
Abstract
Three-dimensional (3D) bioprinting enables the creation of tissue constructs with heterogeneous compositions and complex architectures. It was initially used for preparing scaffolds for bone tissue engineering. It has recently been adopted to create living tissues, such as cartilage, skin, and heart valve. To facilitate vascularization, hollow channels have been created in the hydrogels by 3D bioprinting. This review discusses the state of the art of the technology, along with a broad range of biomaterials used for 3D bioprinting. It provides an update on recent developments in bioprinting and its applications. 3D bioprinting has profound impacts on biomedical research and industry. It offers a new way to industrialize tissue biofabrication. It has great potential for regenerating tissues and organs to overcome the shortage of organ transplantation.
Introduction
Organ transplantation is one of the major treatments for many end-stage organ diseases. The supply of donors is, however, limited. The emerging of tissue biofabrication technologies 1 can one day help overcome the tissue or organ shortage.
Conventional tissue biofabrication involves seeding cells and biomolecules within a scaffold that possesses a porous structure to mimic properties of extracellular matrix (ECM). The scaffold-based strategies have been successfully used for engineering various tissue constructs, such as bone, skin, and cartilage.2,3 Nevertheless, these approaches often fail to imitate complex structures of native tissues and are incapable of placing multiple types of cells in desired positions or in an orderly fashion.
Three-dimensional (3D) printing, also known as rapid prototyping or additive manufacturing, 4 can revolutionarily solve these problems. The concept of 3D printing was developed in the early 1980s. The first “3D printer” was designed by Sachs et al. in 1993 to print nonviable materials, such as plastics and metals. 5 Since then, a number of 3D printers have been invented. 6 Inspired by recent advances in tissue engineering and regenerative medicine, 3D printing has been successfully adapted for tissue biofabrication.7,8 Bioprinting has been defined as the deposition of biological materials along with living cells layer by layer using computer-aided transfer processes.9,10 This approach has high throughput and is scalable and reproducible. It allows for organizing multiple types of cells in a desired structure. 11 Using this technique, one can create tissue constructs with heterogeneous cell placements and vascular structures capable of recapitulating structural features of human tissues and organs.
In general, 3D bioprinting includes three steps: preprocessing, processing, and postprocessing.12–14 Preprocessing includes the generation of a computer-aided design (CAD) of a tissue or organ of interest. A blueprint of tissues and organs can be generated using medical imaging techniques, such as computer tomography (CT) or magnetic resonance imaging (MRI).15–17 The blueprint is then converted into a heterogeneous model describing material and cell composition and distribution. The 3D structures are recreated by reducing the particular prototypes to a series of two-dimensional (2D) layers. The printing process is the simultaneous deposition of cells and biomaterials using computer-aided precision deposition techniques in a layer-by-layer fashion. The postprocessing is the incubation of the printed tissue constructs in a bioreactor.4,18,19
In this review, we first examine the current technologies in bioprinting, along with the broad range of biomaterials used. We thereafter present an overview of 3D tissue and organ printing with a specific focus on the 3D printing of vascularized tissue and organ constructs.
Bioprinting Modalities
Inkjet Bioprinting
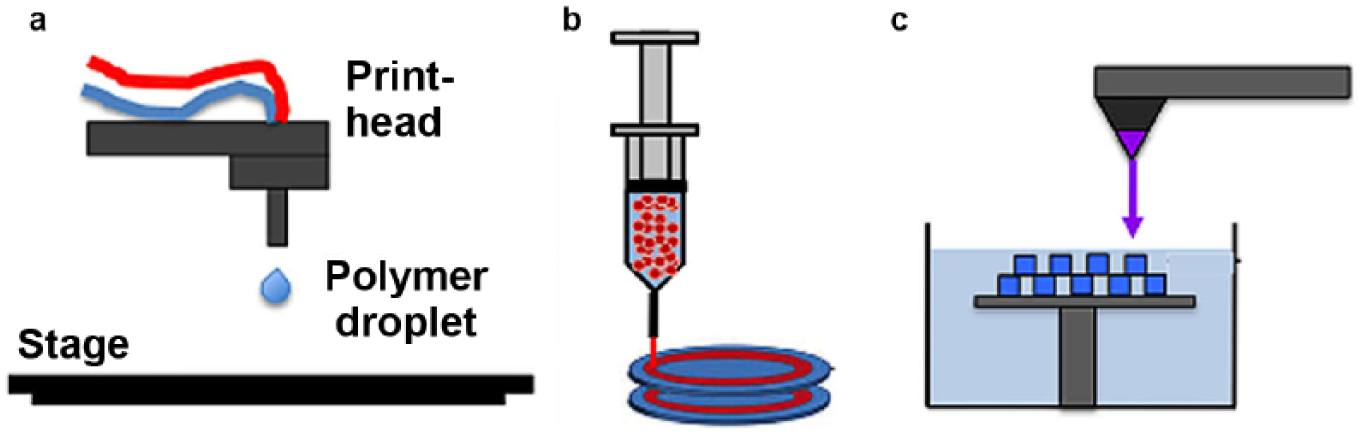
In inkjet bioprinting, cells and biomaterials are patterned into desired substrates in the form of droplets, as shown in Figure 1 . A structure is formed by repeatedly depositing droplets at predesigned locations. 20 Different types of inkjet bioprinters, such as thermal, piezoelectric, and pneumatic microvalve-based inkjet printers, have been developed. In thermal inkjet bioprinting, small air bubbles are generated by heating in the printhead. The bubbles collapse to provide pressure pulses that eject bioink (a mixture of cells and biomaterials) drops out of a nozzle. The volume of the droplets varies from 10 to 150 pL, depending on the applied temperature gradient, frequency of the current pulse, and viscosity of the bioink. 21 The localized heating in a thermal printer lasts for a very short duration of ~2 µs. 22 This causes less effect on cells during printing. In piezoelectric inkjet bioprinting, a piezoelectric crystal induces a shape change and creates an acoustic wave when the voltage is applied. The acoustic wave breaks the bioink into many droplets that are ejected due to a transient pressure from the nozzle.23,24 In pneumatic microvalve printing, the bioink is regulated under a constant pneumatic pressure.25–27
(
Inkjet bioprinting has the advantage of contactless printing. The size, deposition rate, and position of droplets can be altered easily in inkjet bioprinting, allowing for the creation of defined patterns and concentration gradients of chemicals and cells. 28 A 3D structure with irregular shapes or complex structures, for example, branch or tubular structures, can be created using inkjet bioprinting.29,30
While inkjet bioprinting provides a high spatial resolution, the bioink needs to meet many requirements. Inkjet bioprinting uses a biomaterial solution with a low viscosity to avoid clogging and droplet ejection. Thus, it has limited capability of processing high viscous biomaterials. 24 The upper limit of the viscosity is in the order of 0.1 Pa/s. 31 To date, inkjet bioprinting is mainly used for printing small scaffolds. Inkjet printheads with multiple nozzles have been developed to increase the printing speed and fabricate larger cellular constructs. The throughput printing capability can also be improved by integrating microvascular multinozzle printheads with direct ink printing. 32
Extrusion Bioprinting
In extrusion bioprinting, the bioink is extruded out of a nozzle tip continuously in a form of line structures driven by a pneumatic pressure or a mechanical piston. 4 The extrusion printing produces filaments instead of droplets. Biomaterials used for extrusion bioprinting should have a high enough elastic modulus and sufficient loss modulus. They should be nearly fluid-like so that they can be extruded through the tip. Meanwhile, the extrusions should be strong enough to maintain the shape during and after the printing. The biomaterials for microextrusion printing are versatile. For instance, thermoplastic biomaterials can be printed by heating and extruding them as liquid, which is subsequently solidified to form a shape. 4 The extrusion printed scaffolds usually exhibit better structural integrity. The microextrusion technique could be adopted to print a high viscous cell suspension.33,34 Nevertheless, its resolution is relative low compared with that of inkjet and laser bioprinting. 31 Other limitations include stress-induced cell deformation and limited material selection.
Laser Bioprinting
Laser bioprinting uses a laser-induced forward transfer to transport droplets. 35 In principle, laser printing involves the use of a pulsed laser beam, a “ribbon” with a donor transport support, and a source film containing the printing materials. The source film is supported on a ribbon, which absorbs the laser energy. The laser pulse generates high energy to produce a high-pressure bubble that ejects material droplets from a source film onto a collecting substrate. 36 Initially, laser bioprinting was used to pattern cells or polymers in two dimensions. Only in recent decades can a 3D structure be printed by alternating the deposition of hydrogels and cells for multiple cycles using laser pulse–generated droplets.37,38
Laser bioprinting is nozzle-free. It eliminates the clogging that occurs more often in inkjet and extrusion bioprinting. It is capable of printing high-viscose bioinks. Moreover, it can deposit cells at a density of up to 108 cells/mL with a very high resolution. 22 The printing resolution of laser bioprinting is dependent on the viscosity of bioinks, the speed of the laser printing, and the energy and pulse frequency of the laser used. Laser bioprinting permits single-cell manipulation and precise control of the positions of cell droplets. 38 However, the cell viability is often lower than that of inkjet bioprinting, because laser energy causes cell death during bioprinting.13,39
Printable Biomaterials
One of the major challenges of bioprinting is to discover new printable biomaterials in which cells can survive and retain their potency. 40 The biomaterials should not only have appropriate viscosity but also possess a high mechanical strength, 41 so internal pore structures of printed scaffolds will not collapse during layer-by-layer deposition. Moreover, they should be biocompatible, less immunogenic, and biodegradable. 42
The biomaterials used for printing can be divided into synthetic and natural polymers. Synthetic polymers are processable and have mechanical strengths needed for printing. 43 They allow for precise control over the molecular weight, functional groups, and other chemical properties. Nevertheless, synthetic polymers typically lack cell-responsive motifs, hindering cell proliferation and differentiation. 44 In contrast, natural polymers, including polysaccharides and proteins, are biodegradable and highly biocompatible; however, they are usually mechanically weak.
Poly(ethylene glycol) (PEG) is one of the most common synthetic polymers. PEG is a water-soluble polymer that has been widely used for cell encapsulation. It can be functionalized with cell adhesion motifs, making it more biocompatible.40,45 To make it printable, PEG can be modified with acrylate groups, such as photocrosslinkable poly(ethylene glycol) diacrylate (PEGDA).46,47 PEGDA with different molecular weights has been synthesized and used to alter the mechanical strengths of PEG at different concentrations. 48 Recently, a triblock copolymer, based on poly(N-(2-hydroxypropyl)methacrylamide lactate) and PEG, was developed and used as photopolymerizable, thermosensitive, and biodegradable biomaterials for printing. 49
PEG is a nonbiodegradable polymer, which limits its application. Synthetic biodegradable polymers, such as poly(lactic acid) (PLA), poly(lactic-co-glycolic acid) (PLGA), and poly(ε-caprolactone) (PCL), are promising materials for bioprinting. 50 The degradation rate of PCL is considerably slower than that of PLA and PLGA. PCL is often employed as a printing component due to its low melting temperature of 60 °C. 51 The limitation of polylactone-type polymers is the release of acidic matters during degrading, causing inflammation of surrounding tissues.
Collagen is a major ECM protein. 52 It has a triple-helix structure composed of three polypeptide helices. Each peptide consists of three repeat units of Gly-Pro-X, where X can be any amino acid. Collagen mainly comprises three amino acids: glycine, proline, and hydroxyproline. It contains arginine–glycine–aspartic acid (RGD) amino acid sequences binding to integrin. Cells can adhere to and proliferate in collagen. Collagen as a biocompatible and biodegradable polymer has been widely used to regenerate skin, bone, cartilage, and islets.31,33,53,54 Collagen has been extensively used in 3D bioprinting.33,55,56 However, it is relatively weak in mechanical strength. It does not support long-term tissue and organ cultures. 53
Gelatin, derived from native collagen, also contains a RGD cell recognition signal capable of binding to the cell surface receptors. Gelatin is water soluble, biodegradable, noncytotoxic, and nonimmunogenic. 57 However, gelatin gels are not stable at body temperature. Gelation can be modified by appending methacrylate groups to the gel’s amine side groups. The modified gelatin gel is photocrosslinkable in the presence of a photoinitiator.58–62 The rheological property methacrylated gelatin (GelMA) could chemically be modified. 59 For example, acetylation of free amino groups could alter the viscosity of GelMA. 58 GelMA hydrogels with a high cell viability have been printed and used for creating cartilage and cardiovascular structures.61,62
Hyaluronic acid (HA) is a linear polysaccharide composed of β-1,4-linked
Fibrin is a natural protein-based material. 66 It can bind to many growth factors. Fibrin gels have been printed to release vascular endothelial growth factor (VEGF) to enhance vascularization.56,67 It has been used to print thick vascular networks 68 and tubular tissue structures, such as renal proximal tubules. 69
Alginate is a natural polysaccharide isolated from brown algae.
70
It is a copolymer with linear blocks of (1,4)-linked β-
Most biopolymer hydrogels are mechanically weak. To increase the mechanical strength of these gels, thermoplastic materials can be deposited along with these biomaterials during printing. For instance, a multinozzle deposition system was developed to deposit both biopolymer and thermoplastic polymer for fabricating heterogeneous tissues with enough mechanical strength. 74 Boere et al. reinforced the GelMA with a thermoplastic polymer blend of poly(hydroxymethylglycolide-co-ε-caprolactone)/poly-(ε-caprolactone) (pHMGCL/PCL) functionalized with a methacrylate group. 60 The thermoplastic polymer blend, covalently bonded to the GelMA through photopolymerization, resulted in a significant increase in the interface-binding strength between the materials. Therefore, the reinforced hydrogels demonstrated an improved resistance to axial and rotational forces. 60
Decellularized ECM (dECM), in which cells are removed from tissue and organs using physical methods or chemical or biologic agents, could be another excellent biomaterial for printing, as it captures key bioactive signals of native tissues.75,76 Hydrogels printed with tissue-specific dECM are capable of mimicking the composition of native tissues and therefore creating an optimal microenvironment to support biological tissue response. 77
Ceramic or glass particles can be incorporated into 3D bioprinted scaffolds. The ceramic or glass particles, mixed with hydrogels, have been found to reinforce the mechanical strength and improve the bioactivity of polymer matrixes.78,79 Hydroxyapatite is the major inorganic composition of bone. It is widely used in bone tissue engineering because of its excellent biodegradability, osteoconductivity, and osteoinductivity. Hydroxyapatite–polymer composite hydrogels have been made for printing by mixing hydroxyapatite particles with polymers, such as silk, collagen, and alginate.80–82 The addition of bioactive glass into scaffolds not only enhances the mechanical strength but also increases the cell proliferation and enhances the potency of mineralization.83–85 These combinations in 3D hard tissue printing are worth exploring.
Tissue Biofabrication
Scaffold and Tissue Prosthesis Printing
Bioprinting has been applied initially in fabricating tissue scaffolds, such as bone scaffolds. 86 In bone scaffolding, a high porosity stimulates bone ingrowth. However, it diminishes the mechanical strength of the scaffold. 87 The geometry of pores, such as the connectivity and shape of the pores, affects new bone formation within the scaffolds. To date, a number of methods, including freeze drying, salt leaching, thermally induced phase separation, and electrospinning,88,89 have been employed to create scaffolds with a tailored pore structure and composition. While these approaches enable the formation of a tailored pore structure, control over the shape and porosity of the scaffold is hard to achieve with them. These controls can, however, be easily realized with 3D bioprinting. 90 Moreover, a gradient of compositions or pore structures can be formed with 3D bioprinting.3,91 For instance, Sun et al. printed silk or hydroxyapatite bone scaffolds. 81 These scaffolds allow for simultaneously growing human bone marrow–derived mesenchymal stem cells (hMSCs) and human mammary microvascular endothelial cells (hMMECs). Fielding and Bose incorporated silica (SiO2) and zinc oxide (ZnO) into 3D printed tricalcium phosphate scaffolds and tested the biocompatibility of the scaffolds in bicortical femur defects of a murine model for up to 16 weeks. 92 Increased early bone formation and neovascularization were found in the defect implanted with these scaffolds. Monetite (dicalcium phosphate anhydrous) is biodegradable and osteoinductive. Tamimi et al. deveploped customized monetite grafts by 3D printing. 93 They demonstrated the osseointegration of dental implants in bone augmented with printed onlays. A composite of collagen and calcium phosphate mimicking the composition of natural bones has been printed using a low-temperature 3D bioprinting technique. 82 The printed scaffolds were macroporous, mechanically strong, and osteoconductive. In addition, Loozen et al. printed gene-deliverable 3D porous hydrogels by printing calcium phosphate microparticles suspended in alginate. 80
Bioactive glass has been incorporated into polymer scaffolds to increase their bone formation ability. Wang et al. developed alginate hydrogels supplemented with bioactive glass in which bone cells were embedded and printed altogether. 83 The addition of bioactive glass increased the proliferation and mineralization of bone-related SaOS-2 cells in the printed hydrogels. 83 Serra et al. fabricated composite scaffolds by printing bioactive glass with the PLA polymer. 94 The printed scaffolds possessed an interconnected porosity and controlled geometry that supported cell adhesion. 94
In another work, Li et al. designed a biocompatible supramolecular polypeptide–DNA hydrogel by mixing a polypeptide–DNA conjugate with a DNA linker for bioprinting. 95 The conjugate prepared by grafting multiple DNAs onto a polypeptide backbone was crosslinked by a DNA linker containing sequences complementary to the DNA in the conjugates. The printed DNA hydrogel was mechanically stable and biodegradable, suitable for constructing tissue scaffolds.
CAD has been used to create customized, patient-specific bone constructs. For instance, a patient-specific actual replica can be bioprinted after measuring a bone defect using CT. 96 Li et al. reconstructed a 3D model of a patient’s alveolar bone defect and then fabricated PLGA and tricalcium phosphate composite scaffolds identical to the defect. 97 He et al. developed soft-tissue prostheses using a method called scanning printing polishing casting (SPPC). 98 A negative mold of the prosthesis was generated based on 3D data collected with a scanner. The mold was printed with a desktop printer and polished using a chemical method. Various prostheses, such as artificial ears and hands, have been biofabricated using such a low-cost desktop 3D printer. 98
Tissue and Organ Bioprinting
Cell seeding to casted scaffolds has disadvantages due to its insufficient seeding capability. 99 3D bioprinting can overcome these challenges. 3D bioprinting allows for precise placement of high-density cells in a desired location. Its ability to place multiple types of cells in an orderly fashion mimics heterogeneous architectures of native tissues. One major concern of printed cell-laden scaffolds is acute cell death due to the dispensing pressure and nozzle diameter. To improve cell viability, the printing condition needs to be optimized. The materials used for forming bioinks need to be carefully selected as well. Here we discuss several examples of 3D tissue and organ bioprinting.
3D hydrogels containing one or multiple types of cells have been successfully printed. Rajaram et al. printed alginate-HA hydrogels containing Schwann cells for peripheral nerve regeneration. 100 In their work, an alginate-HA strand was printed into a calcium chloride crosslinking solution supplemented with polyvinyl alcohol and low concentrations of polyethylenimine. The printed hydrogels showed an improved structural integrity and a high cell viability. Xu et al. constructed tissue mimics containing three different types of cells by inkjet printing. 101 They demonstrated that cells could survive, migrate, and proliferate in the printed hydrogels. The bioprinted constructs formed a bone tissue with adequate vascularization in vivo. Neufurth et al. used a sodium alginate hydrogel stabilized with gelatin for encapsulating bone-related SaOS-2 cells. 102 The addition of agarose and the calcium salt of polyphosphate led to a significant increase in cell proliferation level. All this indicates that 3D bioprinting has the ability to create tissue constructs with a heterogeneous structure and cell distribution that mimic those of natural tissue architectures.
3D bioprinting has been extensively used to biofabricate cartilage tissues by printing chondrocytes into hydrogel scaffolds. Cohen et al. prepared 3D implants with arbitrary geometries using alginate and chondrocytes. 103 The printed scaffolds had a high cell viability. Shim et al. fabricated dual-cell-laden osteochondral tissues by dispensing thermoplastic biomaterials using a multihead 3D printer. 51 A thermoplastic polymer such as PCL was used to enhance the mechanical strength of the printed construct. Osteoblasts and chondrocytes were separately encapsulated in the hydrogels. A high cell viability was maintained during cell culture. Cartilage tissues have also been fabricated by printing human articular chondrocytes with poly(ethylene glycol) dimethacrylate (PEGDMA). 46 Functional neocartilage formation was observed in these printed constructs treated with growth factors and chondrogenic factors. Pescosolido et al. printed hydrogels consisting of semi-interpenetrating networks of HA and hydroxyethyl-methacrylate-derivatized dextran (dex-HEMA). 63 The hydrogel is photocrosslinkable and mechanically stable. The encapsulated chondrocytes demonstrated a high cell viability. Recently, bilayered osteochondral models were printed using hydrogels incorporated with cell-laden microcarriers. 104 The addition of microcarriers increased the mechanical strength of the hydrogels. The formation of a microcarrier–cell complex led to a higher cell viability within the printed hydrogels.
Human skin has a multilayered structure consisting of epidermis in the outermost layer and dermis in the inner layer. Keratinocytes and fibroblast are the predominant cell types in the epidermis and dermis, respectively. 3D printing has been applied to engineer these stratified human skins. Lee et al. printed a multilayered structure with a high cell viability for engineering skin graft.33,105 In their work, fibroblasts and keratinocytes were printed as constituent cells to represent the epidermis and dermis, respectively. The printed tissue construct was similar to human skin tissue morphologically and biologically. Compared with the conventional method, the 3D printing provided better control over the geometry of the skin. The printed skin exhibited better shape retention during in vitro cultures.
Heart valves have been successfully bioprinted. 106 The printed constructs mimic the heterogeneous structure of aortic valve root wall and trileaflets. Using a PEGDA hydrogel, Hockaday et al. printed an aortic valve replicating the mechanical heterogeneity of an aortic valve. 107 The aortic valve was found to maintain a high cell viability for up to 21 days. 107 Duan et al. printed aortic valve conduits using alginate-gelatin hydrogels encapsulating sinus smooth muscle cells (SMCs) in the valve root and aortic valve (leaflet) interstitial cells (VICs) in the leaflet. 108 Both SMCs and VICs have a high survival rate, good spreading, and phenotype retention in vitro. 108 A trileaflet aortic valve was also printed using photocrosslinkable hydrogels consisting of methacrylated HA and GelMA. 109 Human aortic valve interstitial cells (HAVICs) encapsulated within the printed hydrogels exhibited a high cell viability and remodeling potential.
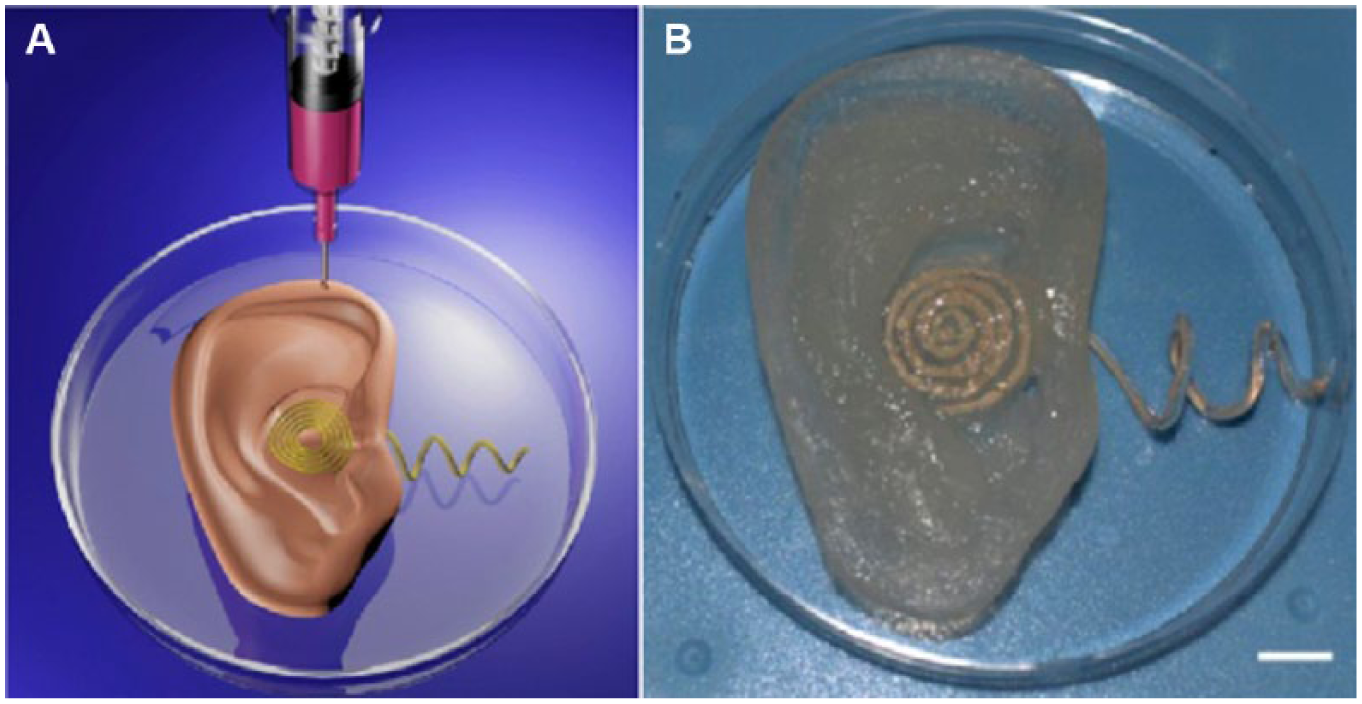
3D bioprinting has the ability to create biological tissues with functional properties by simultaneously printing cells and functional materials. Mannoor et al. developed 3D printed bionic ears by integrating engineered ears with functional electronics, as shown in Figure 2 . 110 Alginate hydrogels seeding with chondrocyte were printed into the geometry of a human ear. Conducting silver nanoparticle–infused silicone was printed into an inductive coil antenna connected to cochlea-shaped electrodes supported on silicone. The printed ear could maintain the shape during the in vitro cell culture. Cartilage was formed around the inductive coil antenna, and the neocartilage exhibited excellent morphology and tissue-level viability. Further, the printed ear was capable of receiving electromagnetic signals and listening to stereo audio music.
(
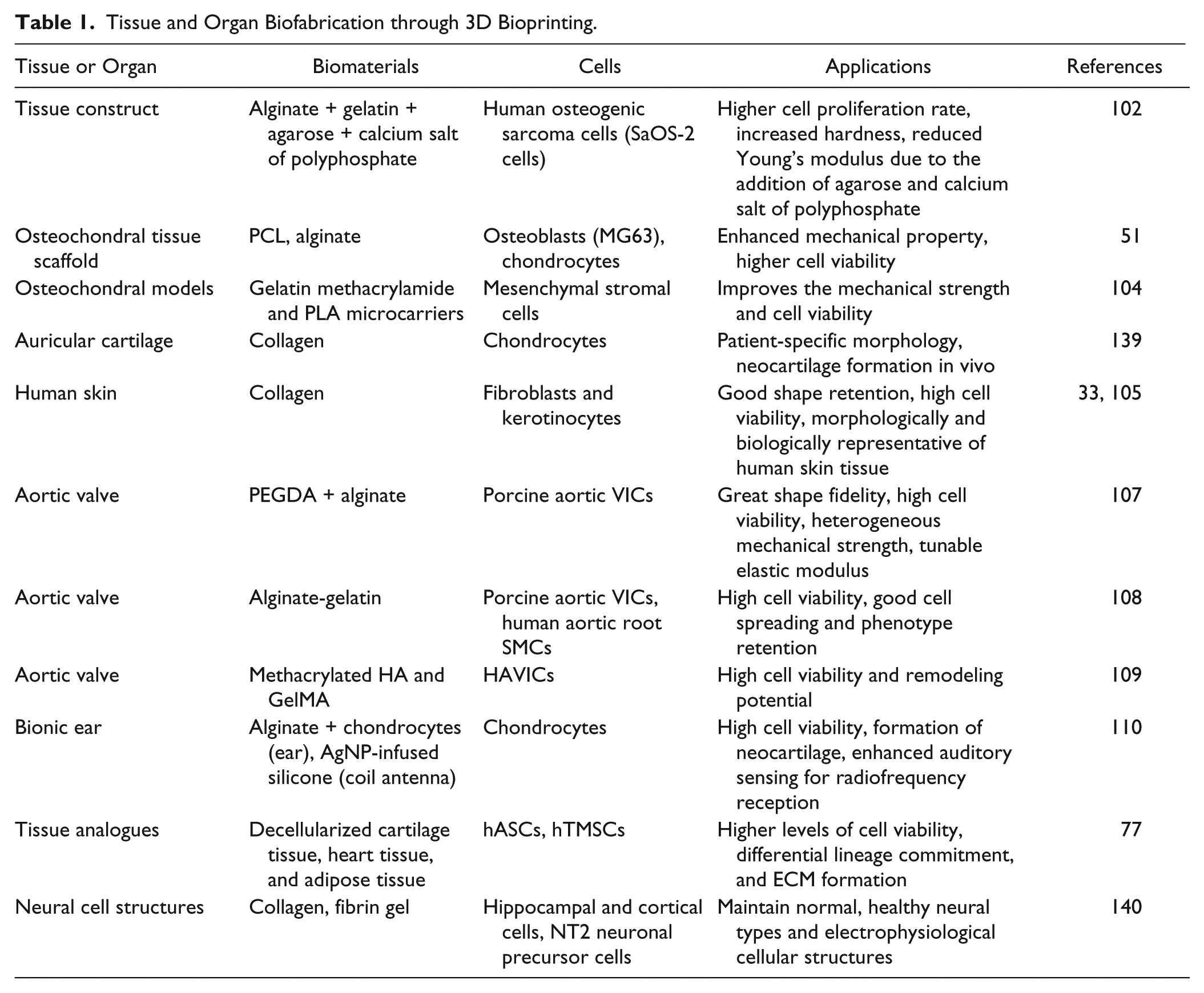
The printing of tissues and organs with natural biomaterials, such as dECM, has been attempted. An dECM hydrogel, combining with different types of cells, is a promising bioink for fabricating biologically functional tissues. For instance, Pati et al. printed tissue constructs using dECM including adipose, cartilage, and heart tissues, in which stem cells, such as human adipose-derived stem cells (hASCs) and human inferior turbinate tissue-derived mesenchymal stromal cells (hTMSCs), were encapsulated. 77 Advances in 3D printing enable the creation of microorgans simulating the physiological microenvironments for studying pathogenesis or for high-throughput drug screening or validation.111,112 For instance, Matsusaki et al. developed human tissue chips by printing different types of cells layer by layer. 113 A cervical tumor model was developed by assembling cells and hydrogels using 3D printing. 114 Compared with the conventional 2D model, 3D printed tumor models led to a higher cell proliferation, matrix metalloproteinase (MMP) protein expression, and chemoresistance. Lee et al. built modulated microfluidic systems using 3D printing and applied a microfluidic device as a biosensor for cancer diagnosis. 115 Table 1 summarizes tissues and organs biofabricated through 3D bioprinting.
Tissue and Organ Biofabrication through 3D Bioprinting.
Bioprinting 3D Microchannels
Despite great successes in engineering 3D tissue constructs possessing an adequate cell density and defined structure, the vascularization of thick tissue constructs remains a critical challenge. 116 Although vascularization can happen with biochemical stimulation by growth factors, the process of angiogenesis could take 1–2 weeks. Bioprinting microchannels, as summarized in Table 2 , is considered one of the promising approaches to achieving adequate vascular perfusion. The development of vascular networks could facilitate the transportation of nutrients, growth factors, and waste removal, thereby increasing the cellular viability.116,117
Blood Vessel–Like Structures Created by 3D Bioprinting.
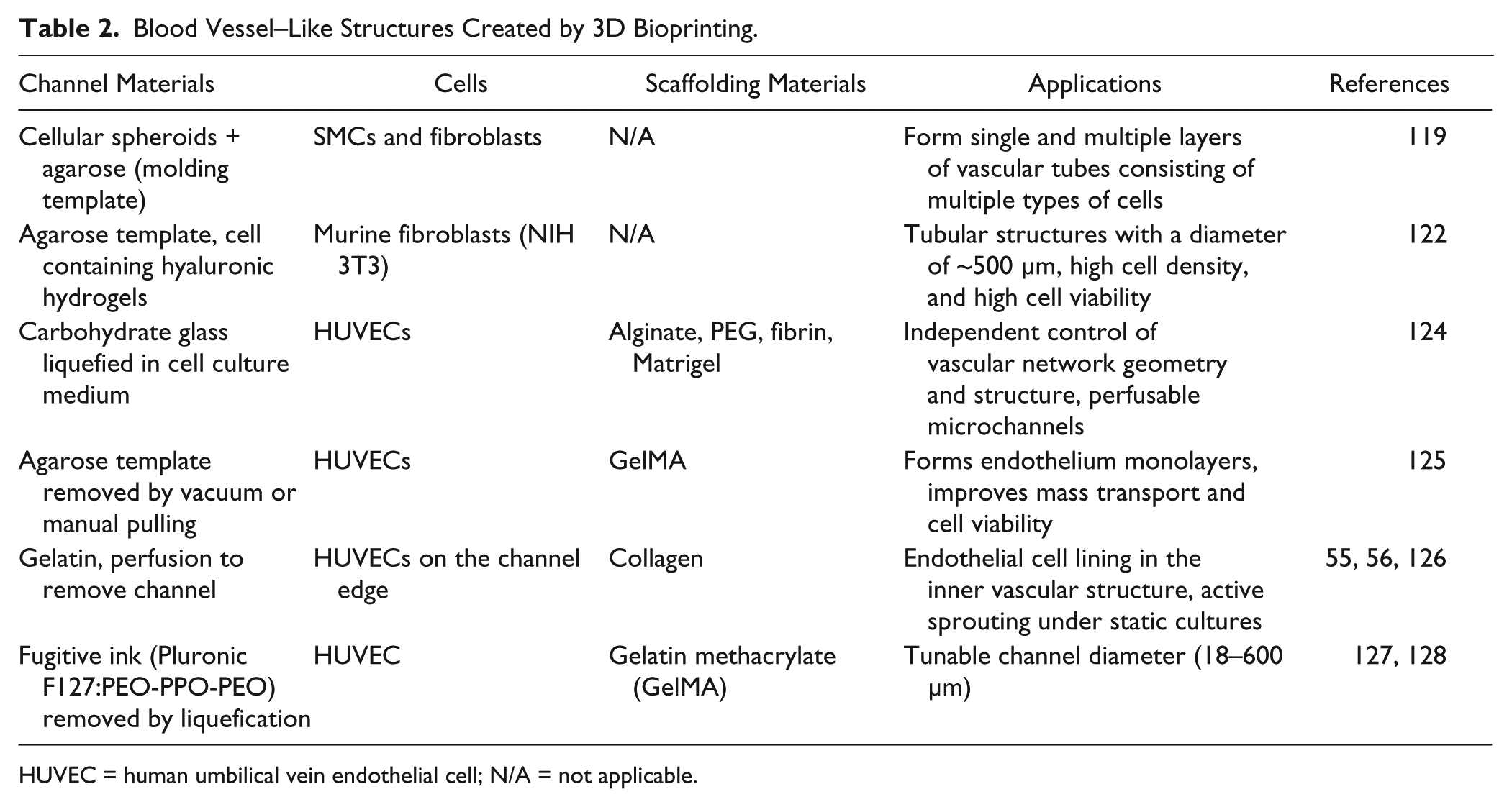
HUVEC = human umbilical vein endothelial cell; N/A = not applicable.
Parallel channels have been created in the tissue structures by simply printing a tubular structure in the hydrogels. Huang et al. printed gelatin-alginate-fibrinogen hydrogels with internal channels for pulsatile culture. 118 Adipose-derived stem cells were printed with these hydrogels with microchannels of ~3 mm in diameter. This method is simple and template-free. It is, however, incapable of replicating a complex hierarchical structure of native 3D vasculatures. Furthermore, the size of the channel is relatively bigger.
In another work, Norotte et al. printed vascular tissue construct using continuous dispensing of multicellular spheroids or cylinders around the sacrificial templates. 119 Since then, scaffold-free vascular tissue spheroids have been widely used to assemble vascular tubes. This scaffold-free method avoids the possible rejection or inflammation of biomaterials.120,121 In Norotte et al.’s work, cellular spheroids with a size of 300–500 µm serve as basic building blocks. An agarose rod was employed as a sacrificial template in which tissue spheroid deposited surrounding the template to form a tubular structure ( Fig. 3 ). A fusion process postprinting taking up to 1 week was required, however. Multicellular cylinders were introduced to increase the throughput and printing speed, leading to shortening of the fusion process to 2–4 days. Single- and double-layer tubes containing multiple types of cells were built. 119 Based on Norotte et al.’s method, Skardal et al. developed vessel-like constructs by printing cell-containing hyaluronan hydrogels around a sacrificial agarose template. 122 Different PEG derivatives were developed as crosslinkers to tailor the rheological property and mechanical strength of hyaluronan hydrogels. It was found that four-arm-based crosslinkers consisting of a compact core and four functionalized PEG chains improve the mechanical strength of the hydrogels compared with linear PEG derivatives. In these works, templates were printed to support mechanically weak cellular spheroids and removed after cell fusion. Recently, Kucukgul et al. developed macrovascular aortic tissues using mouse embryonic fibroblast cell aggregates and hydrogels. 123 A computer model mimicking a real human aorta was generated from medical images. Cell aggregates were then printed into a tubular structure. It was found that printed constructs offered a high cell viability and a robust tissue formation.
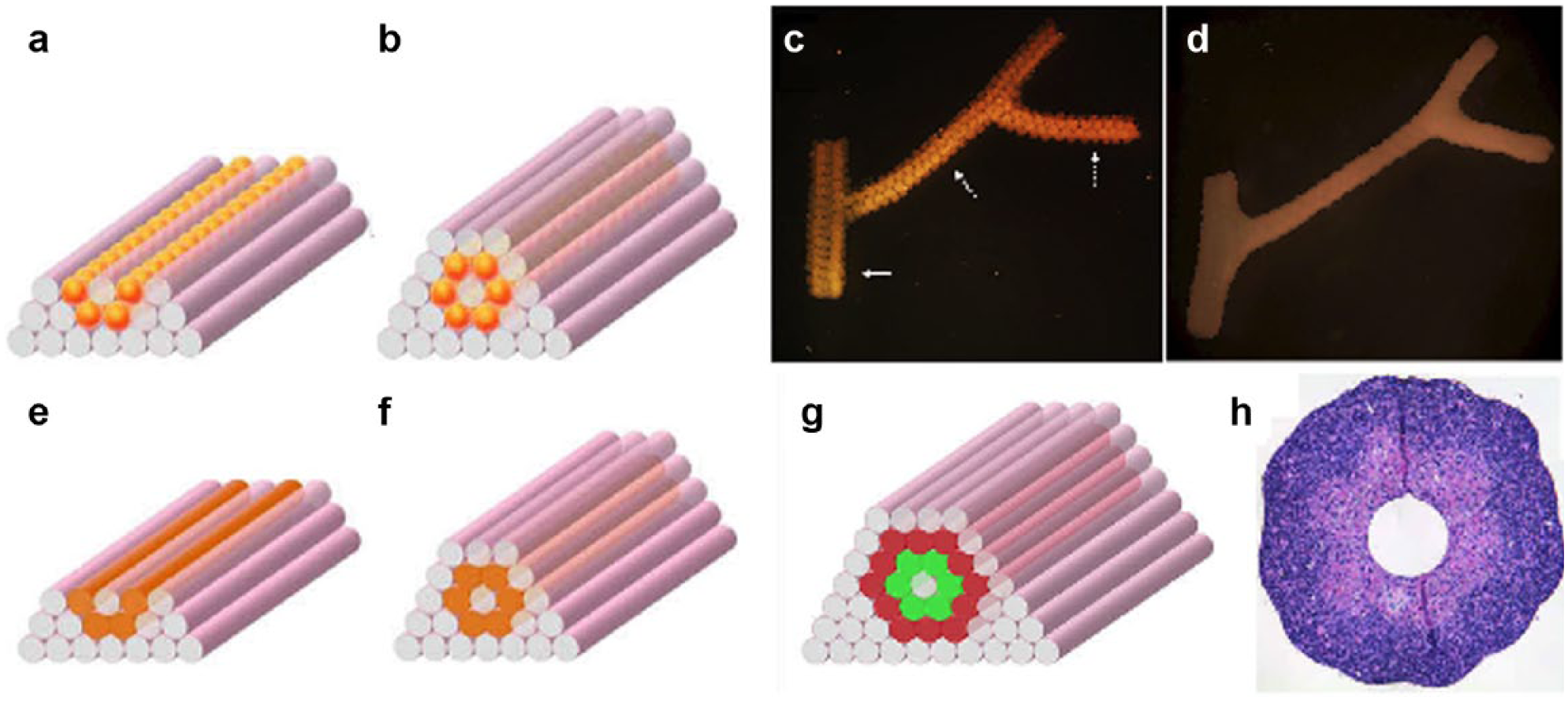
(
Sacrificial materials have been widely used to form microchannels and cavities. Sucrose, glucose, and dextran have been printed into interconnected microchannels that can be dissolved in cell culture media, resulting in the creation of vascular channels. 124 The channels can be perfused with blood under a high-pressure pulsatile flow. Endothelial cells can be lined in these channels. This vascular casting approach offers an independent control over the template geometry and formation of complex vascular structures. Microchannel networks can also be printed using agarose that can be aspirated in vacuum or manually pulled out. 125 Lee et al. developed a perfused vascular channel in which the vascular channel was created by printing endothelial cells with gelatin. 18 Gelatin becomes a solid at room temperature, while it becomes a liquid at 37 °C. Hollow microchannels can be printed by heating the gelatin whiling printing. Endothelial cells, mixed with gelatin before printing, migrated and attached to the surface of the lumen.55,56,126 The fluid active angiogenic sprouting was observed in a static culture condition. Cell viability in the channel was found to be higher than 90%. 55 Recently, fibrin gel containing endothelial cells and fibroblasts was printed in the area between vascular channels to promote angiogenesis. 56 As a result, capillary networks connecting with perfused vascular channels (~1 mm) were formed through a maturation process after printing. Capillary networks started to form by self-assembling endothelial cells in the printed fibrin gels after culturing for 3–4 days. The capillary networks became denser and integrated well with endothelial cells sprouted from vascular channels.
Although significant progress has been made in the development of microvascular networks, the biofabrication of vasculature networks with complicated and hierarchical structures remains a challenge. The resolution of the printed channels was in the range of a few hundred micrometers. Only in recent years has Lewis’s group developed a novel approach for the omnidirectional printing of biomimetic microvascular structures using fugitive ink. 127 Fugitive ink composed of Pluronic F127 is a triblock copolymer with a hydrophobic poly(propylene oxide) (PPO) and two hydrophilic poly(ethylene oxide) (PEO) in a PEO-PPO-PEO configuration. The ink liquefies below the critical micelle temperature (<10 °C). Based on this phase change behavior, the patterned fugitive ink could be subsequently removed by liquefication at 4 °C under modest vacuum after printing. The space induced by nozzle translation was filled with a photocurable polymer, F127-DA. F127-DA was prepared by chemical modification of Pluronic F127 with diacrylate groups. The printed 3D microvascular networks were interconnected, and the diameter of the lumen could be tailored ranging from 18 to 600 µm. 127 This method allows printing biomaterials simultaneously with a vascular structure. Heterogeneous tissue constructs containing multiple types of cells and complex vascular structure could be fabricated. 128
Cell-laden perfusable vascular conduits have been printed for use in regenerating thick tissues. Using a coaxial deposition system, Zhang et al. developed branched vascular conduits by printing sodium alginate. 129 It has been shown that human umbilical vein smooth muscle cells (HUVSMCs) encapsulated in sodium alginate maintain their functions after printing. Similarly, a branch or tubular structure has been printed without using any template.29,30
The angiogenesis process involves a variety of cell types and chemical stimuli. Studies have been performed to determine whether the controlled release of these factors can be incorporated in 3D bioprinting. A study showed that VEGF can be incorporated by mixing gelatin microparticles (GMPs) with bioinks during printing. 130 Prolonged release of VEGF from GMPs led to a significant increase in scaffold vascularization compared with the fast-release group prepared by mixing VEGF with hydrogels.
Clinical Applications of 3D Bioprinted Tissues and Organs
The creation of highly organized multicellular tissue constructs that resemble the functions and architectures of human organs could revolutionize how medical treatments are delivered. Such tissue constructs can also be used as tissue models for drug screening or validation or toxicity study, or as disease models for pathology study. Many efforts have been made in the past decade to harness the advantages of 3D bioprinting to develop personalized tissue and organs for precision medicine. For instance, Organovo has developed 3D printed human liver tissues that can remain fully functional and stable for up to 28 days131,132 and that could potentially be implanted into patients to replace their damaged liver. 3D printed preclinical kidney tissue has also been attempted. These 3D printed preclinical kidney tissue constructs are similar to human kidney, consisting of an apical layer of polarized primary renal proximal tubule epithelial cells supported by a collagen IV–rich tubulointerstitial interface of primary renal fibroblasts and endothelial cells. 133 The other front is the use of 3D printed tissue models as a training tool to improve resident education and the success rate of surgery. For instance, 3D medical imaging data were used to create 3D printed vascular rings and slings that precisely replicate congenital cardiovascular lesions for educating and training residents of cardiology. 134 Using imaging data collected from CT, MRI, and so forth, and combining them with CAD to create 3D printed tissue constructs for clinical application has been explored. A cervical model has been 3D printed and used as a hemorrhagic model for postgraduate gynecological training. 135 3D printing has increasingly been used to manufacture prostheses and implants due to its ability to fabricate personalized implants that can be customized and tailored to fit the patient’s needs. For instance, the real-time 3D printing of on-demand custom cranioplastic prostheses has recently been demonstrated, and the use of 3D printed cranioplastic prostheses in patients is on the way. 136 The use of 3D printed silicone-embedded prostheses for partial hand amputation has also been recently demonstrated. 137 It should, however, be pointed out that the clinical applications of 3D bioprinted tissue constructs are still in their infancy. Advancement in these ends requires more technology breakthroughs and a paradigm shift from conventional, centralized, and off-the-shelf manufacturing to decentralized and on-demand production of tissues and organs that are better customized and tailored for precision medicine.
Challenges and Future Trends
The 3D bioprinting technique has shown profound impacts on tissue engineering and regenerative medicine. Recent developments in computer science, tissue engineering, and nanotechnology, for example, permit the development of 3D tissue constructs with heterogeneous structures that recapitulate better native tissue and organ architectures. The advances in 3D printing allow for re-creating a 3D microengineered environment that mimics in vivo microenvironments. Native organs and tissues exhibit complex heterogeneous structures containing multiple types of cells. The challenges to manufacture these tissues and organs include two main aspects: bioink (cell or cell aggregates mixed with functional biomaterials) and engineering design. Cells that can reproduce the functions of tissues and organs must be carefully selected. In addition, there is still a pressing need for developing biomaterials that are printable and highly biocompatible. Hydrogels derived from dECMs recapitulate the composition of native tissues and are considered promising biomaterials for printing. The construction of a capillary network (~10 µm in diameter) remains a challenge due in part to the limitations in spatial resolution that can be achieved by existing 3D bioprinters. While 3D printed tissues have been demonstrated, integrated organ printing has not yet been fully established. 79
Finally, a new generation of smart or programmable tissue constructs can be potentially printed. The smart polymers that could change their volume or other properties in response to stimuli such as pH, temperature, or magnetic field can be used in 3D printing to create programmable tissue scaffolds. 138 This response may enhance the interactions between cells and printed constructs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by NSF CBET-0756455, CBET1445387, CBET 1531944, and SUNY Health Now Network of Excellence.