
Abstract
Background:
Persons with amputation and residual limb wounds would benefit from the ability to continue wearing a prosthesis while healing. Sockets with vacuum-assisted suspension may reduce intra-socket motion and be less disruptive to wound healing. The purpose of this case series was to measure residual limb wound size over time in persons with transtibial amputation while using prostheses with vacuum-assisted suspension.
Case description and methods:
Six subjects with residual limb wounds were fit with vacuum-assisted suspension sockets. Wound surface area was calculated using ImageJ software at the time of fit and each subsequent visit until closure.
Findings and outcome:
Average wound surface area at initial measurement was 2.17 ± 0.65 cm2. All subjects were instructed to continue their normal activity level while wounds healed, with a mean of 177.6 ± 113 days to wound closure.
Conclusion:
Results suggest that well-fitting sockets with vacuum-assisted suspension in compliant individuals did not preclude wound healing. Further research is required to substantiate these case-based observations.
Clinical relevance
Residual limb wounds are typically treated by suspension of prosthetic use until healing occurs, increasing the risk of long-term prosthesis nonuse. Our results suggest that vacuum-assisted suspension sockets may be used while healing occurs.
Background
Each year, over half of all amputations in the United States are caused by diabetes mellitus (DM) and subsequent complications. 1 Individuals with diabetic amputation are at greater risk of recurrent skin ulceration and pressure damage. A wound on the residuum can be caused by a high-pressure area in the socket, inappropriate use of the prosthesis, overactivity with the prosthesis, or an ill-fitting prosthetic socket. A properly fitting socket is necessary to reduce the pressures and shear forces transferred from the socket to the skin. 2 If left untreated, residual limb wounds can lead to reamputation at a higher level, as occurs in 19% of transtibial amputations. 3
If an individual with amputation develops a wound while wearing a prosthesis, the most common course of treatment is to discontinue use of the device until the area is completely healed. 4 The most significant consequences of this course of treatment are limitations in activities of daily living. For individuals who develop wounds prior to prosthetic fitting, there are long-term functional consequences: it has been reported that the greatest predictor of failure to use a prosthesis following transtibial amputation is the presence of a wound. 5 Clearly, a prosthetic socket that would allow an individual with amputation to continue use of the prosthesis while allowing a residual limb wound to heal would be of great potential benefit.
Over the past decade, vacuum-assisted suspension (VAS) has been introduced into clinical practice. This technology uses a vacuum pump to remove air between a gel liner and the inner wall of a prosthetic socket. It has been theorized that application of negative pressure to the sealed space leads to high static frictional forces that prevent separation of the liner from the socket wall. 6 Studies have suggested that VAS may reduce relative motion between the prosthetic socket and residual limb,7–9 prevent residual limb volume loss,8,10,11 and reduce skin problems in persons with transtibial amputation.12–14 Researchers have hypothesized that VAS maintains residual limb volume by minimizing fluid flow out of the limb, which may improve circulation within the limb and keep the residual limb soft tissues better hydrated.6,15
VAS appears to have the potential to produce conditions inside the prosthetic socket that are theoretically less disruptive to wound healing. However, only a few studies have explored this possibility. Traballesi et al. 13 published a case report of a 60-year-old male with a transtibial amputation due to type II DM who was able to participate in gait training and ambulate for 4 h a day in a VAS system while a large wound on his residuum healed. Brunelli et al. 12 compared 7 persons with transtibial amputation and residual limb wounds managed with VAS prostheses to 17 persons with transtibial amputation without wounds managed with patella tendon bearing (PTB) sockets. The authors reported that all the subject’s wounds were closed after 9 months. In a follow-up study, Kannenberg et al. 14 reported that wound healing success did not differ between groups with transtibial amputation randomized to wearing either the VAS or PTB suction prostheses. 14
The above-mentioned studies calculated wound size using linear measurements of the longest and shortest axes of the wound. It has been suggested that there are inaccuracies in this method and that it is especially inappropriate for irregularly shaped wounds. 16 A more accurate method would be to measure the total wound surface area. Hence, the purpose of this case series was to measure changes in residual limb wound surface area over time in persons with transtibial amputation while using prostheses with VAS.
Case description and methods
Subjects (n = 6) were recruited from among patients with transtibial amputation at Dayton Artificial Limb Clinic (Dayton, OH) from January 2011 to April 2012.Subjects were monitored if they had a unilateral transtibial amputation, had a wound present on their residual limb, and were provided a prosthetic socket with VAS while the wound was still open. Written informed consent to track and report wound healing was obtained from each subject prior to monitoring, and each subject was treated under the direct supervision of a licensed physiatrist.
Subjects who developed a wound while wearing a previous prosthesis were instructed by their physician to wear the new VAS prosthesis as much as possible given any pain they may experience and not to limit their activities. Those subjects who developed wounds during their initial prosthetic fitting process continued with the fitting process and physical therapy regimen as prescribed by their physician. All wounds were dressed according to the physician’s orders, and instructions varied across physicians as well as subjects depending on a number of factors, including wound severity, presence of drainage or blood, patient ability, and resources afforded by the insurance provider. For all subjects, socket adjustments were made over time as necessary to maintain socket fit. Wound surface area was initially assessed at the time of first onset and at each follow-up appointment until wound closure occurred.
Table 1 contains a description of subject diagnoses and pertinent characteristics such as age, gender, weight, height, time since amputation, cause of amputation, and any other pertinent comorbidities. All subjects were provided with custom-made total surface bearing sockets with SealMate™ Liners and Elevated Vacuum Locking System® for suspension (all from Prosthetic Design, Inc., Clayton, OH, USA). As shown in Table 1, subjects used different vacuum pumps and prosthetic feet as well as varying in the average vacuum level maintained inside the VAS socket. Maximum obtainable vacuum level in a VAS socket is dependent on the model of vacuum pump used. The maximum level of vacuum for the pumps used in this study varied from 15 to 25 inHg. The vacuum level for each subject was chosen by finding the highest level at which the subject reported acceptable socket comfort and function after ambulating for 2 min on level ground during the dynamic fitting process. All subjects were started out at the maximum vacuum level allowed by the pump they were using. If discomfort was reported, the vacuum level was reduced until an acceptable level of socket comfort was maintained during the 2-min ambulation period. Theoretically, increased vacuum levels result in an increase in suspension force between the liner and socket wall and hence less relative motion between the residual limb and prosthesis. 6
Subject characteristics.
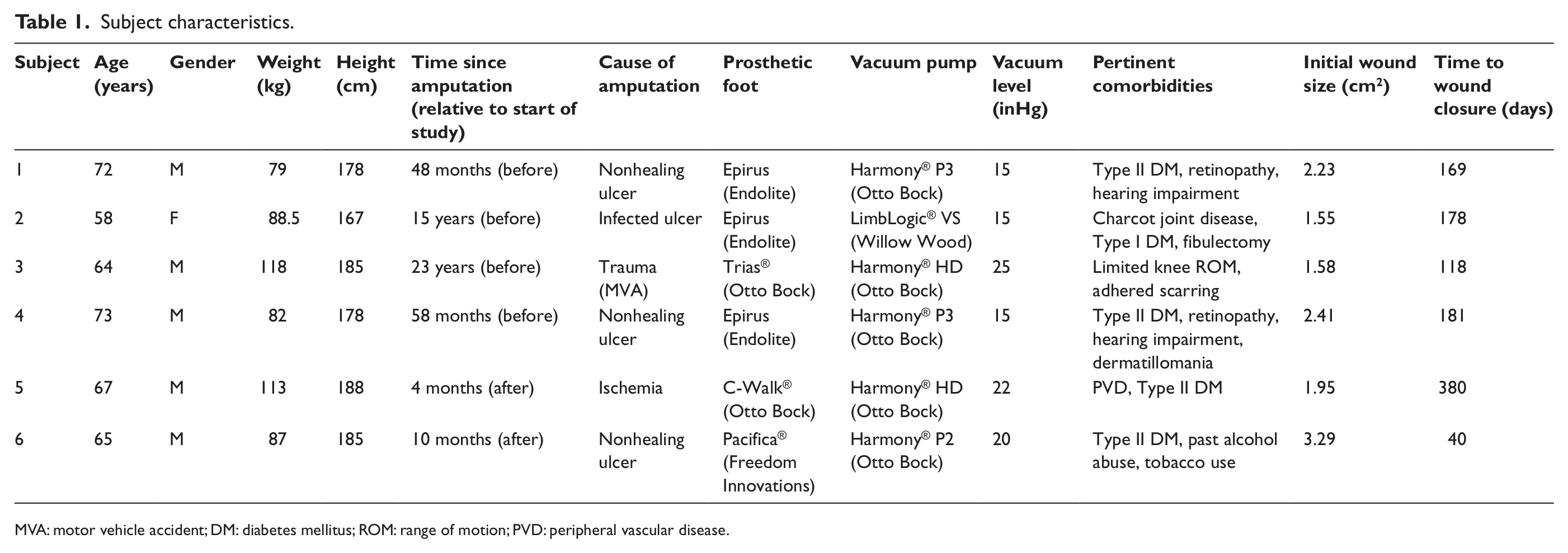
MVA: motor vehicle accident; DM: diabetes mellitus; ROM: range of motion; PVD: peripheral vascular disease.
Changes in wound surface area were documented using digital photographs of the wound (minimum resolution of 5 megapixels) taken at each prosthetic follow-up appointment, beginning the day that the VAS system was delivered and continuing every 1–2 weeks until wound closure occurred. The camera was positioned perpendicular to the wound, and a ruler held just above or below the wound for scaling. The ruler was held in contact with the residual limb to minimize error related to depth, consistent with methods previously reported.17,18
Two raters (authors D.K. and J.M.S.) independently measured wound surface area for all photographs using the ImageJ software developed by the National Institutes of Health. 19 Using measurements from both raters, the mean wound surface area was calculated and recorded for each photograph for each subject. Previous studies have reported good intra- and interrater reliability for this technique.17,20 To check the interrater reliability of measurements in this study, a US minted quarter-dollar coin with known surface area was measured by both raters from a photograph of the object. The variability in measurement of surface area between raters was ±0.2%.
Findings and outcomes
Six subjects with unilateral transtibial amputation and residual limb wounds were followed as part of this case series. Average wound surface area at initial measurement was 2.17 ± 0.65 cm2. While using the VAS system, wound closure was achieved for all subjects although time to healing varied (average time to healing was 177 ± 113 days, Figure 1). Images of the subjects’ wounds at initial fitting with VAS and final follow-up are shown in Figure 2.
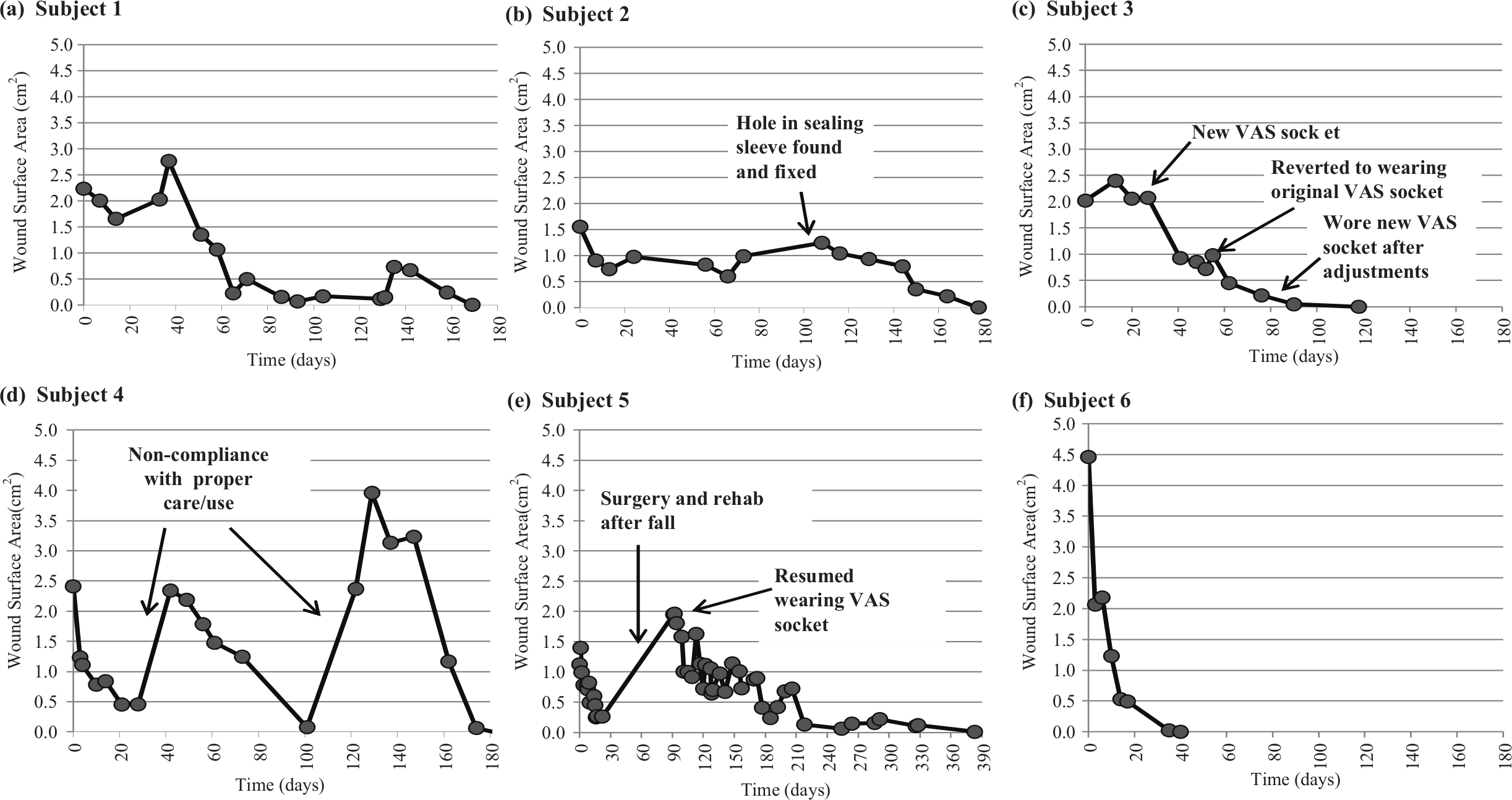
Changes in mean wound surface area during VAS use for each subject: (a) Subject 1, (b) Subject 2, (c) Subject 3, (d) Subject 4, (e) Subject 5, and (f) Subject 6.
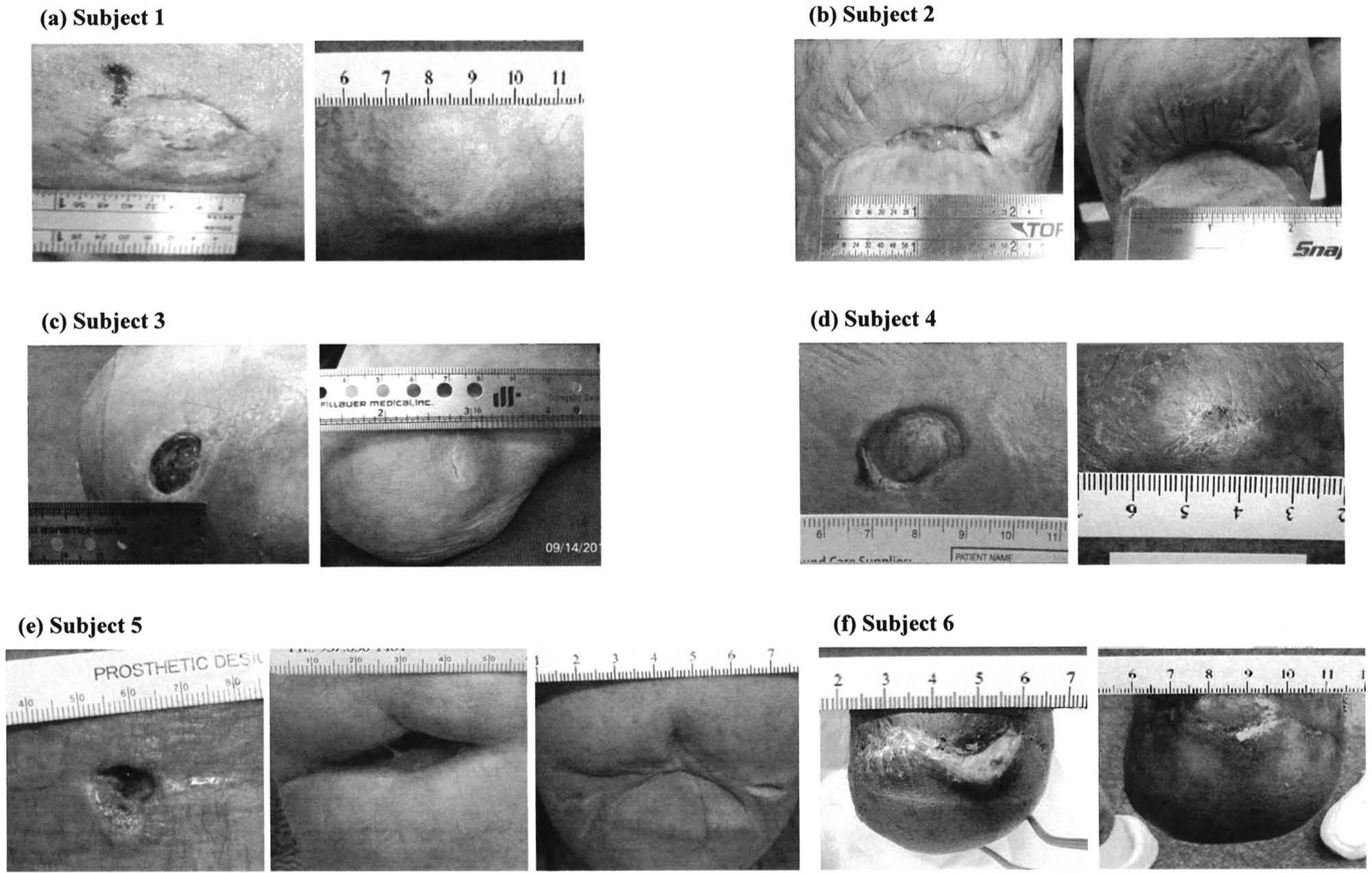
For each subject, left images show wound size at first appointment and right images show wound size at final follow-up appointment. For Subject 5, the central image shows wound size following removal of a hematoma and subsequent incision dehiscence at 3 months and the right image after 13 months of continuous VAS use: (a) Subject 1, (b) Subject 2, (c) Subject 3, (d) Subject 4, (e) Subject 5, and (f) Subject 6.
Discussion
The purpose of this case series was to measure changes in residual limb wound surface area over time in persons with transtibial amputation who were using prostheses with VAS. All subjects obtained wound closure while using the VAS prostheses, consistent with the case study described by Traballesi et al. 13 that suggested that VAS allowed for prosthetic fitting and walking despite the presence of an open residual limb wound with large surface area. It is possible that the benefit of using a prosthesis during wound healing is the ability to continue ambulating rather than the particular socket design used. Beyond permitting continuation of activities of daily living, ambulation may help promote healing. Significant reduction in wound size has been previously reported, when using prostheses that did not incorporate VAS. 4
Variability in rate of wound healing among our subjects was not surprising given the heterogeneity in health conditions, wound severity, and compliance in terms of wound care and prosthesis use (see online supplemental information for in-depth description of subject history and clinical management). Unfortunately, we cannot confirm the contribution of these factors to rate of healing as this was not the aim of this study.
Many other factors can affect wound healing. Loss of negative pressure in the socket system and subsequent increase in wound size that occurred during the follow-up of Subject 2 suggest that active maintenance of vacuum within the socket facilitates wound healing. In the case of Subject 2, once the sealed environment was restored, wound size decreased until the time of closure, with no other changes made to the prosthesis. For Subject 1, intermittent progress in wound healing appeared to be due to noncompliance with the wound dressing protocol, as well as improper use of the prosthesis. Additionally, Salawu et al. 4 reported that age, time since amputation, and duration of wound prior to treatment might all contribute to lack of wound healing with prosthesis use. However, they did not use VAS in their study but rather used various sockets combined with adjustments to relieve direct pressure and shear forces.
Subjects 2, 3, and 5 developed wounds on their residual limbs while wearing a VAS socket, suggesting that a VAS prosthesis does not prevent wounds and that an ill-fitting VAS socket can contribute to wound development just like any other ill-fitting socket. However, as demonstrated by these subjects, if a wound develops while in a VAS socket, changes to the socket to improve fit can rectify the problem without the need to take the individual out of the prosthesis. Salawu et al. 4 reported similar success with continued wear of other socket designs adapted to relieve pressure over residual limb wounds.
When a residual limb wound occurs, the most common course of treatment is to discontinue use of the device until the area is completely healed. However, our case study and the work of Salawu et al. 4 suggest that it may be possible for wound healing to occur without discontinuing use of the prosthesis if socket fit is closely monitored and maintained. Using VAS may help increase the odds of maintaining a good fit, one element of which is the reduction of relative motion between the residual limb and socket.7–9 Although it is generally appreciated that inappropriate mechanical stress (especially shear) can damage soft tissue, it seems that some mechanical stress may facilitate wound healing. It has been proposed that deformation of tissues results in deformation of cells, followed by stimulation of growth factor pathways that leads to increased mitosis and production of new tissue. 21 Tensile stresses applied to the skin stimulate cellular proliferation while compressive forces lead to resorption of the underlying tissues. 22 It would seem that while VAS may reduce relative motion between the socket and residual limb, it is unlikely to entirely remove motion of the bone within the soft tissue that occurs with loading, hence an element of mechanical deformation of the soft tissues remains.9,23 Using videofluoroscopy and a controlled loading protocol, 24 Wilken 9 reported that use of VAS decreased limb–socket displacement by approximately half compared to the same socket without vacuum applied. It is also possible that if there is adhesion of the skin to the inner surface of the liner, vacuum applied to the outer surface of the liner and pulling the liner toward the socket wall may in turn apply a tensile force to the skin. These are all theories in need of further investigation.
In general, documenting wound surface area and prosthetic management specific to each subject provided useful insight regarding the use of VAS during wound healing. The fact that subjects in this study were drawn from a single private practice limited the number of individuals who met our inclusion criteria. The relatively simple protocol described in this article could be used as part of a multisite clinical study to increase sample size and improve the level of evidence for management of residual limb wounds with VAS sockets. Unfortunately, the wound size measurement used in this study, while more accurate than some, 16 does not account for the depth or severity of the wound, making it difficult to determine factors influencing rate of healing.
This report provides observations from six cases collected as part of routine clinical care at a private prosthetic facility. Without a comparison group, it is not possible to infer a causal relationship between our observations of wound healing and the prosthetic intervention. Without a control group, there is no way of knowing whether healing would have occurred regardless of prosthesis use. There are many other confounding factors (actual prosthesis use, additional therapies the subjects may have been receiving, etc.) that were not controlled and may have influenced wound healing.
Additional research is needed to improve understanding of fluid exchange within the residual limb during ambulation, the mechanics of wound healing while using a prosthetic socket and VAS in particular, the rate of healing achieved with different socket designs, and the cost–benefit analysis of wound care without the prosthesis compared to the cost of fitting and monitoring the patient with a socket during wound healing.
Conclusion
We observed closure of residual limb wounds in six subjects with unilateral transtibial amputation while wearing VAS sockets. The results of this case series contribute to the growing body of evidence that suggests that VAS prostheses may be used while managing residual limb wounds in persons with transtibial amputation. The results suggest that a well-fitting socket with VAS in compliant individuals does not preclude wound healing and that wound closure is possible without limiting or halting activities.
Footnotes
Acknowledgements
The authors acknowledge Brad Poziembo, CP/LP and Luci Busch, CP/LP for assisting with data collection and Tracy Slemker, CPO/LPO, FAAOP of Prosthetic Design, Inc. and Dayton Artificial Limb Clinic for supporting this study. The authors would also like to thank the subjects who participated in this case series.
Conflict of interest
Robert Hoskins and Erin Sutton were employees of Prosthetic Design, Inc. while this research was being performed. However, the report focuses on vacuum-assisted suspension technology as a means to manage residual limb wounds in general and not the effects of Prosthetic Design, Inc. components, so the authors feel that they did not introduce significant bias. Prosthetic Design, Inc. had no direct role in the collection, analysis and interpretation of data. The authors accept full responsibility for the integrity of the work performed.
Funding
The contribution of Dr Fatone to this work was supported by the National Institute on Disability and Rehabilitation Research (NIDRR) of the US Department of Education grant H133E080009.