
Abstract
Purpose:
To investigate the influence of greater tuberosity healing on the functional outcomes of reverse shoulder arthroplasty (RSA) for the treatment of acute complex proximal humeral fractures (PHFs), and to investigate the influence of patient- and surgery-related factors in the healing of the greater tuberosity.
Methods:
Retrospective study including 41 consecutive PHFs treated using RSA with minimum 2-year follow-up. In all the cases, tuberosities were reattached with a standardized technique. All the patients were assessed at the last follow-up with constant score. Body mass index, surgery delay, comorbidities, polyethylene size, glenosphere size, overhanging of glenosphere, and scapular notch were recorded, and their influence in final constant score and in greater tuberosity healing was analyzed.
Results:
Mean final constant score was of 60.7 points (standard deviation (SD) = 9.9). Greater tuberosity healed in proper position in 68% of the cases. There were no significant differences in constant score between patients with (mean = 61; SD = 9.5) and without (mean = 61; SD = 11.3) the healing of greater tuberosity. All patients scored above 90° in forward elevation. Scapular notch was reported in 14.6% of the cases. Age significantly affected the constant score (p = 0.008). Comorbidities significantly interfered with greater tuberosity healing (p = 0.03). There was one reoperation after dislocation.
Conclusion:
In spite of expecting good functional outcome with low complication rate after RSA for acute PHFs, the influence of greater tuberosity healing on shoulder function could not be demonstrated. The presence of comorbidities, but not age or gender, negatively influenced the healing of the greater tuberosity.
Introduction
Reverse shoulder arthroplasty (RSA) was originally designed to treat osteoarthritis related to rotator cuff deficiency or massive cuff tears. However, its indications have now spread over time to include the treatment of cuff-deficient shoulders without osteoarthritic changes, acute fractures, fracture sequelae, tumor surgery, and revision surgery. 1 –3
Treatment of complex proximal humeral fractures (PHFs) in elderly patients is still controversial. Recently, there has been a tendency to treat PHFs using RSA instead of hemiarthroplasty (HA), especially among young shoulder surgeons. 1 Results obtained with RSA seem to be superior and more predictable than those obtained with HA in these complex fractures. 4 –11 Functional outcomes in HAs are more unpredictable and depend on the healing capacity of the tuberosities, which is usually diminished in such osteoporotic and comminuted fractures. 12 –14 However, better results obtained with RSA may not provide a clear benefit for patients in daily life, 6 and complication rate can be lower in patients treated with HA. 15,16
Because the RSA system was thought to work without rotator cuff, surgeons did not routinely reattach tuberosities in the early reports of RSA use for acute PHFs. 17 While supraspinatus is not necessary in the RSA, the absence of infraspinatus and teres minor implies lack of active external rotation. For this reason, there is nowadays a tendency for reattachment of tuberosities when using RSA for acute PHFs even though there is still some controversy about the benefits of tuberosity healing on the clinical outcomes. 5 –8,11,18
On the other hand, a strong influence of age, gender, and comorbidities in greater tuberosity healing has been found when hemiartroplasties are used for the treatment of acute PHFs. 13,14,19 Elderly patients (over 75 years old), females, and the presence of three or more comorbidities significantly impair tuberosity healing. However, the influence of these factors in using RSA needs further research.
The main purpose of this study was to investigate the influence of greater tuberosity healing on the functional outcomes of RSA for the treatment of acute complex PHFs. A secondary purpose was to investigate the influence of patient- and surgery-related (surgery delay, overhanging of the glenosphere, polyethylene size, and glenosphere size) factors on the healing of the greater tuberosity.
Materials and methods
A retrospective study was conducted with prospective data collection, including all consecutive PHFs treated with an RSA, from January 2010 to December 2012. All surgeries were performed by the same surgeon (computerized tomography (CT)) and using the same implant (Delta Xtend™; DePuy, Warsaw, Indiana, USA). Patients can participate in the study if they meet the following criteria: (1) acute complex PHF (three- or four-part fracture with or without dislocation) operated within the first 3 weeks of the initial trauma, (2) not suitable for open reduction internal fixation (ORIF) based on surgeon’s decision, (3) no previous surgery on the shoulder affected, (4) clinical and radiological examinations with a minimum follow-up of 2 years, and (5) willing to participate in the study. Patients with incomplete files were excluded.
There were 47 PHFs treated with an RSA during this period. Two patients were exclused because surgery was done after 3 weeks of trauma and another two because of incomplete files. Two patients were lost at the last follow-up because of impairment in their general health and mobility, leaving 41 patients with complete follow-up. All fractures included were analyzed and classified before surgery after reviewing plain radiographs (anterior–posterior and axial views) and CT examinations. Following Neer’s 20 classification system, fractures were classified into 7 three3-part greater tuberosity and 34 four-part fractures. The mean (range) follow-up was 29 (24–37) months.
All surgeries were done through the anterosuperior approach. After excision of the humeral head, the glenoid was prepared and the metaglene placed flush with the inferior glenoid rim. Glenosphere size was decided at surgeon’s preference. The humeral component was always cemented and placed in neutral position (0° of retroversion). In all cases, tuberosity reattachment was performed with a suture configuration that included two horizontal sutures and two vertical cerclages (from diaphysis to greater tuberosity and from diaphysis to lesser tuberosity) with a heavy nonabsorbable braided suture (No. 5 Ethibond; Ethicon, Somerville, New Jersey, USA). In all patients, supraspinatus excision was done before tuberosity reattachment. After surgery, the arm was placed in a sling for 3 weeks, followed by gentle passive motion was initiated. Due to the advanced age of the patients, a home-based rehabilitation program was instituted, starting with passive forward elevation exercises followed by passive internal rotation exercises once the forward elevation reached 120°. Lastly, external rotation exercises were implemented.
Functional assessment was done with an annual constant score. The last score was used for the statistical analysis. 21 Postoperative radiological examinations were performed under fluoroscopic control to assure true anterior–posterior view with the arm in neutral position and outlet view. These radiological examinations were performed immediately after surgery and at 1, 6, and 12 months. The patients were examined annually afterward. Greater tuberosity was considered to heal in anatomic position when (1) visible in the anterior–posterior view with the arm in neutral position, (2) the top of the greater tuberosity at the level of the polyethylene of the humeral component, or (3) the top of the greater tuberosity at the level of the epiphyseal part of the prostheses (Figure 1). The greater tuberosity was considered to be malpositioned or posteriorly migrated if not seen on the neutral anterior–posterior view (Figure 2). Scapular notch according to Sirveaux et al. 2 classification and overhanging of the glenosphere was viewed on the true anterior–posterior view too.
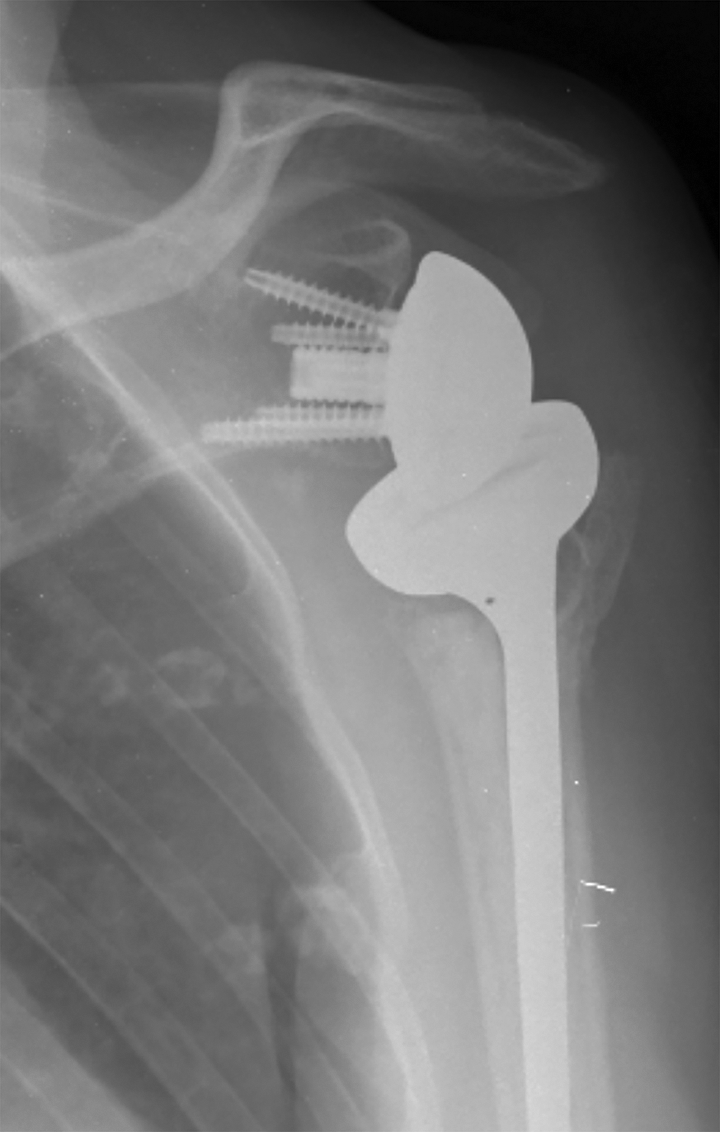
Anterior–posterior view showing greater tuberosity healed in anatomical position.

Anterior–posterior view showing the absence of the greater tuberosity.
Age, gender, body mass index (BMI), surgery delay, overhanging of the glenosphere, polyethylene size, glenosphere size, and comorbidities (recorded through the American Society of Anesthesiologist (ASA) system) were analyzed according to constant score and greater tuberosity healing.
Statistical analysis
Descriptive statistics were used to summarize all data. Quantitative variables were reported with mean and standard deviation, while categorical variables with frequencies and percentage. The correlation between BMI, surgery delay, age, and overhanging of the glenosphere with constant score was assessed with Spearman’s rho correlation coefficient. Differences in constant score among categorical variables were compared with Mann–Whitney U test. Finally, χ 2 and Fisher exact test (as appropriate) were used to compare categorical variables. p Values of less than 0.05 were considered as statistically significant. All analyses were performed with SPSS 18.0 (IBM Inc., Armonk, New York, US). The study was approved by the ethical committee with number 2014/6001/I (CEIC-Parc de Salut Mar).
Results
Epidemiological data
There were 31 females and 10 males with a mean (range; standard deviation (SD)) age of 77.9 (62–90; 6.3) years, mean BMI (range; SD) of 28.1 (23.1–38.4; 3.9), mean (range; SD) surgery delay of 11.6 (0–20; 6.4) days, and mean (range; SD) overhanging of the glenosphere of 6.7 (0–12.8; 2.8) mm.
The +3, +6, and +9 polyethylenes were used in 21, 16, and 4 cases, respectively. Twelve patients received glenosphere of size 38, while 29 patients received glenosphere of size 42. Three patients were assigned to ASA I and ASA IV each, 21 to ASA II, and 14 to ASA III.
Functional results
Mean (SD) absolute constant score at a mean (range) follow-up of 29 (24–57) months was 60.7 (9.9) points, mean (SD) pain was 12.6 (2.4) points, mean (SD) activities of daily living was 16.8 (2.5) points, mean (SD) forward elevation was 6.6 (1.3) points, mean (SD) abduction was 6.3 (1.3) points, mean (SD) lateral rotation was 5.3 (2.1) points, mean (SD) internal rotation was 5.4 (2.2) points, and mean (SD) strength was 6.7 (2.8) points.
Regarding pain, the majority of the patients (83%) scored over 10 in a 15-item scale, where 0 means severe pain and 15 no pain. Regarding forward elevation, all the patients scored over 90° (6 or more in the constant score) except one patient who scored between 61° and 90° (4 in constant score). Lateral rotation of 4 or less points of the constant score was achieved by 33% patients, while 67% at least reached the top of the head (constant score of 6 or more points). Internal rotation over the level of the lumbosacral junction was achieved only by 50% patients.
Constant score was significantly affected by age (elderly patients scored significantly less than younger patients) but gender, BMI, surgery delay, glenosphere overhanging, polyethylene size, glenosphere size, comorbidities, and healing of the greater tuberosity did not significantly affect the final constant score (Table 1).
Constant score according to age, gender, BMI, surgery delay, glenosphere overhanging, glenosphere size, comorbidities, and greater tuberosity healing.

SD: standard deviation; BMI: body mass index.
Healing of the greater tuberosity
The greater tuberosity healed in anatomic position in 28 (68%) patients and was considered to be in nonanatomic position in 13 (32%) patients. Further analysis (with computed tomography) revealed that among the 13 patients with nonanatomic position of the greater tuberosity, in 9 the greater tuberosity healed in a posterior position not visible in the anterior–posterior neutral plain radiograph view (Figure 3(a) to (c)), and in 4 patients greater tuberosity appeared to be resorbed.

(a) The absence of the greater tuberosity in anterior–posterior view, (b) greater tuberosity visible on the back in outlet view, and (c) CT scan assessment of the greater tuberosity healed posteriorly. CT: computerized tomography.
Age and gender did not significantly affect greater tuberosity healing (p = 0.28 and p = 0.37, respectively). Glenosphere size (p = 1.00), polyethylene size (p = 0.26), and overhanging of the glenosphere (p = 0.32) did not significantly affect greater tuberosity healing either. Surgery delay (evaluated as patients operated on before versus after 15 days) did not significantly affect greater tuberosity healing (p = 0.22). BMI (evaluated as patients over 25 compared to those below 25) did not significantly affect greater tuberosity healing (p = 0.055). Comorbidities significantly influenced greater tuberosity healing in patients of ASA I category compared to patients of ASA IV category (p = 0.03; Table 2).
Greater tuberosity healing according to age, gender, BMI, surgery delay, glenosphere overhanging, glenosphere size, polyethylene size, and comorbidities.

BMI: body mass index.
Complications
Notching was present in the 14.6% of the cases (two grade 1 and four grade 5) and inferior osteophyte in 12% of cases. There was one case of dislocation 2 weeks after surgery, which required further surgery in exchange for a 42-mm glenosphere and 42-mm (+ 6) polyethylene and tuberosities reattachment. Dislocation did not affect the final constant score, which was 74. Transient arm paresthesia was noted in six patients.
Discussion
Treatment of complex PHFs is still controversial but RSA has been increasingly used as an alternative to HA in the recent years. 1 Functional outcomes of PHFs treated with RSA seem to be more predictable compared to those obtained with HAs, as it has also been shown in this study, where all the patients included scored above 90° of forward elevation. It is still not clear whether tuberosity healing has any effect on the overall functional score, but the results obtained in the present study do not evidence a significant influence of greater tuberosity healing in functional outcome.
Treatment of complex PHFs with RSA results in better predictability of achieving good functional outcomes, especially forward elevation, when compared to HA as it has been shown in several studies. 5 –11 Almost all the patients reach 90° of forward elevation in RSA, while this result is more unpredictable with the use of HA. Lateral rotation is less likely to be restored with the use of RSA. Ferrel et al. in a systematic review concluded that RSA did better in forward elevation when compared to HA (RSA: 118° and HA: 108º) but lateral rotation was decreased in RSA (RSA: 20° and HA: 30°). 15 Mata-Fink et al. in another systematic review found the same results with RSA doing better in forward elevation compared to HA but with worst results in lateral rotation. 9 Cuff et al. in a comparison study of RSA and HA found better outcomes in forward elevation using RSA but failed to find significant differences in both internal and lateral rotations. 18 On the opposite, Sebastiá-Forcada et al. and Chalmers et al. found better functional outcome in RSA for both forward elevation and lateral rotation. 11,22 In the present study, all the patients reached at least 90° of forward elevation, this being in concordance with previous studies. Lateral rotation was severely impaired in 12 patients that did not even reach the top of the head. In five of these patients the greater tuberosity did not heal, while in seven patients, the greater tuberosity was judged as healed. In 17 patients, internal rotation was considered to be severely impaired with less than 4 points in the constant score (reaching just the buttock). This result is in concordance with the literature published, since internal rotation is not restored and even decreased after an RSA in cuff-deficient shoulders. 2,3,23
It is still controversial whether healing of the greater tuberosity in RSA significantly affects functional outcome. Cazeneuve and Cristofari in an early report found limited results and reduction in the constant score at follow-up in a group of patients with tuberosity excision. 17 Sebastia-Forcada et al. in a prospective randomized study did not find differences in function between healed and nonhealed tuberosities in the RSA group. 11 Bufquin et al. failed to find significantly better lateral rotation in patients with healed greater tuberosity compared to those who did not. 5 Lenarz et al. also did not find that malunion of the tuberosities had an effect in functional outcomes. 8 On the opposite, Cuff and Pupello 18 concluded that function was not affected by healing of the tuberosities except for lateral rotation, and Gallinet et al. 7 and Anakwenze et al. 24 found significant differences in the range of motion comparing patients with repaired and nonrepaired tuberosities. In the present study, patients did not significantly differ in functional outcome depending on the healing of the tuberosities, not only in the overall constant score but also in any of the different items of the constant score. In all the patients, excision of the supraspinatus and reattachment of the tuberosities were intended, obtaining a 68% healing rate. Further analysis of the 13 patients in which tuberosities did not anatomically heal revealed that in 9 patients the greater tuberosity healed in a nonanatomical posterior position as assessed with the CT scan, suggesting that in RSA a nonanatomically posterior healing of the greater tuberosity may result in acceptable function even for lateral rotation. In contrast, HAs need anatomical healing of the greater tuberosity to result in acceptable function both in forward elevation and in lateral rotation. 14 Predictive factors of tuberosity healing in HAs are age, gender, and comorbidities. 13,19 Being female and/or over 75 years old and/or with three or more comorbidities results in a significant reduction in tuberosity healing. Since the vast majority of complex PHFs occur in elderly females, a low rate of healing of the tuberosity is expected when using HA. Healing of the tuberosity is independent of gender and age in RSA, meaning that it can be safely used in the vast majority of fractures that commonly affect elderly females. Comorbidities significantly impair tuberosity healing in both HAs and RSA. Therefore, surgery must be indicates with caution in such frail patients, with limited result expectation. Glenosphere size, polyethylene size, and overhanging of the glenosphere did not show an influence in greater tuberosity healing and its use should be considered because of other biomechanical reasons. Surgery delay and BMI did not influence greater tuberosity healing. Despite not demonstrating that greater tuberosity healing was associated with better functional outcomes, it is the authors’ preference to reattach the tuberosity to try to fix the fracture as close as possible to the patient’s normal anatomy.
Scapular notch rate in PHFs is lower than that reported in RSA for cuff-deficient shoulders. 2,3,23 Lenarz et al. reported 3% of scapular notch development in a retrospective study of 30 patients. 8 Ross et al. also reported a low scapular notch rate of 13.7% (4 out of 29 shoulders) belonging all cases to grade 1. 10 Chalmers et al. reported no scapular notch development in a prospective study of 9 shoulders. 22 Cuff and Pupello also reported no scapular notch development in a series of 27 patients. 18 In the present study, scapular notch was present in 14.6% cases. Further studies are needed to clarify the reasons for the lower rate of scapular notch reported in RSA for the treatment of acute PHFs.
Limitations of the study include its retrospective nature and the use of a nonvalidated scale to determine proper healing of the greater tuberosity. Only two patients were lost at the last follow-up. The small number of patients included also limits the strength of the results obtained in the analysis of the factors influencing greater tuberosity healing. Among strengths, all the patients were operated by the same surgeon with a standardized technique and used the same implant design.
Conclusions
In conclusion, RSA for acute complex PHFs provides a predictable functional outcome, with all the patients reaching at least 90° of forward elevation. However, the influence of greater tuberosity healing on the functional outcomes remains controversial. The presence of more comorbidities, but not age or gender, negatively influenced the healing of the greater tuberosity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.