
Abstract
Background:
Autogenous cancellous bone graft and bone marrow aspirate are commonly used in lower extremity fusion procedures to enhance fusion potential, and frequently in revision situations where bone loss and osteolysis may be a feature. The tibial metaphysis is a common donor site for bone graft, with the procedure typically performed using a curette or trephine to harvest the cancellous bone. Some limitations of this technique include suboptimal harvest of the marrow portion in particular, incomplete graft harvest, and loss of graft material during the harvest process. We describe a novel vacuum-assisted bone harvesting device to acquire cancellous bone and marrow from the proximal tibia.
Methods:
This is a retrospective study of a single surgeon’s consecutive patients who underwent foot and ankle arthrodesis procedures using proximal tibia autograft obtained using a vacuum-assisted bone harvesting device. Descriptive statistics were used to summarize patient and operative characteristics and outcomes. We identified 9 patients with a mean age of 51 years, 4 of whom were female.
Results:
On average, the skin incision was slightly more than 2 cm, and 27 mL of solid graft and 16 mL of liquid phase aspirate were collected. At 6 weeks after the procedure, there was minimal to no pain at the donor site, and we did not observe any fractures or other complications.
Conclusions:
We report the use of a novel vacuum-assisted curette device to harvest bone graft from the proximal tibial metaphysis for use in foot and ankle fusions. This device has been reliable and efficient in clinical practice.
Level of Evidence:
Level IV, retrospective case series.
Introduction
Achieving solid fusion after arthrodesis procedures of the foot and ankle can be challenging, particularly in complex cases involving nonunion, revision, and/or patients with medical comorbidities that may impair healing. The use of graft is often employed in these cases, and autologous bone grafting remains the gold standard because of its osteogenic, osteoinductive, and osteoconductive properties and the lack of risk of infection and reaction associated with allogeneic products. 10
A wide variety of potential sites for harvesting bone graft have been described with associated risks and benefits, including the tibia, iliac crest, femur, and calcaneus. 7,14 For foot and ankle procedures, the proximal tibia offers several advantages, including its location on the operative limb but remote from the operative site and the large volume of bone available for harvesting. 1
In brief, traditionally bone graft has been harvested from the proximal tibia using an osteotome to create a cortical window just lateral to the tibial tubercle. 17 A curette is inserted into the metaphyseal bone, and used to scrape out the cancellous bone, which is retrieved for grafting. Although generally effective, some practical limitations to this technique include the preferential collection of the trabecular bone and not marrow, incomplete graft harvest, and the loss of material during extraction through the window. Here, we report the use of a novel vacuum-assisted bone harvesting device to obtain cancellous bone and marrow from the proximal tibia as a modification of the traditional technique. The collection system of this device captures both solid cancellous bone and liquid marrow and allows both phases to be used for grafting.
Methods
This study was approved by our institution’s Human Investigations Committee, and informed consent was obtained from all patients in the study.
Ten consecutive patients who underwent foot and/or ankle complex primary or revision arthrodesis procedures at a single tertiary academic center were identified. One patient could not be contacted to obtain informed consent and was therefore excluded. The data for the remaining 9 patients are presented in Table 1. The average age was 51 years (range 37-71). Four of the patients were female. Three patients underwent primary tibiotalocalcaneal arthodesis, one underwent primary tibiotalar arthrodesis, one underwent primary subtalar arthrodesis, and the remainder underwent various revision arthrodeses.
Demographic Data and Operative Parameters.

Abbreviations: BMA, bone marrow aspirate; EBL, estimated blood loss; Op, operative; Rev, revision; TN, talonavicular; TT, tibiotalar; TTC, tibiotalocalcaneal.
All patients had no history of knee pain, knee injury, or surgery at the proximal tibia. Incision length was recorded as well as operative time from opening of the cortex to completion of graft acquisition. The volume of cancellous graft and bone marrow were recorded separately. All patients were evaluated at 2 and 6 weeks postoperatively for donor site pain and associated complications.
Technique
All procedures were performed by the senior author. A padded thigh tourniquet was applied, and the patient was positioned with the operative extremity in the appropriate position for the required fusion procedure. The operative lower extremity was prepped in the usual fashion with the drapes placed proximal enough on the extremity that the entire knee was exposed. The bony landmarks of the knee were identified and marked.
When proceeding with graft acquisition, an approximately 2-cm incision was marked just lateral to the tibial tubercle and distal to the Gerdy tubercle at the metadiaphyseal junction (Figure 1). The skin was incised and the dissection was carried down bluntly to the periosteum. A circular entry awl (Avitus Pilot Hole Creator; Avitus Orthopaedics, Farmington, CT) was used to create a cortical window with a diameter of 10.5 mm, which was slightly smaller than the typically described cortical window. 16 A vacuum-assisted bone harvesting curette (Avitus Bone Harvester, Avitus Orthopaedics, Farmington, CT) (Figure 2) was inserted through this window in the proximal tibia and the position confirmed with fluoroscopy. The suction on the curette was activated and the curette was used to progressively scrape the cancellous bone, which was aspirated into the reservoir within the hand piece. Careful technique was required to obtain graft from only the metadiaphyseal junction and well below the joint line to minimize the risk of articular fracture. The extent of the bone harvested and the position of the curette could be confirmed with fluoroscopy throughout the procedure (Figure 3).

Incision for proximal tibia bone graft harvesting.

Vacuum-assisted curette and entry awl for allograft harvest.
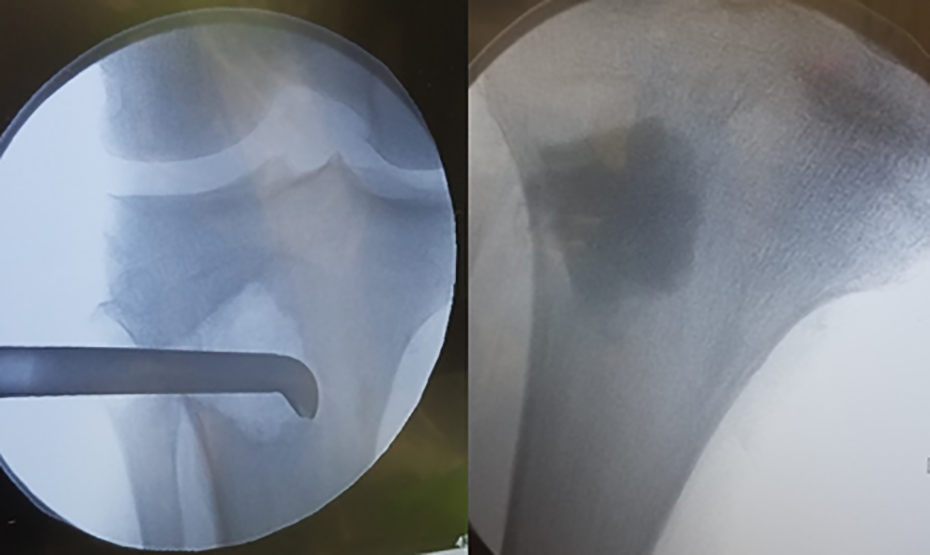
Fluoroscopic images of bone graft harvesting and cementation of the void.
Once a sufficient quantity of graft had been harvested, the curette was removed, and the void was back-filled (Figure 3). The senior author has determined injectable bone substitute to be a very effective and efficient technique to augment this harvesting device using combined calcium sulfate and calcium phosphate (Prodense, Wright Medical, Memphis, TN). When filling the void, additional attention was given to ensure fill of the cortical defect from the entry awl to reduce the potential for a stress riser.
The vacuum-assisted bone harvesting device separated the solid cancellous bone from the liquid marrow, and both were used as graft during the fusion procedure (Figure 4).

Graft material in the collection basket, and then separated into solid and liquid phase.
Results
The incision required for proximal tibial bone harvest in this series averaged slightly more than 2 centimeters, and the longest incision required was less than 3 cm (Table 1). The procedure yielded a mean of 27 mL of cancellous bone (range 20-45) and a mean of 16 mL (range 4-30) of liquid bone marrow. In all cases, graft harvest was stopped because the needs for the primary procedure were met, but more graft could have been harvested later in the case if required. The graft harvest portion of the procedure took approximately 5 minutes on average.
At the routine 2-week follow-up visit, 2 patients had moderate pain, 3 patients had mild pain, and the remainder had no or minimal pain at the bone graft donor site. At the 6-week follow-up visit, 6 patients denied any pain and 3 patients endorsed minimal pain at the donor site. Review of medical records determined that there were no patients with a proximal tibial fracture with at least 1 year of follow-up from the index procedure. No other complications were noted related to the proximal donor site in any patient.
Discussion
The utility of the proximal tibia as a donor site for bone graft harvest has been well established. 15,17 The site allows for large volumes of harvestable bone, usually between 25 and 40 mL in most series. 4,8 This is similar to the volume of cancellous bone acquired in this study, although the current device also permits acquisition of marrow and associated mesenchymal stem cells. Although the role of marrow in bone grafting for arthrodesis is not well-studied, there is evidence to suggest that connective tissue progenitor cells in marrow improve fusion. 13
The proximal tibia is within the standard draped field for foot and ankle procedures, but remote from the operative region for ankle and hindfoot fusions. This can be advantageous in cases in which fusion nails are used, or preexisting bone defects may preclude distal graft harvest. Following the completion of this presented case series, the senior author obtained graft using this technique from the distal femur, distal tibia, and calcaneus without complication. Historically, the anterior iliac crest was considered the optimal site for bone graft harvest because of a large volume of graft available, the options to take tricortical structural graft, and the well-documented success of iliac crest graft in obtaining fusion. 6 However, there is also well-documented morbidity involved in iliac crest harvest, which is at least partly responsible for the interest in other donor sites. 5 Ultimately, the choice of bone graft donor site is case specific.
Although proximal tibial fracture has been reported in the literature, this is a rare complication, occurring in less than 1% of patients. 11,12,15 In 2 of these cases, the metaphyseal void was not filled after the harvest procedure. 11,12 The necessity of backfilling the harvest site has not been conclusively demonstrated in the literature and has been most thoroughly studied for iliac crest harvest for spine surgery. 3 However, given the reported proximal tibia fractures in cases without backfill, the senior author routinely backfills graft harvest sites. Numerous options have been described for filling harvest site voids, including allograft and various cement formulations. 2,9 To our knowledge, none of these materials have demonstrated superiority. The senior author’s preference is to use cement to provide immediate structural support. Other complications of bone graft harvest from the proximal tibia are also rare and include joint perforation, hematoma, and infection, none of which were observed in this study. 14 The risk of joint perforation can be minimized by using fluoroscopy to confirm the position of the curette relative to the joint line.
The occurrence of postoperative pain from proximal tibia graft harvest is similar to previous published reports, in which most patients had mild or minimal pain immediately postoperatively and at last follow-up. 17 This contrasts with studies of iliac crest harvest, where postoperative pain at the graft harvest site is more severe than the arthrodesis site more than a quarter of the time. 5
We were unable to obtain a direct price from the manufacturer due to their confidential pricing model, and we were also unable to obtain a dollar cost that our institution pays. We do recognize the importance of cost-effectiveness in orthopedics, and further study of the cost-effectiveness of single-use devices and instrumentation generally is warranted. The lack of clear pricing information makes accurately assessing the cost-benefit ratio of this device compared to traditional techniques challenging, and is a limitation of this report.
In conclusion, we found that use of this vacuum-assisted bone harvesting curette allowed for rapid and reliable bone graft harvest from the proximal tibia through a 2-cm incision. Backfilling with synthetic bone substitute provided immediate structural integrity, which may be associated with less pain. In addition, the acquisition of autologous marrow for insertion into the fusion site may confer increased success by enhancing the osteoinductive and osteogenic load. Further work could examine the use of this device in other donor sites and compare it more directly to standard curettage techniques.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_2473011420981901 - Novel Vacuum-Assisted Method for Harvesting Autologous Cancellous Bone Graft and Bone Marrow From the Proximal Tibial Metaphysis
Supplemental Material, sj-pdf-1-fao-10.1177_2473011420981901 for Novel Vacuum-Assisted Method for Harvesting Autologous Cancellous Bone Graft and Bone Marrow From the Proximal Tibial Metaphysis by Adam M. Lukasiewicz, Paul S. Bagi, Kristin E. Yu, Vineet Tyagi and Raymond J. Walls in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was obtained from Yale University Institutional Review Board (#2000025458).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.