
Abstract
Cerebrospinal fluid (CSF) leaks can occur when there is communication between the intracranial cavities and the external environment. They are a common and serious complication of numerous procedures in otolaryngology, and if not treated, persistent leaks can increase a patient’s risk of developing life-threatening complications such as meningitis. As it is not uncommon for patients to exhibit increased secretions postoperatively, distinguishing normal secretions from those containing CSF can be difficult. Currently, there are no proven, available tests that allow a medical provider concerned about a CSF leak to inexpensively, rapidly, and noninvasively rule out the presence of a leak. The gold standard laboratory-based test requires that a sample be sent to a tertiary site for analysis, where days to weeks may pass before results return. To address this, our group recently developed a semiquantitative, barcode-style lateral-flow immunoassay (LFA) for the quantification of the beta-trace protein, which has been reported to be an indicator of the presence of CSF leaks. In the work presented here, we created a rapid diagnostic test kit composed of our LFA, a collection swab, dilution buffers, disposable pipettes, and instructions. Validation studies demonstrated excellent predictive capabilities of this kit in distinguishing between clinical specimens containing CSF and those that did not. Our diagnostic kit for CSF leak detection can be operated by an untrained user, does not require any external equipment, and can be performed in approximately 20 min, making it well suited for use at the point of care. This kit has the potential to transform patient outcomes.
Keywords
Introduction
Cerebrospinal fluid (CSF) leaks occur when there is a defect in the dura mater that results in communication between the intracranial cavities and the external environment. CSF leaks are a common complication of numerous procedures in otolaryngology, where the risk in endoscopic skull base surgery has been estimated at 13.8%, endoscopic sinus surgery at 0.17%, and cochlear implantation at 0.4%.1–3 In fact, almost all procedures involving the sinuses, skull base, or ear carry some risk of a leak. Individuals who have not undergone surgical procedures are also at risk for CSF leaks. Approximately 80% of all leaks occur as a result of nonsurgical traumatic injuries, such as facial and skull bone fractures. 4 Although rare, some individuals even present with spontaneous CSF leaks such as CSF otorrhea from an encephalocele. 5 Persistent CSF leaks can result in chronic headaches and discomfort as well as increase a patient’s risk of developing life-threatening complications such as bacterial meningitis and brain abscess.6,7 Therefore, early diagnosis and subsequent repair of CSF leaks is imperative to prevent these complications.
In the acute setting, assessment is performed using imaging modalities such as magnetic resonance imaging or computed tomography. 8 If there is high enough clinical suspicion, such as obvious facial or skeletal deformities, or copious clear rhinorrhea or otorrhea, patients may be taken directly to the operating room for management. This involves first identifying the site of the leak and then using either native tissue or biocompatible materials to patch the affected site.
In an outpatient or postoperative hospital setting, diagnosing a CSF leak can be much more difficult. It is not uncommon for patients to exhibit heighted secretions after surgery, and thus, distinguishing normal secretions from those containing CSF can be difficult. Physicians could turn toward the imaging techniques used in the acute hospital settings; however, the cost is often difficult to justify for patients who otherwise seem healthy. Laboratory-based techniques for the detection of CSF may also be implemented. The laboratory gold standard technique involves the identification of the CSF-specific protein beta-2 transferrin using immunofixation electrophoresis.9–13 Although proven to have excellent sensitivity and specificity in detecting CSF leaks, electrophoretic assays tend to be time-consuming, expensive, and labor intensive. In addition, these assays may not be readily available in some clinical laboratories, and thus, a sample must be sent to a tertiary site for analysis, where days to weeks may pass before results return. 14
As an alternative, researchers have investigated beta-trace protein (βTP), also known as lipocalin-type prostaglandin D2-synthase, as an indicator of CSF leaks. βTP is a ubiquitous protein present at various concentrations throughout the body but is notably one to two orders of magnitude more concentrated in CSF than in serum and nasal secretions. 15 As a result, numerous studies have demonstrated that nasal secretions with βTP concentrations (measured using laser nephelometry) above a certain threshold are highly likely to be contaminated with CSF.16–20 A recent study by Bernasconi et al. 21 demonstrated that concentrations of βTP in nasal secretions ≥1.3 mg/L indicate the presence of a CSF leak, whereas concentrations of βTP <0.7 mg/L indicate the absence of a leak. βTP concentrations between 0.7 and 1.29 mg/L (denoted the “gray zone”) require further analysis and comparison with the patient’s βTP serum level to confirm the presence or absence of a CSF leak. Overall, this approach showed a sensitivity and specificity of 98.3% and 96%, respectively. 21 Although the nephelometric assay is more rapid than electrophoresis, it still requires centralized laboratory equipment that may not be available in every clinical setting. In fact, there are still no proven, widely available diagnostic techniques that allow physicians to rule out the presence of a CSF leak in a rapid, affordable, and noninvasive manner.
To address this, our lab has previously developed a semiquantitative, barcode-style lateral-flow immunoassay (LFA) for the detection of βTP. 22 Using this LFA, we demonstrated the ability to identify serum samples spiked with CSF from those that were not. Although these results were promising, we had yet to validate our LFA using samples from patients with or without CSF leaks. In addition, before running these assays, a sample dilution step was performed using precision laboratory pipettes, which may not be readily available in all clinical settings. In the work presented here, we have developed a rapid diagnostic test kit containing our semiquantitative LFA for detecting βTP, a collection swab, diluent buffers, and disposable quantitative transfer pipettes. The kit we have developed (described herein) is simple to use, does not require prior user training, and does not need additional supplies (such as laboratory pipettes), which make it facile and suitable for use at the point of care. We validated our kit by testing a variety of different samples collected from regions surrounding the brain and demonstrated its ability to serve as a rapid, low-cost screening tool for the detection of CSF leaks. To our knowledge, this is the first rapid diagnostic test kit developed for the detection of CSF leaks.
Materials and Methods
Formation of Anti-βTP Antibody-Conjugated Gold Nanoprobes
All reagents and materials were purchased from Sigma Aldrich (St. Louis, MO) unless otherwise noted. Gold nanoprobes (GNPs) for the detection of βTP were prepared according to our previously reported protocol. 22 Briefly, anti-βTP GNPs were formed by first mixing 35 µL of a 0.1 M sodium borate solution (pH 9) with a 1 mL suspension of 40 nm citrate-capped gold nanoparticles (Nanocomposix, San Diego, CA). Subsequently, 8 µg of anti-βTP detection antibodies were added and incubated for 30 min at room temperature to allow the formation of dative bonds between the antibodies and the surface of the gold nanoparticles. The surface of the gold nanoparticles was then passivated to prevent the nonspecific binding of other proteins by adding 100 µL of a 10% w/v bovine serum albumin (BSA) solution and allowing the mixture to react for 10 min. Lastly, free antibodies were removed from the suspension by 3 centrifugation steps at 9000 rcf for 6 min, followed by a final resuspension in 100 µL of a 0.1 M sodium borate buffer (pH 9).
Preparation of Barcode-Style LFA Test Strips
LFA test strips were constructed by overlapping and securing different functional paper pads on an adhesive backing. Each LFA test strip included a sample pad, conjugate pad, nitrocellulose membrane, and absorbent pad. Each sample pad was made by dehydrating 12 µL of 1% w/v BSA in 0.1 M Tris buffer (pH 9) onto a 3 × 10 mm fiber glass paper pad. Each conjugate pad was made by dehydrating a 12 µL solution containing 2.5 µL GNPs and 1% w/v BSA overall onto a 3 × 10 mm fiber glass paper pad. Both the sample pads and conjugate pads were dehydrated under very low pressure using a Labconco FreeZone 4.5 lyophilizer (Fisher Scientific, Hampton, NH) for 2 h.
The nitrocellulose membrane was prepared by immobilizing antibodies at three different test line locations (T1, T2, and T3) and a control line location. The concentrations of the anti-βTP detection antibodies immobilized at T1, T2, and T3, were 2, 0.5, and 0.35 mg/mL, respectively. The control line was composed of an anti-mouse immunoglobulin G (IgG) secondary antibody immobilized at 0.5 mg/mL. The antibody immobilization process was performed by printing solutions of antibodies in 25% w/v sucrose onto a nitrocellulose membrane using an Automated Lateral Flow Reagent Dispenser (Claremont BioSolutions, Upland, CA) and a Fusion 200 syringe pump (Chemyx, Stafford, TX) at a flow rate of 250 µL/min. The printed membrane was then left in a vacuum-sealed desiccant chamber overnight. After antibody immobilization, the nitrocellulose membrane was blocked by immersing it in a solution of 1% w/v BSA in 0.1 M Tris buffer for 1 h followed by dehydration overnight at low pressure with a lyophilizer.
To assemble the LFA test strip, the nitrocellulose membrane was first mounted onto the adhesive backing. The absorbent pad was adhered onto the adhesive backing just downstream of the control line, where it overlapped the nitrocellulose membrane by 2 mm. Next, the conjugate pad was adhered onto the backing just upstream of the test lines, where it overlapped the nitrocellulose membrane by 1 mm. Lastly, the sample pad was adhered to the region of adhesive backing upstream of the conjugate pad while also overlapping the conjugate pad by 2 mm.
Preparation of Rapid Diagnostic Kit for CSF Leak Detection
A rapid diagnostic test kit was assembled containing one barcode-style LFA test strip, one Flexible Minitip Flocked Swab (Becton, Dickinson and Company, Franklin Heights, NJ), two disposable Samco Exact Volume Transfer pipettes (Thermo Scientific, Waltham, MA) with a capacity of 100 µL, diluent buffers, and user instructions. Tube A contained 2320 µL of phosphate-buffered saline (PBS). Tube B contained 450 µL of PBS mixed with 450 µL of running buffer (0.4% BSA, 0.6% Tween 20, 0.2% polyethylene glycol, 0.1M Tris buffer pH 9). Tube C was supplied empty. All components were placed in a resealable bag with desiccant for storage.
Operation and Validation of Rapid Diagnostic Test Kit for CSF Leak Detection
The schematic representation of the user steps for our developed diagnostic test kit is shown in Figure 1 . To determine whether a sample fluid contained CSF, the fluid was first absorbed into the collection swab. The swab was then inserted into the buffer in tube A and twirled around the edge of the tube for 10 s at two rotations per second to release the sample from the swab into the buffer. Tube A was then inverted five times to ensure the released sample was well mixed. Next, 100 µL of the liquid in tube A was transferred to tube B using one of the provided disposable transfer pipettes. Tube B was then inverted five times to ensure complete mixing. The release of the sample from the swab into tube A and the subsequent transfer into tube B resulted in an overall 300-fold dilution of the original sample. Lastly, 100 µL of the solution in tube B was transferred into tube C, where the barcode-style LFA test strip was also inserted. After 20 min, the results were interpreted where the formation of zero and one, two, or three visible test lines indicated a diagnosis of negative, gray zone, or positive, respectively. Photographs of the test strips were taken by a Nikon D3400 digital camera (Nikon, Tokyo, Japan) in a controlled lighting environment.
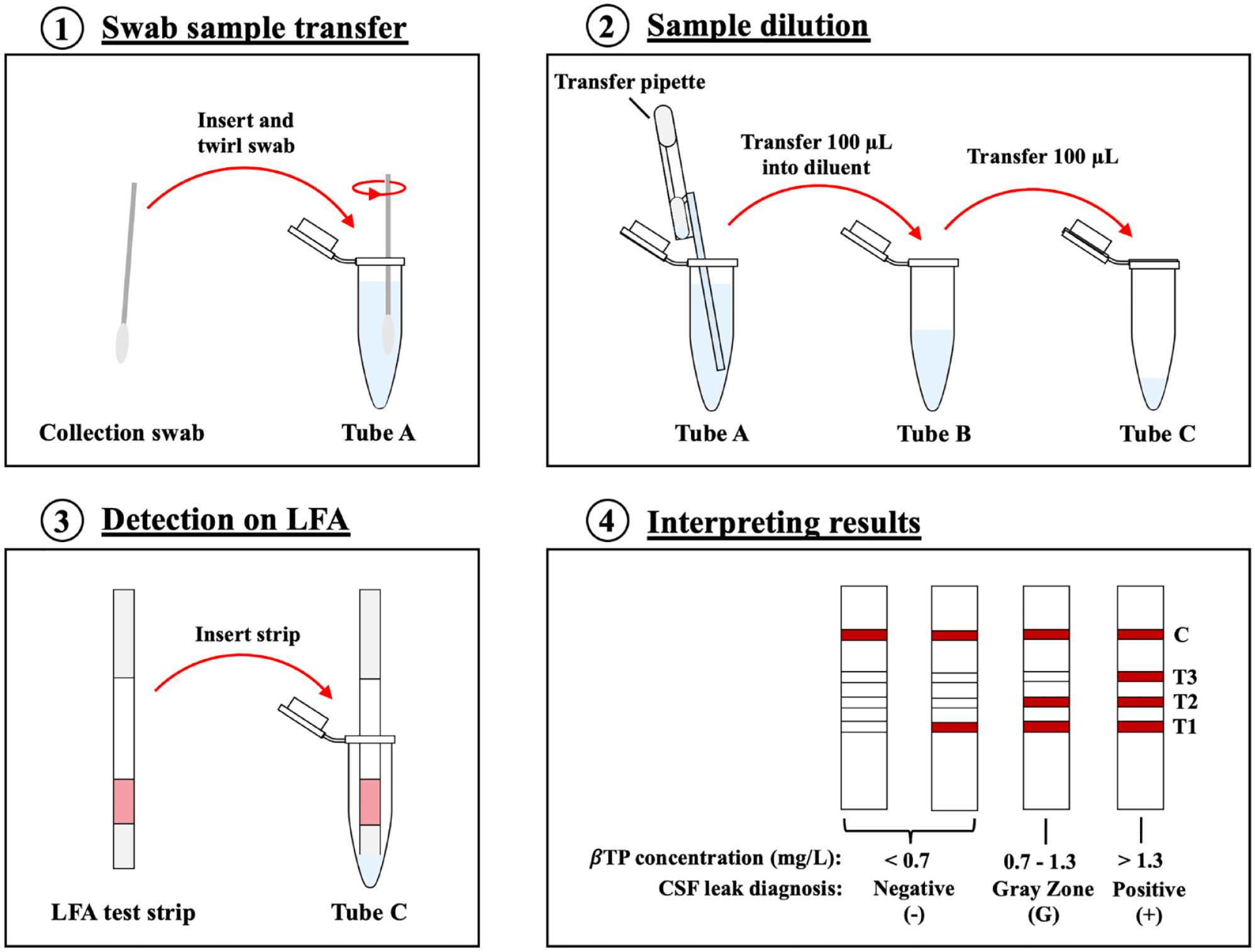
Schematic representation of the procedure for operating our rapid diagnostic test kit for the detection of cerebrospinal fluid leaks. (
We first evaluated the ability of our diagnostic test kit to detect for βTP by testing samples containing purified, recombinant βTP in PBS. Then we evaluated a variety of different patient samples collected at the Ronald Reagan University of California Los Angeles Medical Center that were either negative or positive for the presence of CSF. These included fluid collected from skull base sites during endoscopic transnasal transsphenoidal surgeries, superior semicircular canal dehiscence repair surgeries, and brain tumor resection surgeries. Rhinorrhea and otorrhea specimens from healthy volunteers and patients with suspected CSF leaks were also included (University of California Los Angeles Institutional Review Board approval 17-001065).
Results
Barcode-Style LFA Principle and Interpretation
Similar to our previous work, the barcode-style LFA used in our kit was designed such that the presence of the target biomarker, βTP, would produce one to three visible test lines, because the βTP would become sandwiched between the GNPs and the test line antibodies. Each test line has a cutoff value, which is the minimum concentration of βTP required for that line to become visible to the user. In designing a barcode-style LFA, the cutoff value for each line could be adjusted by varying the concentrations of the immobilized antibodies. Regardless of the presence of βTP, the anti-mouse IgG secondary antibodies immobilized at the control line would bind to the primary antibodies on the GNPs, capturing them. This would result in the formation of a visible red control line to indicate successful flow of the sample solution through the LFA test strip and thus valid test results.
The cutoff values for each test line of our barcode-style LFA were adjusted to correspond with the threshold values proposed by Bernasconi et al. 21 βTP concentrations <0.7 mg/L would result in the appearance of zero or one test line and indicate no CSF leak. Between 0.7 and 1.3 mg/L of βTP, two test lines would appear and classify the sample as in the “gray zone.” Samples that fall within the gray zone cannot be confidently diagnosed as negative or positive for the presence of CSF and therefore should undergo further testing before a clinical decision is made. Lastly, samples with βTP concentrations >1.3 mg/L would result in the appearance of three visible test lines, indicating the presence of a CSF leak.
Detection of Purified βTP
The performance of our rapid diagnostics test kit for the detection of CSF leaks was first evaluated by testing samples of purified, recombinant βTP in PBS. Solutions containing different concentrations of βTP were collected on a swab, transferred into diluent solutions, and then applied to the barcode-style LFA test strip. For all experiments, pink control lines became visible on the LFA test strips, indicating valid test results. βTP was also able to be detected at all concentrations tested, indicated by the formation of at least one pink test line on each LFA strip. More specifically, when the concentration of βTP was 0.3 mg/mL, a visible test line appeared at the T1 location. At a βTP concentration of 0.9 mg/mL, test lines appeared at the T1 and T2 locations. Lastly, at ≥3 mg/mL of βTP, test lines appeared at the T1, T2, and T3 locations ( Fig. 2 ).
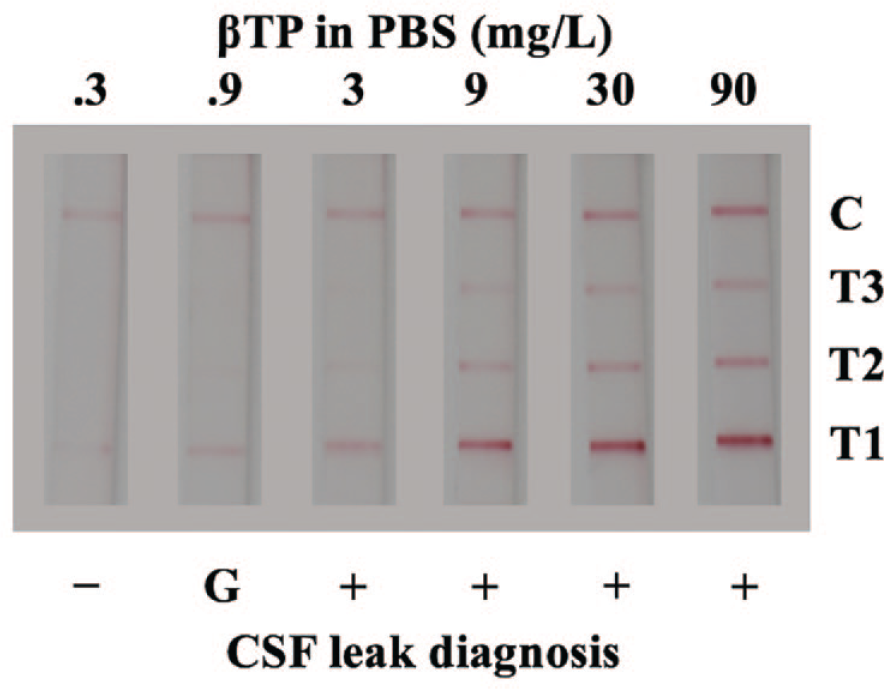
Diagnostic test kit results for the detection of recombinant beta-trace protein (βTP) in phosphate-buffered saline (PBS). Negative (–), gray zone (G), and positive (+) results are indicated.
Detection of Clinical Samples
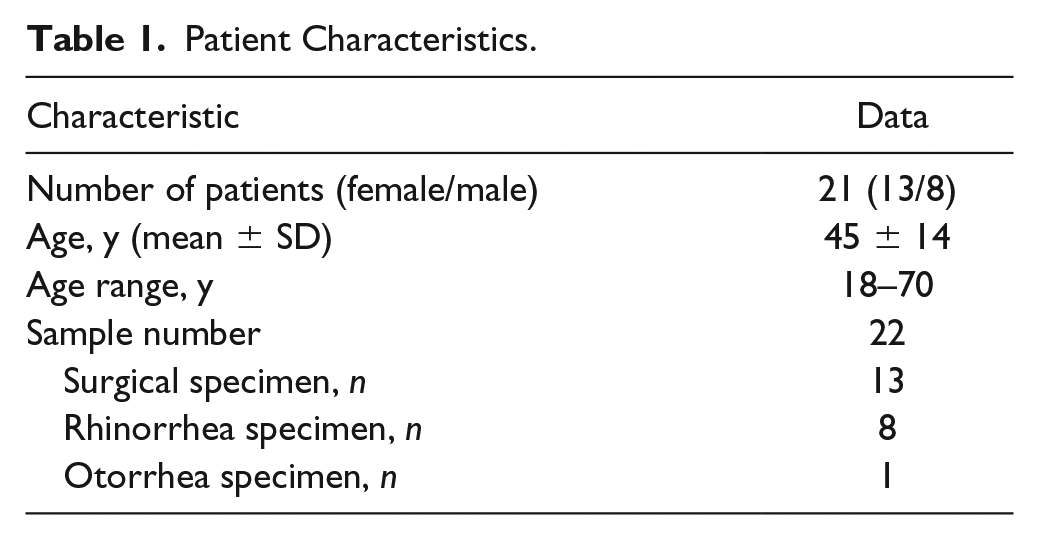
Next we evaluated the performance of our diagnostic test kit with clinical samples. To do this, we tested 22 samples from 21 patients. Of these samples, eight contained CSF from the periphery of the brain and 14 did not contain CSF. The demographics of the study population as well as the sample origins are summarized in Table 1 . Thirteen samples were collected from the site of surgical procedures, eight were rhinorrhea specimens, and one was an otorrhea specimen.
Patient Characteristics.
Each clinical specimen was collected on a swab, transferred into diluent solutions, and applied to the barcode-style LFA test strip. The results that were obtained are summarized in Table 2 (photographs of the test strips are provided in the supplementary information available online). Of the four surgical specimens containing CSF, three produced true-positive results and one produced a gray zone result. On the other hand, of the nine surgical specimens that did not contain CSF, seven produced true-negative results and two produced gray zone results. Rhinorrhea specimens were also examined, in which all three specimens containing CSF resulted in true-positive results and all five specimens that did not contain CSF resulted in true-negative results. An otorrhea specimen containing CSF was also tested, and it produced a true-positive result.
Summarized Diagnostic Test Kit Results.
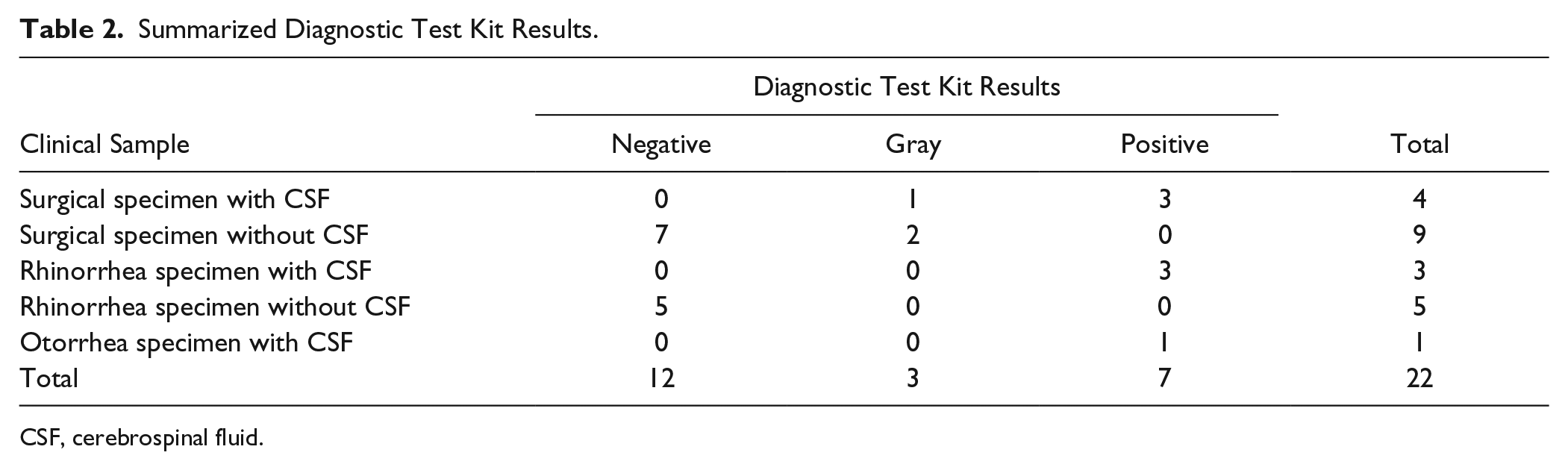
CSF, cerebrospinal fluid.
Three different strategies for interpreting the diagnostic test kit results were evaluated. In the first method, the gray zone results were interpreted as negative. For the second strategy, the gray zone results were interpreted as being positive. Lastly, in the third strategy, gray zone results were interpreted as being equivocal and ambiguous. The first two interpretation strategies allowed us to simplify the obtained results to provide the user with a binary answer as to whether the tested sample does or does not contain CSF. Ultimately, this allowed us to collapse the obtained results onto a 2 × 2 contingency table to characterize the diagnostic test kit performance ( Table 3 ). In the first method, where the gray zone was interpreted as a negative result, we obtained a sensitivity of 87.5%, specificity of 100%, positive predictive value (PPV) of 100%, negative predictive value (NPV) of 93.3%, positive likelihood ratio (+LR) of ∞, and negative likelihood ratio (–LR) of 0.125. In the second method, where the gray zone was interpreted as positive, we obtained a sensitivity of 100%, specificity of 85.7%, PPV of 80%, NPV of 100%, +LR of 7, and –LR of 0. In the third interpretation method, where gray zone results are considered equivocal and ambiguous, the results were not binary, so they could not be analyzed using a 2 × 2 contingency table, and thus sensitivity, specificity, PPV, and NPV could not be calculated. However, the LR for each detection region could be calculated, where a negative result (0 or 1 test line) had an LR of 0, a gray zone result had an LR of 0.88, and a positive result had an LR of ∞ ( Table 4 ).
Diagnostic Performance Using Binary Assay Interpretation.

PPV, positive predictive value; NPV, negative predictive value.
Diagnostic Performance Using Nonbinary Assay Interpretation.
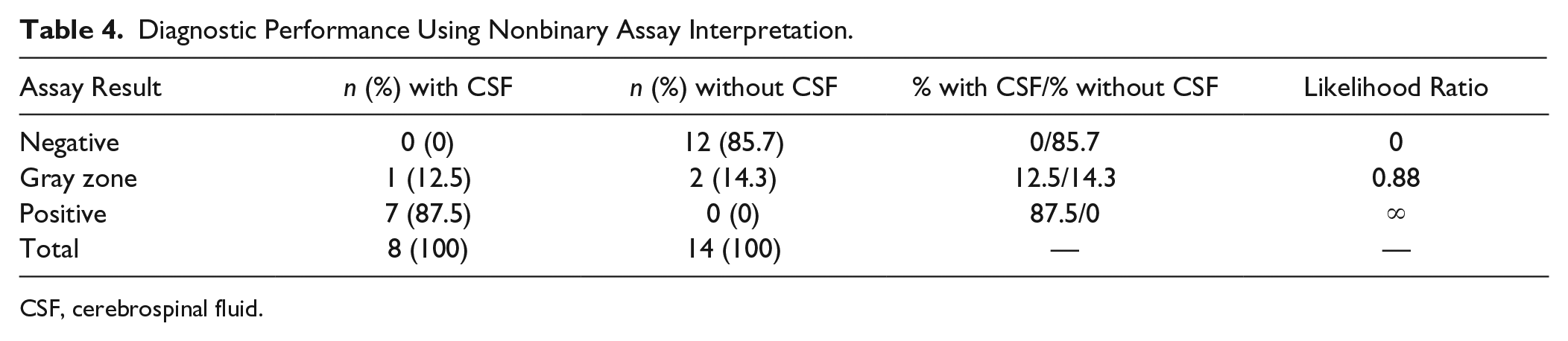
CSF, cerebrospinal fluid.
Discussion
The early and accurate diagnosis of CSF leaks is vital for the prevention of life-threatening complications such as meningitis. The quantification of βTP in rhinorrhea and otorrhea specimens using nephelometry has previously been reported as an effective method of diagnosing CSF leaks. Although it is more rapid than the gold standard laboratory technique of beta-2 transferrin electrophoresis, the nephelometry assay does require the use of expensive, centralized laboratory equipment that is not widely available in all clinical settings. In this work, we created a rapid diagnostic test kit that used a barcode-style LFA and validated its use for the equipment-free collection, dilution, and detection of CSF.
We first tested the rapid diagnostic test kit with purified, recombinant βTP in PBS. Our results demonstrate that the diagnostic test kit can detect for βTP in a semiquantitative manner, as seen by the increase in the number of red test lines visible on the LFA test strip with an increase in the concentration of βTP. More specifically, positive results were observed at ≥3 mg/L of βTP, a gray zone result was observed at 0.9 mg/L of βTP, and a negative result was observed at 0.3 mg/L of βTP. These results correspond relatively well with the cutoff values proposed by Bernasconi et al. 21 In addition, these test results obtained with swabs and disposable transfer pipettes were comparable with that of our previous work, which used no swabs and high-quality laboratory pipettes for collection and dilution. This is significant because it demonstrates that the samples could be collected, released, and diluted in a quantitative manner using low-cost and disposable materials.
All clinical specimens produced true-negative and true-positive test results, with the exception of three surgical specimens that produced results in the gray zone. One of these specimens contained CSF, whereas the other two did not. All three were collected at the sites of endoscopic surgeries, where a significant amount of blood was collected on the swab. The mean concentration of βTP in human serum has previously been reported as 0.59 mg/L with a range of 0.38 to 0.86 mg/L. 17 Recall that our diagnostic test kit produced gray zone results (two test lines) at 0.9 mg/L of recombinant βTP. Thus, it is possible that the gray zone results obtained for the two surgical specimens without CSF can be attributed to contamination with blood that has a βTP concentration at the upper end of the reported range. It is worth noting that the other seven surgical specimens with true-negative detection also contained blood; however, the blood could have been more dilute or at the lower end of the reported βTP concentration range for serum. Regarding the surgical specimen containing CSF that produced gray zone results, it is likely that the CSF was significantly diluted in other secretions to below the positive detection threshold of our diagnostic kit.
We evaluated three different strategies for interpreting and analyzing our diagnostic test kit results. The first two methods involved simplifying our results of negative, gray zone, or positive to a binary readout of negative or positive. The performance of the first method, in which gray zone results were interpreted as negative, is conducive for a rule-in test, because it was highly specific where false-positive results are extremely unlikely, and thus a positive result could be used to confidently confirm the presence of the CSF leak. For the second method, in which gray zone results are interpreted as positive, our diagnostic test kit became an effective rule-out test, because it has high sensitivity where false negatives are extremely unlikely, and thus it can be used to confidently send healthy patients home.
In the case that we designed our diagnostic test kit to provide only binary results, such as if the LFA test strip was printed with one test line as opposed to three test lines, a rule-out test would be desired. From a clinical perspective, a rule-out test is advantageous because it would allow clinicians to more confidently send healthy patients home who were suspected of having a CSF leak and otherwise would have been scanned and admitted into the hospital for observation or further invasive procedures. This would ultimately save hospital resources and minimize the number of healthy patients who would undergo unnecessary and costly workups such as magnetic resonance imaging (MRI) or computed tomography (CT) imaging. Although the rule-out test would be the most useful binary test for the detection of CSF leaks, it is not without its disadvantages. Note that the rule-out test has a very high sensitivity (100%) at the cost of a slightly lower specificity (85.7%). The PPV was calculated as 80%, meaning that 20% of the positive test results were actually false positives. Therefore, further testing would have to be performed for all patients with positive test results prior to intervention to confirm the presence of a leak.
To avoid having to choose between a binary test with either high sensitivity or high specificity, a nonbinary third interpretation strategy is presented, in which the gray zone results are treated as their own category indicating equivocal and ambiguous test results. In the case that the pretest odds for some unhealthy condition are known, LRs multiply the pretest odds to determine the posttest odds, which then can be converted to the posttest probability that a patient has some condition of interest. 23 Thus, the LR values of 0 for a negative test and ∞ for a positive test indicate that, regardless of the pretest probability, a negative test result confirms that the patient does not have a CSF leak, and a positive test result confirms a CSF leak. This is an improvement over the previously discussed second strategy, in which 20% of positive results were false positives. Lastly, gray zone results had an LR of 0.88, which provides very little useful information to influence the clinical diagnosis because it is close to 1. Therefore, patients who appear healthy but test within the gray zone would be identified as being at risk of having a CSF leak, and further noninvasive testing, such as beta-2 transferrin electrophoresis, should be performed prior to clinical decision making. It is worth noting that in our study, only 14% of patient samples produced gray zone results that would require further confirmatory testing. This is a significant improvement over the 45% of patients who would be required to receive further testing if the binary rule-out test format was implemented.
Altogether, the diagnostic test kit developed in this study costs less than $4 to produce at the laboratory scale and produces results in approximately 20 min. Using our kit, clinicians would be able to rapidly and accurately identify healthy individuals from a pool of patients with suspected CSF leaks. Ultimately, this would save hospital resources by minimizing the number of healthy patients who would otherwise be admitted to the hospital for multiday observation while waiting for beta-2 transferrin electrophoresis results as well as minimize the number of unnecessary and costly workups such as MRI or CT imaging.
Conclusions
In summary, we have developed the first rapid diagnostic test kit for the detection of CSF leaks. Every step, from sample collection through results interpretation, can be performed with minimal training and requires only the provided disposable materials, which make this kit well suited for use as a point-of-care diagnostic. Validation studies from testing clinical samples that either did or did not contain CSF demonstrated excellent predictive capabilities. Overall, our test kit has the potential to influence the clinical decision-making process by preventing unnecessary workups for healthy patients and rapidly confirming the presence of leaks in unhealthy patients. Ultimately, this will lead to the improved management and treatment of CSF leaks. This kit has the potential to transform patient outcomes.
Supplemental Material
Bradbury_et_al_SLAS_CSF_Manuscript_Supplementary_info – Supplemental material for Rapid Diagnostic Test Kit for Point-of-Care Cerebrospinal Fluid Leak Detection
Supplemental material, Bradbury_et_al_SLAS_CSF_Manuscript_Supplementary_info for Rapid Diagnostic Test Kit for Point-of-Care Cerebrospinal Fluid Leak Detection by Daniel W. Bradbury, Ashley E. Kita, Kensuke Hirota, Maie A. St. John and Daniel T. Kamei in SLAS Technology
Footnotes
Supplemental material is available online with this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D. W. Bradbury, A. E. Kita, M. A. St. John, and D. T. Kamei are inventors of the device being studied and may benefit financially if the patent application is approved and the device is eventually manufactured and marketed.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health grant 1R21NS099800-01 and a 2016 AAO-HNS Core Resident Research Award.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.