
Abstract
Background
Radiocapitellar arthroplasty fills a treatment void for young patients who experience isolated capitellar fractures or radiocapitellar osteoarthritis who are not candidates for total elbow arthroplasty. The outcomes of this procedure are sparsely reported. We designed a meta-analysis to determine the utility of radiocapitellar arthroplasty with respect to functional and patient reported outcomes.
Methods
The PubMed database was searched for relevant studies. Only studies published in English language that assessed patient reported outcomes following radiocapitellar arthroplasty were included in this study. Reporting followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses for 2020.
Results
The initial review yielded 562 studies that met the criteria. After excluding duplications and confounding factors, eight case series were identified for review. Of the eight studies, seven were eligible for inclusion in the meta-analysis for Mayo Elbow Performance Score, flexion-extension arc, and pronation–supination arc. The pooled standard mean difference was found to be statistically significant between pre-operative and post-operative outcomes for Mayo Elbow Performance Score (SMD = 3.04, 95% CI [2.40, 3.67]), flexion-extension arc (SMD = 1.28, 95% CI [0.73, 1.83]), and pronation–supination arc (SMD = 0.81, 95% CI [0.43, 1.18]). Cochran's Q-test and I2 statistics indicated statistically significant heterogeneity for Mayo Elbow Performance Score (p = .04, I2 = 54%) and flexion-extension arc (p < .01, I2 = 67%).
Conclusions
Patients undergoing radiocapitellar arthroplasty showed statistically significant improvements in flexion-extension arc, pronation–supination arc, and Mayo Elbow Performance Scores compared to pre-operative measures.
Introduction
Osteoarthritis (OA) of the elbow joint has been historically underreported. Pooley et al. reported that a considerable proportion of patients with elbow pain in the 1980s were diagnosed with rheumatoid arthritis. 1 It had previously been well accepted that primary elbow OA was uncommon 2 and therefore patients, who presented with elbow pain and absent radiographic findings, were often diagnosed with lateral epicondylitis. As surgical management improved and arthroscopy was adapted, it became clear that primary OA of the elbow joint, and more specifically the radiocapitellar (RC) joint, was much more common than previously reported.1,3–8 Kachooei et al. performed a retrospective review of 887 patients and identified 54 isolated radial head fractures treated nonoperatively. Of these, they reported a 7.5% incidence of radiocapitellar osteoarthritis (RC OA) diagnosed by standard radiographs. 9 In addition, Rajeev et al. reported that patients who commonly presented with elbow pain had normal radiographic findings, yet arthroscopic evaluation often revealed degenerative changes isolated to the lateral compartment of the elbow. 8 These findings suggest that standard radiographs may underdiagnose RC OA, therefore affording a potential domain for improvement.
RC OA is an inflammatory and/or degenerative condition of the lateral elbow joint that is associated with traumatic injury or wear and tear. Surgical management of isolated RC OA was difficult, specifically in the younger patient population, as total elbow arthroplasty (TEA) was the only definitive option. As a result of the misunderstood prevalence of isolated RC OA, radial head replacement was often considered for symptomatic elbow pain 10 yet, neglected capitellar chondromalacia continued to be symptomatic. Another treatment option, anconeus interposition, was first described by Morrey and Schneeberger in the early 2000s. 11 In this procedure, the anconeus muscle is rotated into the radiocapitellar and/or proximal radioulnar joint 11 providing a soft tissue barrier. 12 Additionally, Morrey et al. described increased elbow stability when the anconeus is routed underneath the lateral collateral ligament. 11 Baghdadi et al. reported improvements in pain and upper extremity function at a mean 10-year follow-up following anconeus interposing. However, postoperative complications were found to be 7% and progressive OA was noted in 17% of the cohort. 12 In attempts to minimize continued patient suffering, alternative surgical management techniques were sought throughout the early 2000s.
Radiocapitellar arthroplasty (RCA) was introduced in 2005 with the addition of the lateral resurfacing elbow (LRE). 7 Soon after the introduction of the LRE, a second implant called the Uni-elbow Radio Capitellum System was introduced and was available for clinical use until 2017 when Stryker reviewed data that suggested suboptimal performance and increased revision rate compared to other proximal radial head devices13,14 (Figure 1). The advent of RCA filled a gap in surgical management for young patients who had experienced capitellar fractures or isolated lateral compartment primary, rheumatoid, or post-traumatic OA. Ideally, patients could expect improved motion, stability, and function with less pain following RCA. Sabo et al. reported physiologic kinematics following RCA when the MCL remained intact. 16 Few studies confirmed these outcomes following RCA. The purpose of this study was to identify the benefits of RCA through meta-analysis.

The lateral resurfacing elbow (LRE) (A) and uni-elbow radio capitellum system (B). 15
Materials and Methods
The PubMed database was searched for terms associated with RCA including “radiocapitellar reconstruction,” “radiocapitellar arthroplasty,” “radiocapitellar replacement,” “lateral resurfacing elbow,” “uni-elbow,” and “radiocapitellar hemiarthroplasty.” Due to the manual nature, and presumed limited number of published RCA studies, only one database was queried. One combination search of “radial head arthroplasty and mayo” was included to capture patients who were treated with isolated radial head arthroplasty and were followed with Mayo Elbow Performance Score (MEPS). We defined RCA as an isolated arthroplasty of the radiocapitellar joint including prosthetic implantation. Reports were included in this study if pre-operative and post-operative MEPS were recorded. Studies were excluded if they were published solely in non-English languages. Additionally, studies were excluded if isolated radial head arthroplasty, TEA, or anconeus interposition was performed. Reports that included an abstract only were excluded.
Systematic Review Registration
A PROSPERO registration completed 08/23/2022 and approved on 09/07/2022 can be found with registration number CRD42022353461.
Systematic Review Process
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram is displayed in Figure 2. 17 All original searches were performed by the primary author (E.P.S.) to minimize the risk of reporting bias. The original searches were performed September 7, 2022 to September 10, 2022 and yielded 562 articles. Of the 562 articles, 205 were excluded based on duplication. The remaining articles were collaboratively screened by five of the reviewers and 275 were excluded based on failure to meet inclusion criteria. The remaining 84 articles were retrieved through Carilion Clinic Institute of Orthopaedics and Neurosciences. All 84 articles were thoroughly assessed for eligibility by two reviewers (E.P.S., D.T.H.). Of these 84, additional articles satisfied exclusion criterion for the following reasons: 42 for isolated radial head arthroplasty, 2 for TEA, 1 for isolated collateral ligament reconstruction, 16 for lack of patient reported outcomes, 9 for reconstruction without prosthesis, 4 for anconeus interposition arthroplasty, and 3 for other forms of elbow reconstruction. The remaining 7 studies were included in this review.

The PRISMA 2020 flow diagram of systematic review process and study selection including search terms.
During the above review process, one article was identified through citation tracing. This article was not published on PubMed or other large databases. Due to the sparsity of data on RCA, the primary author (E.P.S) included the data from Pooley et al. in this review.
Level of Evidence
Each study was assigned a level of evidence based on the 5-tier Oxford Center for Evidence-Based Medicine Level of Evidence for orthopedic literature. Table 1 reflects the grading system used. 18
Oxford Centre for Evidence-Based Medicine Levels of Evidence.

RCT, randomized control trial.
Extraction of Data
Eight articles were included, seven of which were identified via PubMed, and one identified through citation tracking in the originally identified articles (Table 2). All articles included in the review were identified as level IV. The authors, sample demographics, study design, outcome metrics (instability, flexion-extension arc, pronation–supination arc, MEPS, OES, DASH, quick-DASH (Q-DASH), m-ASES, and ASES-e), outcomes, and p-values were extracted where available.
Included Study Characteristics.
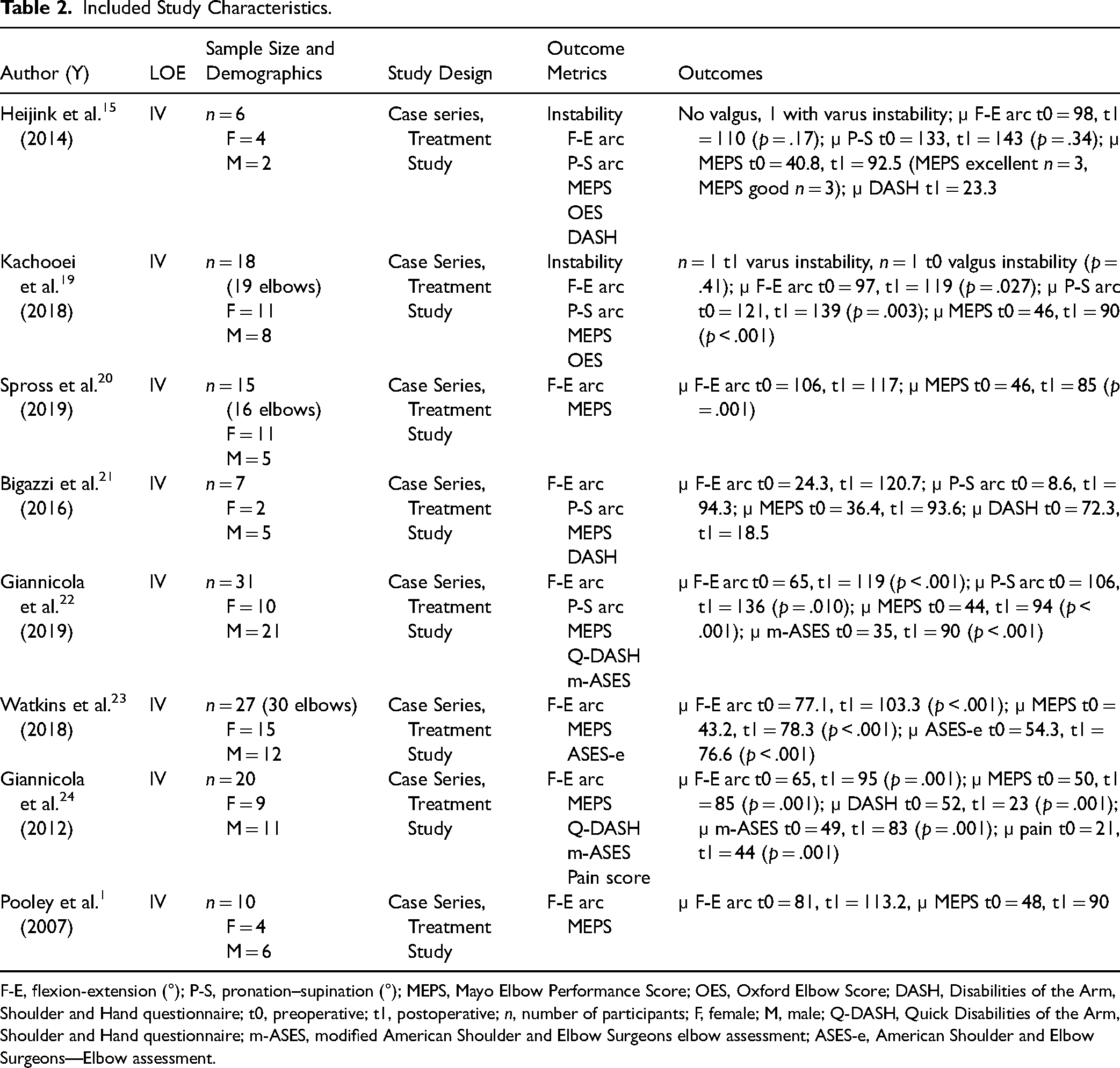
F-E, flexion-extension (°); P-S, pronation–supination (°); MEPS, Mayo Elbow Performance Score; OES, Oxford Elbow Score; DASH, Disabilities of the Arm, Shoulder and Hand questionnaire; t0, preoperative; t1, postoperative; n, number of participants; F, female; M, male; Q-DASH, Quick Disabilities of the Arm, Shoulder and Hand questionnaire; m-ASES, modified American Shoulder and Elbow Surgeons elbow assessment; ASES-e, American Shoulder and Elbow Surgeons—Elbow assessment.
Statistics
Summary statistics (µ, SD) for MEPS, flexion-extension arc, and pronation–supination arc were successfully extracted from 6 of the 8 studies meeting inclusion criteria. The Giannicola 2019 study did not report SD, and so SD estimates were backcalculated using the range method postulated by Walter and Yao. 25 The Watkins 2018 study only reported sample mean, and thus could not be included in the meta-analysis. Standard mean difference (SMD) and corresponding 95% CI were estimated and pooled to assess the difference between pre- and post-operative measures. Heterogeneity was tested using Cochran's Q-test (significance defined as p < .10) and further measured by I2 statistics (I2 > 50% indicating significant heterogeneity). A random-effect model was used to calculate pooled SMD in cases of significant heterogeneity (p < .10 or I2 > 50%); a common effect model was used in all other cases. SMD of 0.2, 0.5, and 0.8 were considered small, moderate, and large effect sizes. 26 The outcome of meta-analysis was summarized using a forest plot, and potential publication bias was detected using egger's funnel plot (p < .05 significance). All analyses were performed using R (version 3.6.2) and R Studio (version 1.3.959) softwares.
Risk of Bias
The eight included articles were assessed for risk of bias using the revised Cochrane Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I). This tool (Figure 3) assesses risk of bias in seven different domains with an overall judgment based on these domains. 27 The review was conducted by 2 authors (D.T.H., J.H.B.). Consistency was high between the two reviewers. Traffic-light plot (Figure 4) figure was created using the Cochrane risk-of-bias visualization (RoB2.0) tool to visualize the risk of bias assessment for each included article. 28

Revised cochrane risk of bias in nonrandomized studies of interventions (ROBINS-I) assessment tool.

Traffic-light plot using the cochrane risk-of-bias visualization (RoB2.0) tool.
Results
MEPS Analysis
Of the 7 studies included in the meta-analysis, 7 had data on pre/post-operative MEPS. The SD backcalculation for Giannicola et al. 2019 was calculated for preoperative (SD = 9.80) and postoperative (SD = 20.70) MEPS for inclusion in the meta-analysis calculations. A meta-analysis was completed with respect to MEPS and is summarized in the forest plot in Figure 5. The pooled SMD was found to be statistically significant between pre-operative and post-operative outcomes (SMD = 3.04, 95% CI [2.40, 3.67]). Cochran's Q-test (p = .04) and I2 statistics (I2 = 54%) indicated statistically significant heterogeneity.
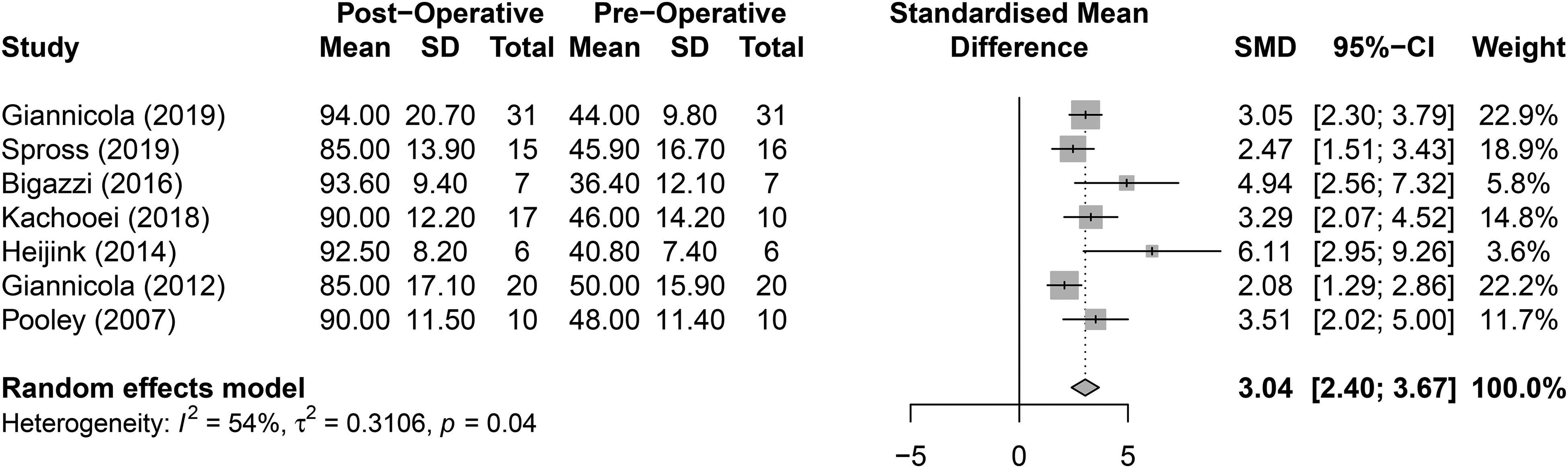
Meta-analysis of pre- and post-operative Mayo elbow performance Index (MEPS).
Flexion-Extension Arc Analysis
Of the 7 studies included in the meta-analysis, 7 had data on pre/post-operative flexion-extension arc. The SD backcalculation for Giannicola et al. 2019 was calculated for preoperative (SD = 31.7) and postoperative (SD = 23.1) flexion-extension arc for inclusion in the meta-analysis calculations. A meta-analysis was completed regarding flexion-extension arc and is summarized in the forest plot in Figure 6. The pooled SMD was found to be statistically significant between pre-operative and post-operative outcomes (SMD = 1.28, 95% CI [0.73,1.83]). Cochran's Q-test (p < .01) and I2 statistics (I2 = 67%) indicated statistically significant heterogeneity.

Meta-analysis of pre- and post-operative flexion-extension arc.
Pronation–Supination Arc Analysis
Of the 7 studies included in the meta-analysis, 4 had data on pre/post-operative pronation–supination arc. The SD backcalculation for Giannicola et al. 2019 was calculated for preoperative (SD = 41.4) and postoperative (SD = 34.1) pronation–supination arc for inclusion in the meta-analysis calculations. A meta-analysis was completed regarding pronation–supination arc and is summarized in the forest plot in Figure 7. The pooled SMD was found to be statistically significant between pre-operative and post-operative outcomes (SMD = 0.81, 95% CI [0.43, 1.18]). Cochran's Q-test (p = .15) and I2 statistics (I2 = 43%) did not indicate statistically significant heterogeneity.

Meta-analysis of pre- and post-operative pronation–supination arc.
Indications and Follow-Up Analysis
Of the 109 included elbows analyzed, 51 (46.8%) had RCA due to primary OA, 37 (34%) due to post-traumatic OA, 7 (6%) due to elbow revision, 5 (5%) due to avascular necrosis, 7 (6%) due to fracture, and 2 (2%) due to rheumatoid arthritis. Heijink et al. reported a mean follow-up time of 50 months (range, 30–64 months), Kachooei et al. reported a mean follow-up time of 35 months (range, 12–88 months), Spross et al. reported a mean follow-up time of 3.4 years (range, 2–6 years), Bigazzi et al. reported a mean follow-up time of 40 months (range, 12–50 months), Giannicola et al. 2019 reported a mean follow-up time of 6.8 years (range, 3.8–11.5 years), Giannicola et al. 2012 reported a mean follow-up time of 22.6 months (range, 6–47 months), and Pooley et al. reported a range of follow-up from 9 to 18 months.
Discussion
Utility of the RCA
Radiocapitellar arthritis can stem from multiple etiologies including post-traumatic, degenerative, and inflammatory arthritis. Conservative treatment strategies consist of anti-inflammatory medications and cortisone injections, physical therapy, and bracing. Treatment options when these conservative measures fail include open or arthroscopic debridement with or without radial head excision and excision of osteophytes, synovium, and loose bodies and joint replacement/resurfacing surgery. The subset of patients that present with severe lateral elbow pain, normal elbow radiographs but in whom arthroscopy/open surgery reveals complete loss of the articular cartilage from the radiocapitellar joint remain a challenge for the treating surgeon. The known complications associated with resection of the radial head include neurovascular damage, cubitus valgus, progressive ulnohumeral arthritis, loss of strength, myositis ossificans, and forearm longitudinal instability. 29 Thus, re-establishing the native anatomy, when possible, should be considered in the arthritic elbow. This review indicates that range of motion (ROM), pain, and daily function improved after RCA intervention as assessed by objective and subjective measures. Our results show there was a large (>0.8) SMD for pre- and post-operative MEPS (SMD = 3.04, 95% CI [2.40, 3.67]), flexion-extension arc (SMD = 1.28, 95% CI [0.73, 1.83]), and pronation–supination (SMD = 0.81, 95% CI [0.43, 1.18]) in favor of the RCA intervention. A conservative estimate of SMD using the lower 95% CI showed large, moderate, and small SMD for MEPS, flexion-extension arc, and pronation–supination, respectively. The indications for RCA in this meta-analysis were diverse; OA, rheumatoid arthritis, fracture, failed osteosynthesis of the radial head and proximal metaphysis of ulna with capitellar OA, and capitellar osteonecrosis. The variety of indications for RCA coupled with the substantial improvements in ROM and patient reported outcomes, make it an efficacious treatment option for patients especially those with inflammatory or degenerative pathologies. These findings suggest that RCA is an alternative treatment for degenerative and inflammatory conditions of the elbow. Young patients, in which the severity of degenerative changes due to primary OA, post-traumatic OA or rheumatoid arthritis involving the lateral compartment of the elbow is severe but total elbow replacement arthroplasty (TEA) would not be an option are the subset of patients this type of procedure should be considered. The review demonstrates this should be a consideration regardless of the etiology of the degenerative changes within the radiocapitellar joint.
There was significant heterogeneity between studies for MEP (I2 = 54%, p = .04) and flexion-extension arc (I2 = 67%, p ≤ .01). One contributing factor could be the diversity of indications for RCA between studies. For instance, Bigazzi et al. 21 reported 3 out of 7 patients with 0 degrees on flexion-extension arc. These same patients had trauma or fractures as the precipitating event for RCA, and thus could not perform the pre-operative assessment. When compared to patients with degenerative or inflammatory pathologies, this traumatic sub-population of patient will inherently perform lower on pre-operative ROM and PROs (patient reported outcomes), skewing the meta-analysis toward increased heterogeneity. An additional source of heterogeneity could be variations on how assessments were performed between studies.
Additional Outcomes
The review included a combination of patient and clinician reported outcomes to capture the impact of RCA, however, additional patient reported outcomes exist that offer valid and useful data. Heijink et al. 15 and Bigazzi et al. 21 reported disabilities of the arm, shoulder, and hand (DASH) scores in their respective reviews. DASH is a 30-item disability scale, scored 0 (no disability) to 100. 30 Heijink et al. found a mean postoperative DASH score of 24.3 indicating that patients had residual symptoms that were mild to moderate while Bigazzi et al. found a mean preoperative DASH score of 72.3 and postoperative DASH score of 18.5 indicating an improvement in disability after treatment. An additional variation of DASH called Q-DASH (quick-DASH) was employed by Giannicola et al. in their 2012 24 and 2019 22 publications. Q-DASH uses 11 of the 30 items in the traditional DASH but offers a valid alternative in a less extensive questionnaire. Giannicola et al. 2012 24 found a mean pre-operative Q-DASH of 52 and post-operative Q-DASH of 23. Giannicola et al. 2019 22 evaluated two prostheses and found that the LRE system and the Uni-Elbow Radio-Capitellum Implant (UNI-E) showed improvements in post-operative Q-DASH (9 and 17) compared to pre-operative Q-DASH (66 and 66), respectively. Giannicola et al. 2019 also demonstrated that patients who were treated with the LRE showed significant decreases in all parameters (extension, flexion, extension/flexion arc, pronation, pronation/supination arc, MEPS, Q-DASH, and m-ASES) except supination (p = .305) to which they commented that that pre-operative supination was satisfactory. In addition, the data showed that all parameters were improved post-operatively in those treated with the UNI-E implant.
These data further suggest that RCA offers a viable intervention for individuals suffering from isolated radiocapitellar pathology. This intervention prolongs the need for TEA with permanent lifting restrictions and offers satisfactory results regarding function and pain.
Future Aims
The LRE is the only current implantable RCA device, and furthermore is only available in the European market. As discussed previously, isolated elbow OA is a much more prevalent condition than is apparent, and more so, the use of RCA is sparse due to the limited global awareness and availability. In the coming years, global accessibility and awareness for this implant is necessary for advancing elbow joint care as a specialty. As the awareness of utility for RCA grows, it will be imperative to maximize outcomes regarding operative technique, implant design, and patient satisfaction through randomized control trials in the future.
Limitations
Major limitations of this study were the search methodology and the lack of reported patient specific data from Giannicola et al. 2019 and Watkins et al. Due to the likelihood of improper filtering and inability to screen for duplicates, additional databases were not included in this review. Additionally, throughout the review process, one article was identified as satisfying inclusion criteria, although it was not found on the PubMed database. This article was included in the systematic review, which may have introduced selection bias. Due to the absence of patient specific data from Giannicola et al. 2019, an estimated standard deviation was calculated using the range method postulated by Walter and Yao, 25 which may have introduced statistical error to the meta-analysis. In addition, the lack of patient specific data from Watkins et al. could have skewed the meta-analysis and caused the statistical analysis to be underpowered. This review was also limited by the lack of prospective, randomized controlled trials. Each study included in this review was a case series, therefore increasing the risk of bias.
Conclusions
Patients undergoing RCA showed statistically significant improvements in flexion-extension arc, pronation–supination arc, and Mayo Elbow Performance Scores compared to pre-operative measures. The pooled SMD was found to be statistically significant between pre-operative and post-operative outcomes for MEPS (SMD = 3.04, 95% CI [2.40, 3.67]), flexion-extension arc (SMD = 1.28, 95% CI [0.73, 1.83]), and pronation–supination arc (SMD = 0.81, 95% CI [0.43, 1.18]). Cochran's Q-test and I2 statistics indicated statistically significant heterogeneity for MEPS (p = .04, I2 = 54%) and flexion-extension arc (p < .01, I2 = 67%). These data suggest that RCA may be offered as an alternative treatment option. Additionally, we have outlined the need for improved standard of care for individuals with isolated radiocapitellar pathology, a commonly underdiagnosed condition. Within this subset population, RCA may yield success in younger patients of whom would prefer to delay TEA. This study highlights the underutilization and lack of availability for isolated RCA, and therefore identifies a need for future randomized control trials to improve the awareness and utility of RCA.
Footnotes
Acknowledgments
The authors thank Dr Allison Tegge with the Virginia Tech Department of Statistics for the collaboration of the statistical analysis. Additionally, they thank the Health Sciences Libraries at Carilion Clinic and Virginia Tech Carilion School of Medicine for supplying all necessary literature for this review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: the Musculoskeletal Education and Research Center within the Department of Orthopaedic Surgery at Carilion Clinic Institute for Orthopaedics and Neurosciences.