
Abstract
Ankle fractures are common musculoskeletal injuries that may result in tibiotalar joint dislocations. Ankle fracture-dislocations occur via similar mechanisms as ankle fractures, although the persistence or magnitude of the deforming force is sufficient to disrupt any remaining bony or soft-tissue stability. Ankle fracture-dislocations likely represent distinct clinical entities, as the pathology, management, and patient outcomes following these injuries differ from those seen in more common ankle fractures without dislocation. Ankle fracture-dislocations have higher rates of concomitant injury including open fractures, chondral lesions, and intra-articular loose bodies. Long-term outcomes in ankle fracture-dislocations are worse than ankle fractures without dislocation. Higher rates of posttraumatic osteoarthritis and chronic pain have also been reported. In this review, we discuss the current literature regarding the history, management, and outcomes of ankle-fracture dislocations and highlight the need for future study.
Ankle fractures are among the most common injuries encountered by musculoskeletal professionals, with more than a quarter of a million ankle fractures occurring yearly in the United States. 2 Concomitant tibiotalar dislocations have been reported to occur in as many as 21% to 36% of ankle fractures. 44,45 Purely ligamentous ankle dislocations without accompanying malleolar fracture do occur but are relatively rare. 16,18,24,26,36,48,59 Ankle fracture-dislocations may warrant special attention because of higher rates of open injury, osteochondral lesions (OCLs), intra-articular loose bodies, articular malreduction, chronic pain, posttraumatic osteoarthritis, and worse patient-reported outcomes when compared with nondislocated ankle fractures.* These factors should be considered during the evaluation of ankle fracture-dislocations, which potentially warrant advanced postreduction imaging to improve management and outcomes. 5,30,38,39,45,55 Ultimately, ankle fracture-dislocations as a distinct entity remain poorly described in the literature. The purpose of this article is to review the relevant anatomy, pathomechanics, classification, evaluation, management, and outcomes of ankle fracture-dislocations while addressing current gaps in our knowledge.
Anatomy and Pathomechanics
Relevant Anatomy
The ankle is a complex hinge joint with both bony and ligamentous contributions to joint stability. Osseous stability is provided by the ankle mortise consisting of the medial and lateral malleoli and the distal tibial plafond. The medial malleolus ends more proximally and is located anterior to the lateral malleolus, leading to an ankle axis with 15 degrees of external rotation. 21 The subcutaneous location of the medial border of the tibia creates an inherent risk for soft-tissue injury leading to open fractures. The articular surface of the tibial plafond is concave anterior to posterior corresponding to the convex talar dome. In any position of the talus, the tibial plafond covers about two-thirds of the talar articular surface. 21 The talus is wider anteriorly than posteriorly, creating more constrained motion in dorsiflexion than in plantarflexion. 36 Ligamentous stability of the ankle is provided at this distal tibiofibular joint by the syndesmotic ligaments. The syndesmosis is composed of the anterior-inferior tibiofibular ligament, the posterior tibiofibular ligament, the interosseous, and the inferior transverse ligament. The anterior talofibular and calcaneofibular ligaments as well as the medial deltoid ligament stabilize the talus within the mortise (Figure 1).
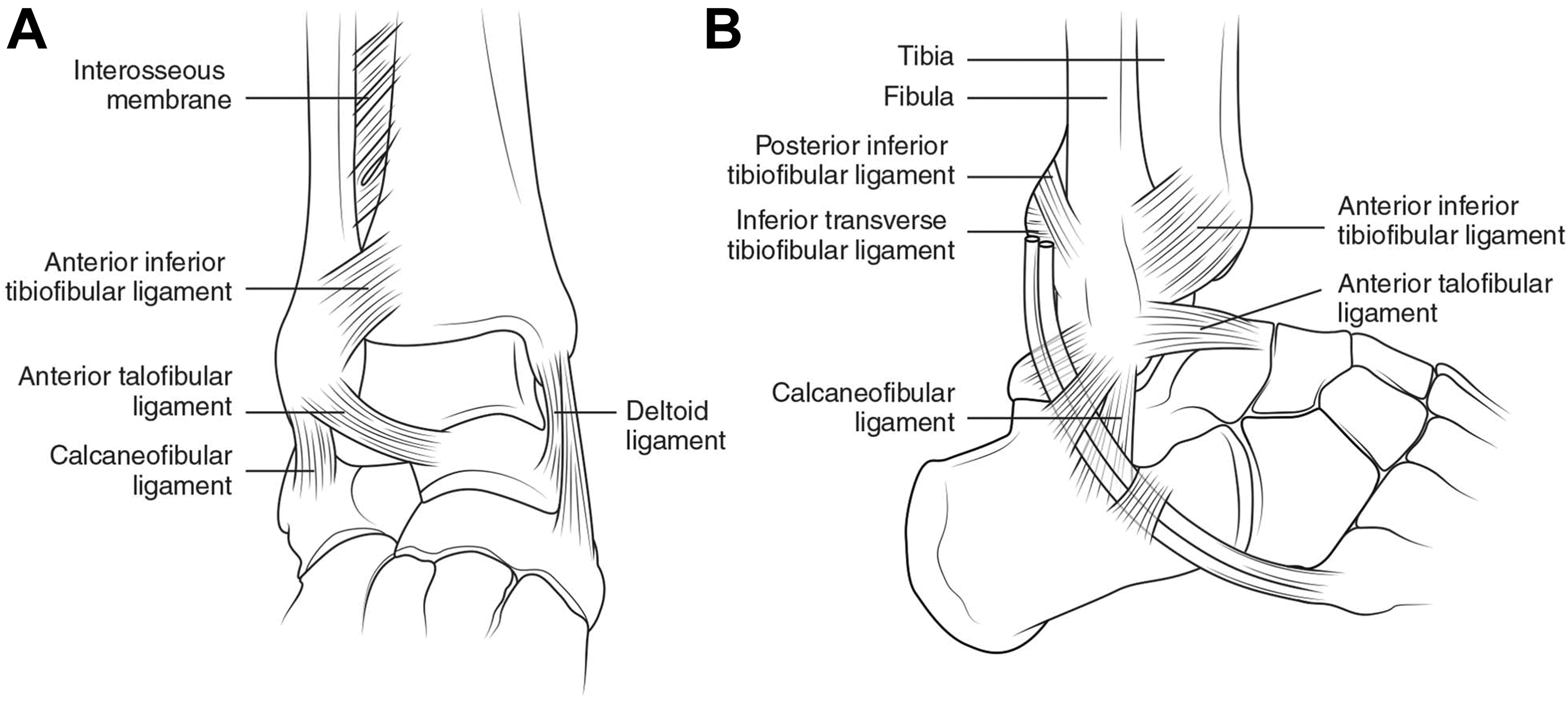
(A) Anteroposterior and (B) lateral views of the ankle joint highlighting the skeletal and ligamentous components. Reprinted with permission from Hunt KJ, Phisitkul P, Pirolo J, Amendola A. High ankle sprains and syndesmotic injuries in athletes. J Am Acad Orthop Surg. 2015;23(11):661-673.
Mechanism of Injury
Ankle fractures most often occur by rotational mechanisms with the external forces transmitted through the foot via the talus to the malleoli. The specific pattern of fracture and ligamentous injury depends on the position of the foot and the direction of the force at the time of injury. This is the basis of the Lauge-Hansen ankle fracture classification. 25 Ankle fracture-dislocations occur through similar mechanisms and patterns as nondislocated fractures, but the persistence of the deforming force after the fracture serves to disrupt the soft-tissue stabilizers resulting in talar dislocation. Depending on concomitant injury, the ligaments binding the talus to the hindfoot may still be intact. This injury process may occur via high- or low-energy mechanisms depending on the patient’s bone quality and ligamentous integrity. 36 Ankle dislocation without fracture is rare and has been reported to occur via multiple mechanisms. 16,18,24,26,36,48,59 The most common injury pattern is a posteromedial dislocation caused by maximal plantarflexion, axial load, and inversion of the ankle, often creating an open injury. 16,24 Proposed predisposing factors for ankle dislocations include malleolar hypoplasia, ligamentous laxity, and previous ligamentous injury. 26
Ankle Fracture-Dislocation Classification
Numerous ankle fracture classification systems currently exist, some of which address tibiotalar dislocations. The Lauge-Hansen classification was devised in 1948 after cadaveric research demonstrated different rotational fracture patterns that occur based on foot position and direction of force. 25 Their study demonstrated the stepwise progression of soft-tissue and osseous injury that occurs around the ankle, allowing for the prediction of mechanism and injury patterns based on plain radiographs. It is the most commonly used classification, and while it is not specific to ankle fracture-dislocations, the last stage of each mechanism of injury corresponds to an unstable ankle, which, if the force persists or is of great enough magnitude, may result in a fracture-dislocation. Although widely used, the Lauge-Hansen classification may not reliably predict all ankle fracture patterns.
The Danis classification was presented in 1949 and later modified and popularized by Weber. 9 This system classifies ankle fractures into 3 groups based on the level of lateral malleolus fracture seen on radiographs relative to the tibial plafond and is useful in the prediction of syndesmotic injury. However, this classification system fails to address medial and posterior injury patterns and is not specific to ankle fracture-dislocations. The AO classification is a detailed numerically based expansion of the Danis-Weber classification, presented as a unified code in 1996 and revised with the Orthopedic Trauma Association (OTA) in 2007. 19,33
The AO/OTA system classifies malleolar fractures under section 44 and is based on radiographic criteria detailing infrasyndesmotic (44A), transsyndesmotic (44B), and suprasyndesmotic (44C) injuries. This classification is further subclassified based on the presence of additional injuries. Tibiotalar dislocations are described under section 80B and modified by the direction of the dislocation as anterior [5a], posterior [5b], medial [5c], lateral [5d] and multi-directional [5f]. 19 Although the AO/OTA system is not specific to ankle fracture-dislocations, it currently provides the most comprehensive means of describing these injuries by encompassing principles set forth by Lauge-Hansen and Danis-Weber. 53 Limitations to this classification system include its ease of implementation and lack of focus on ligamentous injury patterns.
There is, however, an early reported classification system focused solely on tibiotalar dislocations. The Fahey and Murphy classification, described in 1965, defined tibiotalar dislocations based on the direction of talar dislocation under the tibial plafond. 15 Like AO/OTA, their classification listed anterior, posterior, medial, lateral, and superior talar dislocations, as well as combinations of these directions. However, this classification focused on tibiotalar dislocations without fracture, and as such, it is not readily applicable in the setting of more common ankle fracture-dislocations. Superior, or intrasyndesmotic, dislocations do occur with diastasis of the distal tibiofibular joint, also known as the log splitter injury. These occur from high-energy trauma and have a large rate of concomitant plafond injury. 4
Initial Management
Physical Examination and Closed Reduction
Initial management includes a thorough history, including mechanism of injury, which can provide insight into potential injury patterns. 25 Physical inspection should include neurovascular assessment and an examination of the soft tissue for signs of open wounds, blanching, swelling, and tenting. Up to one-third of ankle fracture-dislocations present as open injuries, with higher incidences reported in ankle dislocations without fracture. 22 Grossly identifiable ankle fracture-dislocations should be reduced as early as possible to decrease the risk of neurovascular and skin complications, release soft-tissue tension, reduce the time of cartilaginous impingement, and prevent delay to surgery if indicated. 40,57 In addition, as ankle fracture-dislocations can occur in the setting of high-energy trauma, full-body evaluation should be conducted when appropriate.
Prereduction radiographs may help identify obvious concomitant injuries and rule out trauma that can mimic ankle fracture-dislocation deformities including distal tibia fractures and subtalar dislocations (Figure 2A). However, gross reduction attempts should not be delayed to obtain these images if soft tissue is at risk. 40 Reduction is commonly performed with either an intra-articular block or conscious sedation in the emergency department (ED). 10,46,58 The classic reduction performed is via the Quigley maneuver, which includes knee flexion to relax the gastrocnemius-soleus complex, leg external rotation, foot adduction, and supination. 42 A modified version of this technique has proven beneficial for single-person reduction and splinting in the ED (Figure 3). 49 Following reduction, either a short leg splint or cast is applied based on fracture type, patient, surgical urgency, and surgeon preference. Closed reduction is usually successful; however, soft tissue can block reduction attempts. 14,27,50 In posterolateral dislocations, a common block to reduction is the tibialis posterior tendon, which may need to be manually reduced prior to reducing the foot. A unique irreducible fracture variant was first described by Bosworth in 1947, 7 in which the proximal fibular shaft fragment becomes incarcerated on the osseous posterolateral ridge of the distal part of the tibia.

(A) Trimalleolar ankle fracture dislocation. (B) Postreduction and splinting radiographs. (C) Computed tomography scan ordered to assess posterior malleolar fragment demonstrated retained intra-articular fragment. (D) Operative approach was tailored to address this fragment. Final ankle construct images are demonstrated.

Modified Quigley maneuver for single-person reduction and splinting of ankle fracture-dislocations. Full technique described by Skelley and Ricci. 49
Postreduction Imaging
Anteroposterior, lateral, and mortise radiographs should be obtained postreduction to determine the adequacy of reduction, for surgical decision making, and for surgical planning. Multiple views may be necessary to properly visualize the fracture pattern owing to the radio-opacity of the material used in the cast or splint (Figure 2B). Despite routine use, radiographs do not provide adequate assessment of articular injury, posterior malleolar involvement, OCL size, intra-articular loose bodies, or malreduction. 17,32,38 OCLs, which are present in up to 79% of all ankle fractures, are missed by radiographs up to 50% of the time. 20,30,31,39,55 The sensitivity and specificity of postreduction radiographs in detecting articular injury and intra-articular loose bodies in ankle fracture-dislocations have not been fully explored. There is a debate regarding the need for advanced postreduction cross-sectional imaging (computed tomography [CT] or magnetic resonance imaging [MRI]) to better identify concomitant injuries associated with ankle fracture-dislocations or as a potential result of iatrogenic cartilage injury during closed reduction (Figure 2C).
Studies suggest that advanced imaging (CT or MRI) may provide a better assessment of concomitant injuries associated with ankle fracture-dislocations and influence surgical planning. 5,11,17,28,55 A prospective analysis of 104 patients presenting with chronic ankle pain demonstrated that CT (0.81 sensitivity, 0.99 specificity), MRI (0.96 sensitivity, 0.96 specificity), and diagnostic arthroscopy were significantly better (P < .05) than standard radiography in the detection of OCLs. 55 MRI, however, can overestimate the true extent of intra-articular injury in the acute setting due to bone edema. 13 Recent studies suggest that subchondral bone appearance on CT may provide a better assessment of OCLs over MRI. 55 In addition, a prospective evaluation of 69 acute ankle fractures found that preoperative CTs allowed for the detection of posterior malleolar lesions, intra-articular loose bodies, and bony avulsions that would have otherwise been missed. 28 Operative plans have been reportedly altered in 24% to 28% of ankle fracture cases to address concomitant injuries identifiable on CT but not on radiographs. 5,28 One study found a significant difference in the operative plans modified between standard ankle fractures and ankle fracture-dislocations (20% vs 31%, respectively). 5 Despite proven utility, the use of preoperative cross-sectional imaging (CT or MRI) and arthroscopy for ankle fracture-dislocations remains surgeon dependent and a topic for future research. Similar experiences were previously reported in the setting of hip dislocations, where the morbidity associated with failure to discover concomitant injuries on plain radiographs has led to post–hip reduction CT becoming the standard of care. 1
Ultimately, clinical evaluation and postreduction imaging guide the nonoperative or operative treatment of ankle fracture-dislocations. Surgical treatment focuses on the principles of restoring native ankle anatomy but may require special considerations to address concomitant soft-tissue injuries, posterior malleolar involvement, OCLs, intra-articular loose bodies, and malreduction (Figure 2D). Specific treatment guidelines for ankle fracture-dislocations have not been outlined and are beyond the scope of this review. Nevertheless, identification and management of concomitant injuries are paramount to outcome.
Concomitant Injuries
Soft-Tissue Injury
Wound complications including dehiscence and infection are 2 of the most common complications encountered during the management of ankle fractures. 51 While patient-related factors such as diabetes, peripheral vascular disease, and smoking have all been shown to have an effect on wound complications, injury characteristics such as mechanism and timing until temporary fracture reduction also play a major role. Ankle fracture-dislocations represent an increased insult to the surrounding soft tissues, both in the force required to elicit tibiotalar diastasis and pressure from bony prominences on the soft tissue prior to reduction. This increased soft-tissue injury is represented by an increase in open wounds, with up to one-third of ankle fracture-dislocations presenting open. 41,47 Increased soft-tissue injury has been shown to result in an increased rate of postoperative complications when not properly addressed. 8,22,47 One review of surgical complications in 121 ankle fractures found that ankle fracture-dislocations (n = 41; 34%) had 3 times as many major complications, including infection, compared with standard fractures (19% vs 6.3%, P < .05). 22 In that same report, fractures-dislocations, which were not expeditiously treated, were found to have a higher major soft-tissue complication rate compared with standard ankle fractures (44% vs 5.3%). Another study found the subsequent need for irrigation and debridement for infection in 19.6% of the ankle-fracture dislocation patients, a rate significantly higher than the nondislocated cohort. 40 Some recent studies, however, have shown no significant association between postoperative infections and wound complications when comparing standard ankle fractures to ankle fracture-dislocations. 47,56 In these reports, there was a significant number of ankle fracture-dislocations that were treated initially with the application of temporary external fixators and delayed operative intervention (19% vs 49%, P = .003). 47 The use of external fixation and delayed surgery has been shown to be effective in other fractures with considerable soft-tissue injury such as pilon fractures. 40 The use of external fixation has also been recommended in ankle fractures with considerable soft-tissue injury. 44 Currently, the role of external fixation in ankle fracture-dislocation treatment is not clearly defined and likely requires individual evaluation of the soft tissue as to when to utilize it.
Intra-articular Injury
The incidence of OCLs increases with severity of the ankle fracture, with the highest rates reported in ankle fracture-dislocation series (10% up to 70%). 6,38,45,51 At medium-term follow-up, the postoperative MRI evaluation of 100 cases found OCLs of the talus and distal tibial plafond in 66.7% of all ankle fracture-dislocations versus 25% of nondislocated fractures. Patients with Ankle fracture-dislocations demonstrated a significantly higher risk of developing OCLs than patients with nondislocated fractures (odds ratio, 5.56; 95% confidence interval [CI], 1.77-17.40; P = .003). 45 In addition, the preoperative CT evaluation of 100 ankle fractures reported a 10% incidence of OCLs, with the only lesions occurring in Lauge-Hansen stage III/IV fractures. 38 Arthroscopic studies have validated preoperative MRI and CT findings, but further studies are needed to confirm the true rate of OCLs in ankle fracture-dislocations. 55 Proper identification and treatment of OCLs is crucial because of their strong association with the development of posttraumatic osteoarthritis (PTOA) and their relationship to patient-reported outcomes. 51
Ankle fracture-dislocations are also associated with higher rates of posterior malleolar involvement and intra-articular loose bodies that may require operative intervention. 23,28,54,56 One CT study of pronation–external rotation (PER) fractures found that posterior malleolar involvement was seen in 72% of dislocated PER IV fractures versus 48% in nondislocated fractures. 56 Operative plans are altered in up to 31% of ankle fracture-dislocation cases upon review of preoperative CT to address posterior malleolar involvement and intra-articular loose bodies. 23,28 Involvement of the posterior malleolus has also been demonstrated to predict worse outcomes. 54
Malreduction
Fracture comminution, poor bone quality, and technical errors have all been associated with an increased risk of malreduction. 3 Articular malreduction is known to be a major factor affecting outcomes of operatively treated ankle fractures. 3 A recent study retrospectively reviewed PER ankle fractures specifically comparing the outcomes of ankle fractures to ankle fracture-dislocations. 56 They demonstrated that postoperative articular malreduction was higher in the dislocated compared with the nondislocated group, but this was not found to be statistically significant. 56 Malreduction of the syndesmosis in the dislocated group was not found to be significant. Another study, however, evaluating supination external rotation (SER) fractures found that articular malreduction during surgery was significantly more common in the dislocated group as assessed by postoperative CT scan, 20% versus 3% (P = .005). 47 An increased rate of malreduction has been postulated as secondary to the increased complexity of articular injury seen in ankle fracture-dislocations.
Outcomes
Studies have reported variable outcomes associated with ankle fracture-dislocations. 29,44,47,56 In a recent report, ankle fracture-dislocations had a statically significant higher revision open reduction internal fixation (ORIF) rate than the nondislocated group (OR, 1.82; CI, 1.26-2.6). 41 The largest and earliest prospective study included 306 cases of ankle fracture-dislocations with a mean follow-up of 2 to 6 years, and an excellent and good outcome was reported in 82% of patients. 29 No patient-reported outcome measures were used, however, and assessment was reported by the treating surgeon. Evidence of PTOA was seen in 14% of cases at final follow-up, and female gender and accuracy of reduction were found to significantly influence clinical outcome. 29
More recent studies have shown evidence of PTOA in up to 63% of patients with ankle fracture-dislocations. 44 Ankle fracture-dislocations have been found to be significant predictors of PTOA and persistent pain without neuropathic characteristics following ORIF. 43,44 Despite these findings, long-term improvements in patient-reported outcomes have been reported up to a decade following surgery. Short- and medium-term outcomes, however, seem unfavorable toward ankle fracture-dislocations. A prospective evaluation of SER fractures revealed that at a mean follow-up of 21 months, patients with ankle fracture-dislocations had increased pain (84% vs 73%, P = .005) and decreased activities of daily living (78.1 vs 87.7, P = .014) as assessed by the Foot and Ankle Outcome Score (FAOS), when compared with nondislocated ankle fractures. 47 Similarly, a retrospective review of PER IV fractures with a mean 30-month follow-up found that fracture-dislocations were significantly associated with poorer FAOS results (symptoms, 46 vs 70, P = .002; pain, 56 vs 82, P < .001; activities of daily living, 61 vs 84, P < .002; sports, 37 vs 59, P = .036; quality of life, 25 vs 59, P < .001). 56
Prior ankle fracture studies have demonstrated significant improvement in function seen from 6 months to 1 year postsurgery. 12,37 As shown by short- and medium-term outcome studies, ankle fracture-dislocations might delay full functional recovery. 47,56 These observations could be attributed to the higher rates of concomitant injuries and articular malreduction seen in ankle fracture-dislocations.
Conclusion
Ankle fracture-dislocations are common injuries that have different outcomes than ankle fractures without dislocation. 2,44,45 Differences in outcome have been understudied, but factors including soft-tissue injury, posterior malleolar involvement, OCLs, intra-articular loose bodies, and malreductions have been postulated as possible causes for varying clinical results. † One controversy surrounding the current management of ankle fracture-dislocations includes the need for postreduction CT or MRI to assess for concomitant injury, as simple radiographs been shown to miss a large percentage of these lesions. 5,30,39,45,55 Further research is warranted into the contributing factors leading to differential outcomes seen in ankle fracture-dislocations versus fractures with dislocation.
Supplemental Material
Supplemental Material, FAO765122-ICMJE - Ankle Fracture-Dislocations: A Review
Supplemental Material, FAO765122-ICMJE for Ankle Fracture-Dislocations: A Review by Kevin A. Lawson, Alfonso E. Ayala, Matthew L. Morin, L. Daniel Latt, and Jason R. Wild in Foot & Ankle Orthopaedics
Footnotes
Notes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.