
Abstract
Introduction
Anatomic hemiarthroplasty (aHA) is a treatment option for non-reconstructable constructable multifragment proximal humeral fractures that preserves range of motion. Our study aims to evaluate the radiographic and clinical outcomes of patients who received a modular aHA with anatomical sizing of the tubercle-bearing metaphyseal components.
Materials and Methods
The medical records of thirty-nine consecutive patients were reviewed. Patients were treated at a single institution with aHA as first-line treatment following a non-reconstructable constructable proximal humeral fracture. Tubercle resorption and cranialization of the aHA were analyzed using radiographic controls. Patient clinical function was assessed using the Constant Murley Score (CS).
Results
Twenty-four patients (62%) were available for clinical follow-up, with a mean CS of 54 points after a mean 56-month follow-up period. There was no significant difference in functional outcome on average between patients with healed tubercles (CS = 57) and resorbed tubercles (CS = 51). Radiographic follow-up was available in 33 patients (85%), demonstrating healed tubercles in 33% of the patients. Patients with resorbed tubercles had significant smaller acromio-humeral distances (AHD) than patients with healed tubercles (p = 0.043). A positive correlation was observed between greater AHD and increased constant scores (p = 0.022).
Conclusions
The final patient outcome measures demonstrated a positive correlation with a greater acromio-humeral distance and tubercle healing rates. However, the modular stem design with sizing of the metaphyseal components did not result in superior outcomes when compared with the literature.
Keywords
Background
Anatomical hemi-shoulder-arthroplasty (aHA) is a treatment option utilized in cases of dislocated multi-fragment proximal humeral fractures when reconstruction is technically not feasible, or when there is an increased risk of either secondary humeral head necrosis or secondary displacement after internal fixation.1–3 Depending on the fracture pattern, three criteria play an important role as risk factors for the development of head necrosis: (1) the involvement of the posteromedial metaphysis and its degree of displacement, (2) fractures of the anatomical neck, and (3) fractures of the tuberosities. 4 In addition to the correct anatomical alignment of the humeral shaft, tubercle healing is crucial in determining the patient's clinical outcome. 5
Some authors have advocated a reverse total shoulder arthroplasty (rTSA) as a reasonable alternative due to undesirable previously reported results of aHA. 6
In recent years, numerous studies have attempted to modify the aHA procedure to achieve more optimal tubercle healing, with proposed solutions including refinements of the suture/wire material and threaded straps that affix the tubercles to specifically designed (eg tantalum-coated) prosthesis models.7–12
Kralinger et al evaluated tubercle healing rates using the predecessor model to the aHA analyzed in this study and found that 16.8% of patients had tubercle healing with more than 0.5 cm of displacement, and 37.1% had healing with less than 0.5 cm of displacement. 13
A newer generation of aHA (Global Unite®, DePuy-Synthes, West Chester, PA, USA) utilized at our institution for several years has allowed for modularity and the ability to convert an aHA into an rTSA in the event of revision surgery (eg, due to tubercular resorption) without having to change the shaft. This particular model also has specific proximal metaphyseal joint pieces (porous-coated components; Figure 1) and suture collars for refixation of the tubercles.
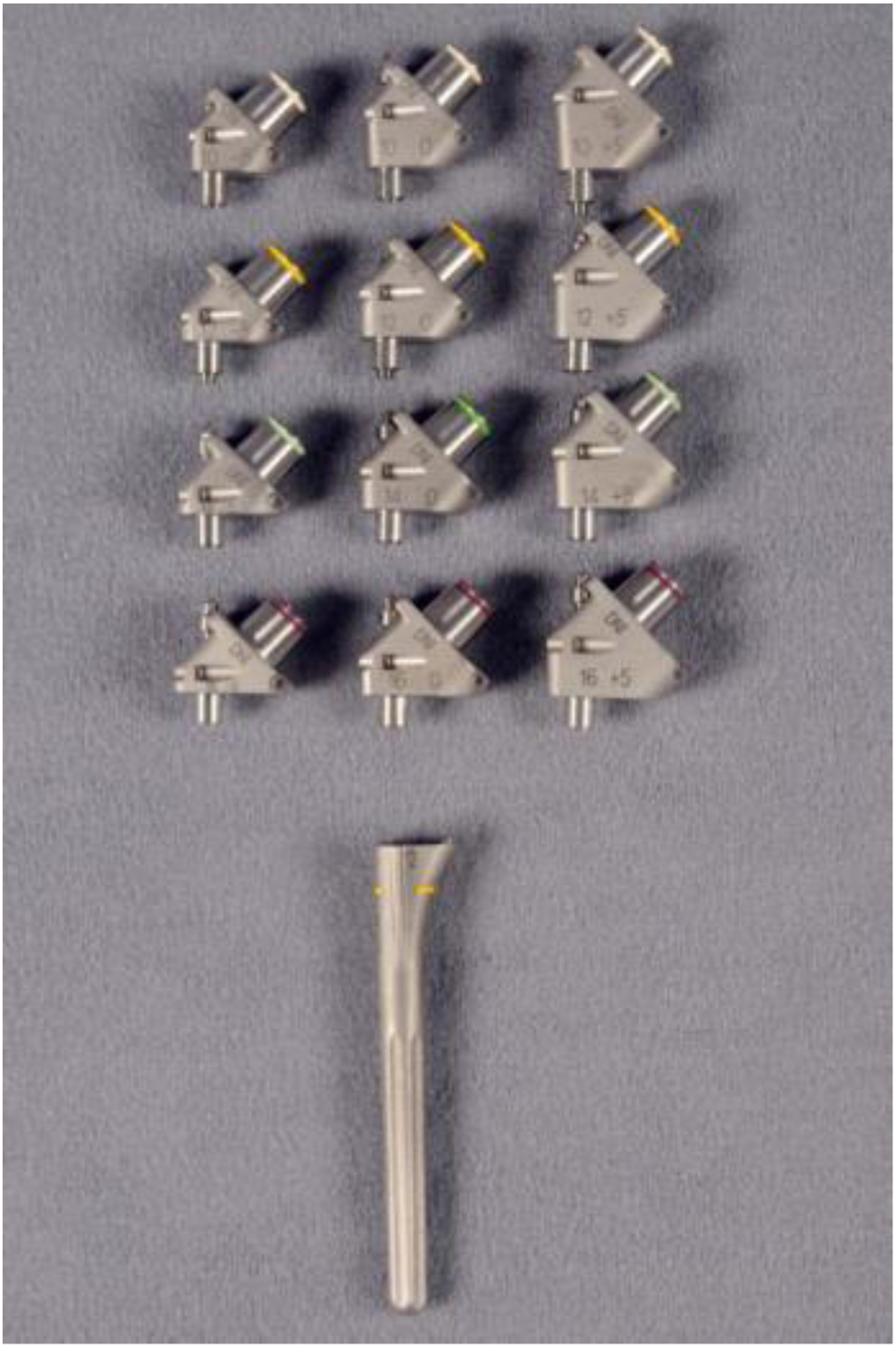
Samples of the metaphyseal components for individual size adjustment(Global Unite® DePuy Synthes, West Chester, PA, USA). The original implants are porous coated.
This grants the surgeon increased flexibility to adapt to each patient's unique anatomical proportions.14,15 While studies on tubercle healing in various prosthesis designs can be found in the literature, to date, there are no results on the healing rates of the tubercles in this particular model with individual metaphyseal size adjustment.
Our study aims to assess the radiographic and clinical outcomes of patients receiving modular aHA with the Global Unite® system.
Methods
All applicable institutional and governmental regulations concerning the ethical use of clinical data were followed during this research. The institutional review board of the University of Bochum (Germany) approved this study (16-5799-BR). Informed consent was obtained from all participants. A retrospective chart analysis was conducted on 39 patients who presented themselves between 2010 and 2016 with isolated, non-reconstructable proximal humeral fractures and underwent aHA surgery at our institution. After IRB-approval was obtained, all patients were contacted for follow-up examination. The inclusion criteria were defined as non-reconstructable proximal humeral fracture as isolated trauma that was treated with an aHA. The exclusion criteria were defined as polytraumatized patients, patients with paretic symptoms of the upper limb, and patients with a secondary diagnosis of septic disease.
Functional and Radiographic Analyses
Patient functional outcomes were measured using the Constant Murley Score (CS). 16 The range of motion and force were measured using a goniometer and a force gauge (Isobex isometric dynamometer, Cursor, Bern, Switzerland). The resorption of the tubercles and the cranialization of the aHA were analyzed radiographically with plain film x-rays. Two senior level surgeons and one radiologist (R1; R2; R3) assessed the images, assigning fracture types according to the classification of Neer and Resch to minimize misdiagnoses regarding the exact fracture patterns, acomio-humeral distances and resorption of tubercles.17,18 Tubercle resorption was analyzed based on the remaining bone mass in the a.p. radiographs. It was assumed that tubercle resorption was present if less than 50% of the bone mass was present at the time of the last radiograph compared to the initial postoperative x-ray (Figure 2).

64-year-old female. (a) Intraoperative image of the trial prosthesis with adapted tubercles; (b) Subsequent postoperative a.p.-image. (c) Resorbed tubercles, approximately the same AHD and centered prosthesis (CS 45 points) after 72 months.
To classify a secondary cranialization of the prosthesis, the acromio-humeral distance (AHD) at follow-up was compared to the immediate postoperative x-ray. A cranial decentering distance between 5 and 7 mm was rated as partial cranialization, and distances ≤ 4 mm were rated as complete cranialization. One surgeon carried out clinical examinations to minimize interobserver errors. A statistical analysis was conducted to determine the impact of patient-specific factors (eg, rheumatoid disease, smoking history, ASA, and BMI) on the resorption rate of the tubercles. Furthermore, the analysis considered the impact of the sizing of the metaphyseal body on tubercle resorption.
Statistical Analysis
All statistical tests were carried out with SPSS (Statistical Package for the Social Sciences, Chicago, IBM, IL, USA). The evaluation was initially conducted with descriptive statistics. Numerical data, means, standard deviations, or medians were calculated depending on the distribution. The Mann-Whitney test was used to determine the presence of any relationship between functional and radiological findings. The Pearson correlation coefficient was calculated to assess the relationship between CS and AHD. Significance was determined for all tests at p < 0.05. Inter- and intra-rater reliability was evaluated using Cohen's Kappa.
Surgical Note
All patients were operated on within the first 48 h after trauma. The surgical technique included either press-fit anchoring of the humeral shaft or cement fixation. In the case of cement fixation, care was taken to ensure the cement did not reach the contact zone of the tubercles to the shaft in order to allow bony healing. Prior to insertion of the prosthetic stem, a trial reduction was carried out with the help of a trial stem. Size adjustments were then made of the modular metaphysis, suture collars/eyelets, and a prosthetic head corresponding to the patient's size. The selection of the “appropriate” metaphyseal component is based on the surgeon's experience of how best to fit the patient's proximal humeral anatomy based on the trial stem. The size of the tubercles to be refixed play an important role. This was assessed both intraoperatively and fluoroscopically. After the original implants were inserted, the tubercles were fixated with tear-resistant, non-absorbable sutures (FiberWire®, Arthrex Naples, USA). First, the greater tubercle was reattached to the prosthesis and the stem using two horizontal threads. This was followed by reattachment of the lesser tubercle, which was positioned on the prosthesis and stem using two additional horizontal threads that also encompassed the greater tubercle. Finally, vertical threads were passed through the shaft, pulled through the eyelets of the collar, and knotted to ensure a stable connection to the prosthesis and to the shaft.
Postoperative Management
In the initial two-week period, the arm is immobilized in a shoulder orthosis in order to stabilize the shoulder and facilitate healing. Patients are instructed to commence passive movement exercises under the guidance of a physiotherapist. These exercises include gentle pendulum exercises and passive lifting of the arm, but without active muscle contractions, and are designed to maintain mobility without placing undue strain on the shoulder. The shoulder orthosis is still used, but can be removed for the exercises and short intervals during the day. Pain management involves the regular administration of pain medication and the application of ice packs to reduce swelling. From the sixth week, active range of motion exercises are introduced, but without weight bearing on the shoulder. Patients start with isometric strengthening exercises, where the muscles are tensed without any movement in the joint. These exercises facilitate the strengthening of the muscles surrounding the shoulder joint, thereby improving stability. Physiotherapy is intensified in order to support the full mobility and function of the shoulder.
Results
A total of 39 patients were treated with aHA (Global Unite® DePuy Synthes, West Chester, PA, USA) between 2010 and 2016 due to a non-reconstructable proximal humeral fracture (29 female, 10 male). The average age at surgery was 63 years. Five (13%) of the initial 39 patients were converted to an rTSA since their initial procedure. In four of five cases, revision surgery was performed due to secondary cranialization of the prosthesis, resulting in poor functional outcomes. In these cases, patients requested re-operation after 7, 8, 25, and 49 months. In one case (3%), a periprosthetic infection with positive pathogen detection (Staphylococcus aureus) led to a staged revision surgery after 13 months. Six patients were lost to follow-up, and four patients were unwilling to participate in the study. A total of 24 patients (62%) were available for clinical follow-up, with a mean follow-up period of 56 months (±15.05; range 26-80 months). The distribution of patients included in the clinical and radiological analysis is illustrated in Figure 3.

The following flowchart illustrates the distribution of patients undergoing clinical and radiological follow-up examinations.
The Results Related to the Functional Outcome
The 24 patients available for clinical follow-up examination reached an average CS of 54 points (±14.86; range 29-79 p.) at an average follow-up of 56 months (±15.05; range 26-80 months). Patients with healed tubercles achieved an average CS of 57 p. (±18.34; range 29-79; p = 0.565), while patients who had resorbed tubercles reached an average CS of 51 p. (±14.58; range = 29-77 p; p = 0.268). Greater measurements of acromio-humeral distances demonstrated a positive correlation with increased constant scores (p = 0.022; Figure 4).

Correlation of the constant score (x-axis) the acromiohumeral distance at last follow-up (y-axis), p = 0022.
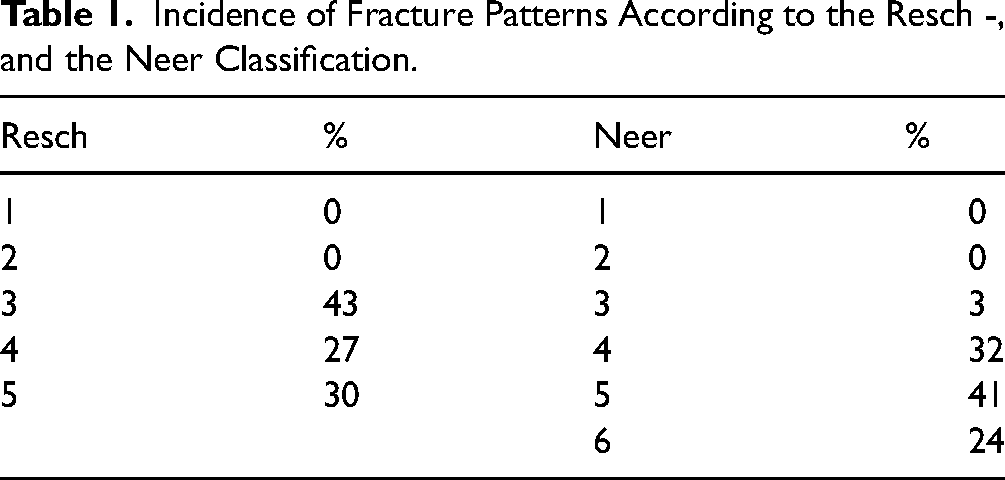
With regard to interrater and intrarater error, Cohen's kappa coefficients demonstrated a moderate agreement between R1 and R2, and R1 and R3, while a substantial agreement was achieved between R2 and R3 (R1:R2, κ = 0.50 (SE 0.05); R1:R3, κ = 0.60 (SE 0.04); R2:R3, κ = 0.65 (SE 0.04)). The Neer and Resch classification patterns did not demonstrate a correlation with the eventual functional outcome (Neer: p = 0.908; Resch: p = 0.123) or with tubercle healing (Neer: p = 0.203; Resch: p = 0.194). The exact distributions of the fracture patterns, according to both classifications, are provided in Table 1.
Incidence of Fracture Patterns According to the Resch -, and the Neer Classification.
Results of Patient-Specific Factors and Metaphyseal Body Sizing and Tubercle Resorption
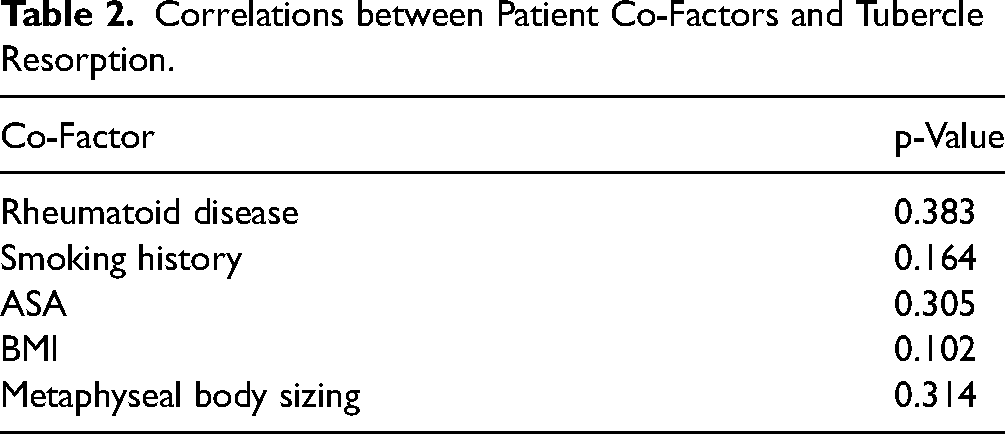
Only two of 39 patients had a history of rheumatoid arthritis, according to their medical records. The mean BMI of the 39 patients included was 28.55 (range 20.7 to 40.4). The results did not yield any significant findings regarding the resorption of the tubercles and the aforementioned patient-specific co-factors, nor metaphyseal body sizing. The exact p-values are shown in Table 2.
Correlations between Patient Co-Factors and Tubercle Resorption.
Results of Tubercle Healing and AHD Measurements
Six patients were lost to follow-up, resulting in the availability of x-ray images for radiological assessment in 33 patients (85%). Converted patients were nevertheless taken into account with regard to the success rate. Healed tubercles were found in 11 of 33 patients (33%), while resorbed or largely resorbed tubercles were observed in 22 of 33 patients (66%). The average AHD was 6.81 mm (± 4.4 mm). A complete cranialization of the aHA was found in 9 patients (27%), with an average AHD of 2.22 mm (± 1.30 mm; range = 1-4 mm). Twelve patients (36%) had a partial cranialization, with an average AHD of 6.08 mm (± 1.5 mm; range = 5-10 mm). Twelve patients (36%) showed no cranialization. Patients with resorbed tubercles had a significantly smaller AHD than patients with healed tubercles (p = 0.043). Figure 5 shows the x-rays of a 54-year-old patient with healed tubercles and a satisfactory functional outcome (CS 74).

54-year-old male. (a) Direct postoperative image with adapted tubercles; (b) Subsequent postoperative a.p.-image after 6 months. (c) Subsequent x-ray after 2.5 years with healed tubercles and centricity of the prosthesis (CS 74).
Discussion
Tubercle Healing Rates and Functional Outcomes
Our study revealed a tubercle healing rate of 33% and an average Constant Score (CS) of 54 points following aHA. This functional outcome is comparable to the results found by Boileau et al, who reported a CS of 56 points following an average follow-up of 27 months in patients with aHA after trauma. 5
Singh et al examined critical variables for tubercle healing after aHA in 84 patients with 4-part humeral head fractures one year postoperatively. They found that tubercle healing occurred in 44% of patients, while tubercles did not heal in 56% of the patients. Notably, patient age, smoking status, bone density, or the presence of diabetes did not significantly correlate with tubercle healing rates, as none of the patient-specific co-factors analyzed in our data exhibited a correlation. It is noteworthy that male patients exhibited a higher success rate, and that a sufficient distance between the cement and the tubercles was found to be a significant factor for successful healing of the tubercles. The clinical follow-up and functional outcome data were not presented. 19 A longitudinal study by Hackett et al revealed that 73% of patients who underwent aHA experienced displacement or malunion of the tubercles. A number of factors have been identified as contributing to the high failure rates associated with aHA. Boileau et al identified detachment, migration, or incorrect positioning of the tubercles in 50% of their patients, which correlated with poor clinical outcomes, including stiffness, weakness, and persistent shoulder pain.5,20
Kralinger et al concluded that the patient's age and the type of prosthesis utilized appear to influence the healing rates of the tubercles as well as the patient's functional outcome. The predecessor model (DePuy Global Advantage Shoulder Arthroplasty System, DePuy, J & J, Warsaw, USA) yielded a tubercle healing rate of 29%, which is comparable to the healing rates of the successor model examined in our study (33%). 13
In a comparative study, Li et al examined the outcomes of a conventional aHA and a trabecular aHA (trabecular metal™ shoulder prosthesis). The authors observed a reduced incidence of tubercle-associated complications with the trabecular metal^(TM)-coated prosthesis (6.1% vs 25.7%), so that the focus was once again on the nature of the metaphysical component. 21 Fucentese et al conducted a study investigating the use of a prosthesis with a large metaphyseal volume in 30 consecutive patients. A total of 12 cases were identified in which the greater tubercle exhibited resorption, while five cases demonstrated displacement. In contrast, 23 tubercles exhibited healing in situ. 11
Fracture Patterns and the Functional Result
Our analysis revealed that there was no detectable influence of fracture patterns on the functional outcome following aHA as indicated by the statistical analysis by Resch (p = 0.123) and Neer-fracture patterns (p = 0.908). A study conducted by Agarwal et al focused on a cohort of 24 individuals who underwent treatment utilizing the earlier version of the shoulder prosthesis that was employed in the patient population of our investigation, specifically the DePuy Global Advantage Shoulder Arthroplasty System manufactured by DePuy (Warsaw, USA). The findings of Agarwal et al demonstrated that patients afflicted by a proximal humeral head fracture classified as 3 to 4-part fractures experienced an average Constant Score of 56 points. It is noteworthy that the researchers in their investigation did not delve into the phenomenon of tubercle resorption but instead directed their attention towards the post-operative proximal migration of the reinserted tubercles. This particular occurrence was documented in a subset of 4 out of the total of 24 patients included in the study. 22
The Role of the Acromio-Humeral Distance in the Functional Outcome
The outcomes we observed demonstrated a similar pattern as documented by Kralinger et al, particularly when considering the notable associations between the CS and AHD (p = 0.039), as well as the AHD and tubercle resorption (p = 0.043). Within a multicenter investigation conducted by Kralinger et al, it was found that 46.1% of participants experienced either resorption or dislocation of tubercles following an average monitoring period of 29 months subsequent to the insertion of an aHA due to trauma. Additionally, 16.8% of individuals exhibited tubercle healing with a displacement exceeding 0.5 cm, while 37.1% displayed healing with a displacement of less than 0.5 cm. Patients with resorbed tubercles attained notably lower CS scores (mean 49) in comparison to those with healed but subsequently dislocated tubercles (CS 53). Their research was deemed to be lacking statistical power, thus preventing the formulation of significant conclusions. 13
Limitations of the Present Study
The main limitations of the present study are the retrospective design and the lack of a control group. Additional factors may significantly influence tubercle healing, such as tubercle quality, tubercle size (multifragmented or single), and the type of fixation technique used. Because modularity makes intuitive sense with respect to individual metaphyseal size adjustments, future prospective randomized studies with larger patient populations should be performed before definitive conclusions can be drawn regarding the efficacy of this surgical technique.
Conclusion
The final patient outcome measures demonstrated a positive correlation with a greater acromio-humeral distance and tubercle healing rates. Despite the individual size adjustments of the metaphyseal tubercle-bearing process of the prosthesis, the resorption rates of the tubercles remained high, with comparable clinical outcomes to previous models. The option to convert to an rTSA while leaving the stem in place represents a significant advantage.
Footnotes
Acknowledgements
Not applicable.
Availability of Data and Materials
The dataset used during the current study is available from the corresponding author on reasonable request.
Code Availability
Not applicable.
Consent to Participate
Informed consent has been obtained. All study participants have given a written declaration of consent to participate and agreed to the publication of the data obtained.
Consent for Publication
All authors and study participants have given a written declaration of consent for publication of the data obtained in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
We certify that all applicable institutional and governmental regulations concerning the ethical use of clinical data were followed during the course of this research according to the Declaration of Helsinki. This study (16-5799-BR) was approved by the institutional review board at the University of Bochum (Germany) on 07/15/2016.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Trial Registration
This study (16-5799-BR) was approved by the institutional review board at the University of Bochum (Germany) on 07/15/2016.