talar subluxation. Magnetic resonance imaging revealed intra-articular PTT dislocation. The tendon was displaced medially above the ankle and across the tibiotalar joint, showing signs of tearing (Figure 4). Retrospective review of the initial ankle CT revealed that PTT entrapment was visible but not detected (Figure 5).

Left ankle magnetic resonance image showing intra-articular dislocation of the posterior tibia tendon (*). (A) Axial proton density–weighted sequence. (B) Coronal T1-weighted sequence. (C) Sagittal T1-weighted sequence.
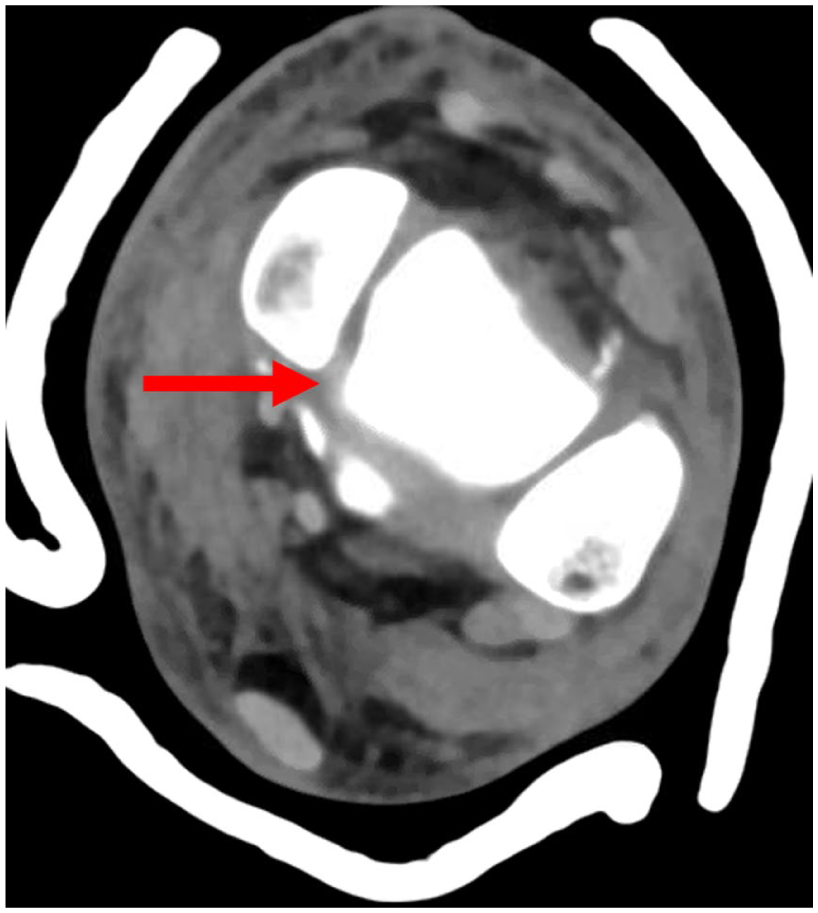
Axial view of initial left ankle computed tomographic scan showing the intra-articular dislocation of the posterior tibia tendon (arrow).
The patient was subsequently referred to the senior author (J.Y.K.), who performed additional surgery approximately 3 months after the initial injury. Posterior medial ankle exploration revealed a frayed, atrophic, and dislocated PTT within the ankle joint, coursing beneath the deep deltoid ligament (Figure 6). The rupture was deemed irreparable, necessitating excision of the diseased portion and flexor digitorum longus transfer with proximal tenodesis of healthy PTT. Fluoroscopy demonstrated proper mortise alignment.

Intraoperative view of the frayed posterior tibia tendon showing (A) its abnormal intra-articular course and (B) its rupture.
Six months following his index procedure, the patient was pain free, back to jogging, and could perform single-leg heel rise (Figure 7). Final radiographs demonstrated complete osseous healing with anatomically aligned mortise (Figure 8).

Patient performing single-leg heel rise test at last follow-up, demonstrating functional flexor digitorum longus transfer.

Six-month postoperative left ankle radiographs showing restored ankle joint syndesmotic alignment: (A) anteroposterior view, (B) lateral view.
Discussion
Cases of irreducible ankle fractures due to soft tissue interposition, such as involving the PTT, extensor digitorum tendon, or deltoid ligament,1,3 remain an underrecognized problem. A systematic review reported a missed diagnosis in 60% of cases.2,4-6 Given the relative rarity, the current literature largely consists of case reports and short case series.
Irreducible ankle fractures are rare and accurate identification of the underlying cause is essential to ensure proper management. As such, an increased level of suspicion should arise when an adequate closed reduction is unobtainable, especially in the hands of an experienced surgeon and with adequate anesthetic/analgesia administered. 5 Dislocation of the PTT typically occurs following pronation-external rotation ankle injuries such as demonstrated in the case presented. 6 Other common features include high-energy trauma, AO 44-C2 fracture, distal tibiofibular dislocation, and lateral talar translation with increased medial clear space. 3
In the case presented, the PTT entrapment created the appearance of syndesmotic malreduction due to fibular malalignment and anterior talar subluxation, similar to the case reported by Nguyen Van and Nguyen Nang. 4 Cases of anterior talar subluxation in the setting of syndesmotic malreduction have been previously described. 7 Identifying the cause of talar subluxation is essential to distinguish between syndesmotic malreduction and PTT entrapment. The initial revision surgery resulted in little improvement in sagittal talar alignment given the still occult PTT dislocation not being addressed. Although a syndesmotic injury was expected because of the fracture pattern, persistent malreduction despite adequate fixation suggested that another structure was obstructing anatomic mortise alignment.
Surgeons tend to focus solely on osseous structures when analyzing preoperative CT imaging for ankle fractures. Although appropriate, soft-tissue evaluation should not be overlooked, especially in cases of challenging reduction. In addition to ankle fractures, recent evidence suggests that PTT entrapment may be underdiagnosed in tibial plafond fractures. In a study of 363 surgically treated posterior malleolar and pilon fractures, Aamir et al 8 found a 22% incidence of PTT entrapment on preoperative CT. This demonstrates that tendon entrapment can be identified directly on CT without necessarily requiring magnetic resonance imaging, and its relatively high incidence underlines the importance of routinely assessing for PTT entrapment during preoperative planning.
To evaluate PTT dislocation on CT, Thoreau et al 3 recommend first to inspect its anatomical position, the retromalleolar groove, and if absent, to explore common dislocation. Reported dislocations in the literature are within the tibiofibular space (61%), tibiotalar joint (11.1%), a combination of both (16.7%), or within medial and posterior malleolar fractures (11.1%).
Conclusion
This case highlights the importance of identifying the underlying cause of a failed reduction in ankle fractures. Posterior tibial tendon entrapment should be considered when adequate closed reduction is unobtainable. Advanced imaging (and careful review of preoperative CT for tendon position) may be warranted when talar alignment remains abnormal despite apparently adequate syndesmotic fixation. Careful systematic examination for tendon entrapment should be undertaken whenever preoperative CT is obtained, especially in cases of initial fracture-dislocation. Increased vigilance is warranted when an anatomic mortise reduction cannot be achieved intraoperatively despite appropriate operative technique.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251386023 – Supplemental material for Intra-articular Posterior Tibial Tendon Entrapment in an Ankle Fracture Mimicking Syndesmotic Malreduction: A Case Report
Supplemental material, sj-pdf-1-fao-10.1177_24730114251386023 for Intra-articular Posterior Tibial Tendon Entrapment in an Ankle Fracture Mimicking Syndesmotic Malreduction: A Case Report by Amal Chidda, Jaeyoung Kim, Ivan Golub, Bonnie Y. Chien and John Y. Kwon in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval was not required for this case report. The patient provided informed consent for publication of this case report.
Data Availability Statement
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.