
Abstract
The objective of this review is to summarize the surgical options for primary osteoarthritis of the elbow, reported clinical outcomes, and suggested indications in previous literatures. The surgical management of primary elbow arthritis has evolved because of an improved understanding of pathologic mechanisms and manifestations as well as the development of novel surgical techniques and devices. Osteocapsular arthroplasty (OCA), elbow debridement, distraction arthroplasty, and total elbow arthroplasty (TEA) have been employed for managing elbow osteoarthritis. Elbow debridement and OCA can be helpful in most cases of symptomatic elbow arthritis. TEA is usually recommended for end-stage arthritis in elderly patients after prosthetic implants have been in place for long periods or after complications. Distraction arthroplasty might find a place in the treatment of younger, active patients with end-stage arthritis.
Keywords
Introduction
Primary osteoarthritis is characterized by the degeneration of hyaline articular cartilage, which exposes the subchondral bone. Elbow osteoarthritis is uncommon as compared with osteoarthritis in other joints. It has been reported to affect up to 2% of the general population and is more prevalent in men than in women. 1,2 More importantly, its incidence is higher in the people who overuse upper extremities; for example, manual laborers, throwing athletes, and individuals requiring wheelchair assistance. 3
Elbow arthritis has been referred to as a “marginal disease” based on a practical perspective 4 ; that is, a consistent pattern of osteophyte formation results in a rim around each of the margins of the humeral, ulnar, and radial articular surfaces, with maintenance of the joint space. This forms the basis of the treatment, which comprises the debridement of these osteophytes that are responsible for impingement pain and motion loss.
Because the main complaints associated with symptomatic elbow osteoarthritis are pain at the terminal range of motion (ROM) and mechanical symptoms (impingement, locking, and crepitus) from intra-articular osteophytes and loose bodies, the surgical interventions need to address these aspects. 5,6 Osteocapsular arthroplasty (OCA) has been widely performed to manage early- or mid-stage disease and obtain favorable outcomes. 7,8 In contrast, prosthetic elbow replacement is only offered for end-stage osteoarthritis, but it has been associated with relatively higher complication rates. 8,9
The objective of this review article is to summarize the surgical options for primary osteoarthritis of the elbow, reported clinical outcomes, and suggested indications in previous literatures.
Etiology
Genetics, ethnicity, aging, repetitive minor trauma, and unbalanced joint loading due to instability or malalignment have all been reported as important etiologic factors that are associated with elbow osteoarthritis. 10 –12 The onset and progression of arthritis appear to be highly associated with an underlying imbalance in the cytokine-mediated anabolic and catabolic processes of articular chondrocytes. 13 Additionally, changes in water and proteoglycan homeostasis in the osteoarthritic cartilage have direct effects on cartilage health. 14 –16 However, the understanding of onset mechanisms and natural history of the disease still remains limited. 2
It is now widely accepted that elbow osteoarthritis begins at the radiocapitellar joint. A previous biomechanical study suggested the radiocapitellar joint as a target for elbow osteoarthritis at the onset of disease. The radiocapitellar joint, which has a smaller articular surface than that of the ulnohumeral joint, takes 55% of the axial loading in the neutral forearm position. 17 Jeon et al. speculated that the zona conoidea could be a point of susceptibility in the development of osteoarthritis due to the alternating contact and separation during supination and pronation along with the associated changes in loading as it is implied. 18 Advanced degeneration in the radiocapitellar joint relative to the ulnohumeral joint has been associated with progressive changes from the radiocapitellar joint to the ulnohumeral joint. 19,20 These changes have been associated with posteromedial cartilage defects in the radial head and corresponding defects in the posterior part of the crest that separates the trochlea from the capitellum. However, no such pattern of degeneration affecting the ulnohumeral articulation has been described in literature. Studies on large numbers of specimens or patients are needed to clarify the predisposing factors for elbow degeneration.
Clinical presentation
Patients with osteoarthritis typically present with initial symptoms at the age of about 50 years,
1,5
and this disease more commonly affects men, with a male-to-female ratio of 4:1.
21
The dominant extremity is more commonly involved in osteoarthritis. Patients with elbow arthritis typically present with complaints of pain, weakness, and loss of motion. Loss of motion: functional ROM required for daily living activities is considered to be an arc of motion of 100 degrees (30 degrees of extension to 130 degrees of flexion) and a 100-degree arc of forearm rotation (50 degrees of pronation to 50 degrees of supination). Capsular contracture and osteophytes in the fossa and processes of the olecranon and coronoid are the main pathologic mechanisms resulting in the loss of motion. Pain of impingement (endpoint pain): patients commonly feel pain at the end of motion in flexion and extension. Radiologic evidence demonstrates the destruction of the three-dimensional matching of shape in the olecranon and coronoid fossa and process, with point contact due to osteophyte formation. The concentration of contact force at the point contact area could be a possible explanation, but the reason of impinging pain is still unclear. Pain in the rest or mid-arc: some patients complain of pain in the mid-arc of motion and even at rest. This type of pain occurs due to cartilage erosion or destruction that characterizes advanced elbow arthritis. If this type of pain is subtle or inconsistent, then elbow motion with axial loading as a provocative test would be helpful. Ulnar nerve neuropathy or irritation.
Because the disease is characterized by marginal osteophytes involving the cubital tunnel, ulnar nerve irritation is a common clinical presentation. Ulnar nerve involvement should be carefully examined, especially among patients with previous elbow trauma or surgery, because it affects surgical decision-making and is related to revision or reoperation rate. Ulnar nerve release is associated with a low rate of reoperation for ulnar nerve decompression in patients with elbow contracture release and preoperative ulnar nerve symptoms or a positive Tinel test. 22 Prophylactic ulnar nerve release has been advised for elbows with high-grade stiffness (less than 90–100 degrees of preoperative flexion); otherwise, it is not an absolute necessity. 22 –24
Radiologic assessment
Because the main symptoms of elbow osteoarthritis are resting pain, mid-arc pain due to joint cartilage destruction, endpoint pain, and limited ROM due to spurs and loose bodies, a staging system, or classification for elbow arthritis should include symptom-related factors to guide treatment. To determine the severity of disease, the Broberg and Morrey classification and the Hastings and Rettig classification have been used for qualitative staging. The Broberg and Morrey system 25 is based on the formation of osteophytes and narrowing of joint space. The Hastings and Rettig system 26 is based on the presence of subluxation and involvement of the radiocapitellar joint.
Plain radiographic staging systems
In the Broberg and Morrey system, grade 0 is defined as a normal joint, grade I as a slight narrowing of joint space with a minimum formation of osteophytes, grade II as a moderate narrowing of joint space with a moderate formation of osteophyte, and grade III as severe degenerative change with a gross destruction of the joint. In the Hastings and Rettig system, class I is defined as degeneration at the margins of the ulnotrochlear joint, with the presence of coronoid and olecranon spurring and the absence of degenerative changes within the radiocapitellar joint; class II is defined as class I plus mild narrowing of joint space within the radiocapitellar joint, without subluxation of the radial head; and class III is defined as class II plus radiocapitellar subluxation.
Computed tomography (CT)–based staging system
In the CT-based staging system (Figure 1), the quantification of spurs in the fossa is performed by measuring the involved depth on sagittal CT sections. More than 50% involvement of the fossa is defined as an “involved fossa.” “Joint space narrowing” is defined as the presence of a gap of more than 1 mm in the ulnohumeral joint in more than 50% of the joint space in the reference section. Grade 0 is defined by a lack of involved fossa with intact joint space, grade 1 as uni-compartmentally involved fossa with an intact ulnohumeral joint space, grade 2 as bi-compartmentally involved fossa with an intact ulnohumeral joint space, and grade 3 as joint space narrowing regardless of the state of the fossa. CT-based staging is highly reproducible and more clinically feasible than previous plain radiograph–based staging systems. 27

Summary of CT-based classification for primary elbow osteoarthritis. More than 50% involvement of the fossa is defined as an “involved fossa.” “Joint space narrowing” is defined as the presence of a gap of more than 1 mm in the ulnohumeral joint in more than 50% of the joint space on the reference section. Grade 0: no involved fossa with intact joint space. Grade 1: uni-compartmentally involved fossa with an intact joint space. Grade 2: bi-compartmentally involved fossa with an intact joint space. Grade 3: joint space narrowing regardless of the state of the fossa.
Management
Nonsurgical treatment
Symptomatic treatment is appropriate, especially in the early stages, because symptoms are slowly progressive and well tolerated. Activity avoidance may be effective initially. Nonsteroidal anti-inflammatory drugs and intra-articular corticosteroid injections are often helpful in alleviating symptoms. Physical therapy may include pain control measures, such as avoidance of activities that put a high stress on the elbow and gentle ROM exercises to maintain muscle mobility and strength. The most important feature of the initial treatment is to explain the potential causes and the natural history of the process to the patients so that they can modify their activities accordingly. Patients should avoid activities that increase pressure on the cubital tunnel if there are ulnar nerve symptoms.
Surgical treatment
OCA
OCA was initially performed in an open manner and comprises capsular release, synovectomy, and the removal of osteophytes and loose bodies for reducing mechanical symptoms, thus improving ROM. The goal of this surgical procedure is to relieve the pain associated with mechanical symptoms and recover functional ROM. Favorable outcomes with lower complication rates have also been reported in various studies. 28 –30 With advances in minimally invasive surgical techniques, the arthroscopic approach has emerged as an attractive option for managing both mechanical impingement resulting from osteophytes and soft tissue contractures. The benefits of arthroscopic OCA include its association with minimal surgical damage, which promotes rapid rehabilitation and lowers the risk of capsular contractures by reducing the morbidity associated with a large incision and exposure of the joint.
(1) Indications and contraindications
The typical indication for arthroscopic OCA is the functional loss of elbow motion and impingement pain due to the formation of osteophytes and capsular contracture. For patients with a functional arc of motion, which is defined as flexion from 30 to 130 degrees preoperatively, 31 the indication for surgery is painful impingement or functional impairment due to the need for terminal elbow extension. This indication is not applicable to all patients. Although most people can lead normal lives with a functional arc of motion of the elbow, young and high-demand patients (usually athletes) cannot tolerate lesser degrees of contraction. Low radiologic grades with obvious symptoms (e.g., impingement pain and mechanical symptoms of loose bodies) can also be considered for the procedure. For these patients, arthroscopic OCA can be performed to treat even less severe contractures. 32,33
Advanced elbow arthritis is associated with poor clinical and radiologic outcomes, 34 and end-stage elbow osteoarthritis can be considered as a relative contraindication. However, elbow debridement or OCA is still an option even for advanced elbow osteoarthritis as a palliative treatment for patients who do not accept total elbow arthroplasty (TEA) or are not suitable candidates for TEA due to infection.
Substantial anatomic distortion is a relative contraindication. Prior submuscular transposition of the ulnar nerve may be a selective contraindication depending on the surgeon’s experience. Dislocation or prior subcutaneous transposition of the ulnar nerve, failed prior contracture release, or extensive scarring from skin grafts or flaps are not regarded as contraindications.
(2) Surgical technique
1) Open debridement arthroplasty
Open debridement arthroplasty is performed with a posteromedial or lateral approach with a column procedure. 35 –37 Ulnar nerve release or anterior transposition can be achieved through the same approach in patients with preoperative ulnar neuropathy or flexion less than 90 degrees. While using the lateral (Kocher) approach, it is possible to use the anterior and posterior capsules in the column procedure after detecting the lateral supracondylar ridge.
Anterior compartment
The origin of the flexor–pronator muscle group is elevated from the medial epicondyle. All the anterior structures in the distal humeral region are elevated subperiosteally. The anterior band of the medial collateral ligament (MCL) needs to be preserved. The flexor or pronator origin and the anterior capsule are dissected down to the bone. Osteophytes and loose bodies are removed from the coronoid process, the coronoid fossa, and the radial fossa with the use of a rongeur or an osteotome.
Posterior compartment
The ulnar nerve is fully mobilized so that it can be transposed anteriorly or released further. The medial joint line is exposed up to the anterior band, and the posterior band of the MCL is excised. Next, the posterior capsule is excised by elevating the triceps with a deep retractor. Osteophytes are removed from the olecranon and olecranon fossa.
Lateral compartment
The lateral compartment is exposed through a lateral skin incision that extends distally from the lateral supracondylar ridge of the humerus to the posterior border of the ulna. The dissection between the triceps and the brachioradialis muscles exposes the lateral condyle and joint capsule. Importantly, the dissection through the radial edge of the anconeus muscle allows the radial head to be exposed by the longitudinal incision of the annular ligament. The anterior joint capsule is dissected subperiosteally. Spurs are removed from the radial head, the radial fossa, and the posterior edge of the capitellum. The joint is observed from both the medial and the lateral incision, and the osteophytes that limit motion are cleared completely.
2) O-K (Outerbridge–Kashiwagi) procedure
The Outerbridge procedure, as popularized by Kashiwagi, has been verified as an effective method for relieving pain and improving motility in patients with osteoarthritic elbows. 38 –42 It was designed to deepen and widen the olecranon fossa, thus removing osteophytes and loose bodies in the posterior compartment and eventually fenestrating the olecranon fossa to the coronoid fossa. This procedure allows access to the anterior compartment and coronoid osteophytes through this fenestration. The mini-open or modified O-K procedure has been introduced recently as a less invasive option. 38,42 The surgical procedure starts with a longitudinal incision of 4 cm (Figure 2(a)). The triceps tendon is then split, and the tip of the olecranon is osteotomized. A posterior capsulectomy can be performed through the split triceps (Figure 2(b)). With the exposure of olecranon fossa, all loose bodies, and contracted capsules are removed. After identifying the floor of the olecranon fossa, a high-speed burr is used to create an elliptical window. A small osteotome can be inserted through this window to remove the tip of the coronoid and release the anterior capsule. Any loose bodies in the anterior compartment of the elbow may be removed through the window. Gelfoam is inserted through the window (Figure 2(c)). Special attention is needed to avoid the over-resection of bone from the medial column, which is usually thinner than that in the lateral column and may be prone to fracture while making the hole. 43
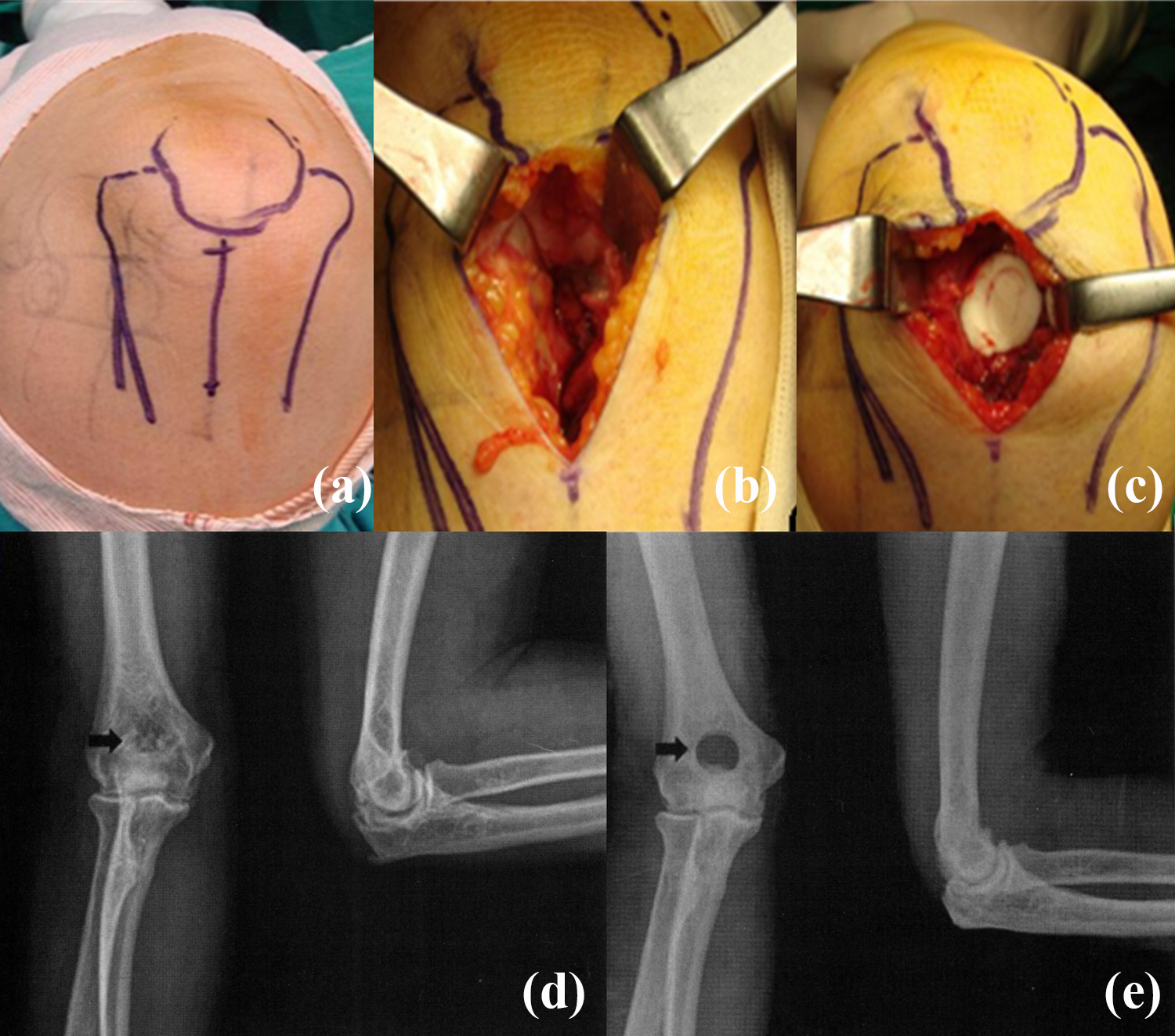
Outerbridge–Kashiwagi (O-K) procedure. (a) Draw the landmarks of the surface anatomy of the elbow in the supine position. Make an approximately midline longitudinal skin incision of 4 cm proximally from the olecrenon on the distal posterior humeral area. (b) After exposing the olecrenon fossa, make a round window by drilling with a trephine. Through this window, detach the loose bodies and osteophytes in olecranon (posteriorly), coronoid (anteriorly) during passive flexion and extension. (c) After removing all the osteophytes and loose bodies, insert Gelfoam through the window. (d) Preoperative X-ray. (e) Postoperative X-ray.
3) Arthroscopic OCA
General anesthesia is administered, and the patient is placed in the lateral decubitus position with the arm resting on an arm holder. The elbows are set to allow a full assessment of postoperative flexion and extension. Considering that the radial nerve shifts medially (further from the portal) during flexion and laterally during extension, 30,44 the shoulder is flexed between 90 and 100 degrees, and the elbow rests at 90 degrees of flexion. For OCA, the patient positioning is critical for an adequate access to the coronoid and coronoid fossa without the working instruments hitting the patient’s chest. Specifically, the shoulder should be elevated forward at least 90 degrees, and the elbow should be kept at least as high as the shoulder. Standard elbow arthroscopy portals (proximal anteromedial, anterolateral, direct posterior, and posterolateral) and an accessory portal for an intra-articular retractor are used. Anterior capsulectomy with an arthroscopic shaver (Figure 3(e) and (f)) is performed after removing all osteophytes and loose bodies from the coronoid fossa (Figure 3(a) and (b)). The direct posterior portal is used, along with the posterolateral portal, to remove osteophytes and loose bodies in the olecranon fossa and the tip of the olecranon (Figure 3(c) and (d)). Both posteromedial and posterolateral gutters are also debrided. Posterior capsulotomy is considered when satisfactory flexion cannot be achieved with the anterior compartment procedure. In cases of limited ROM, especially for flexion limitations, the mini-open ulnar nerve decompression through an incision of 2 cm is performed to avoid the postoperative stretch neuropathy.
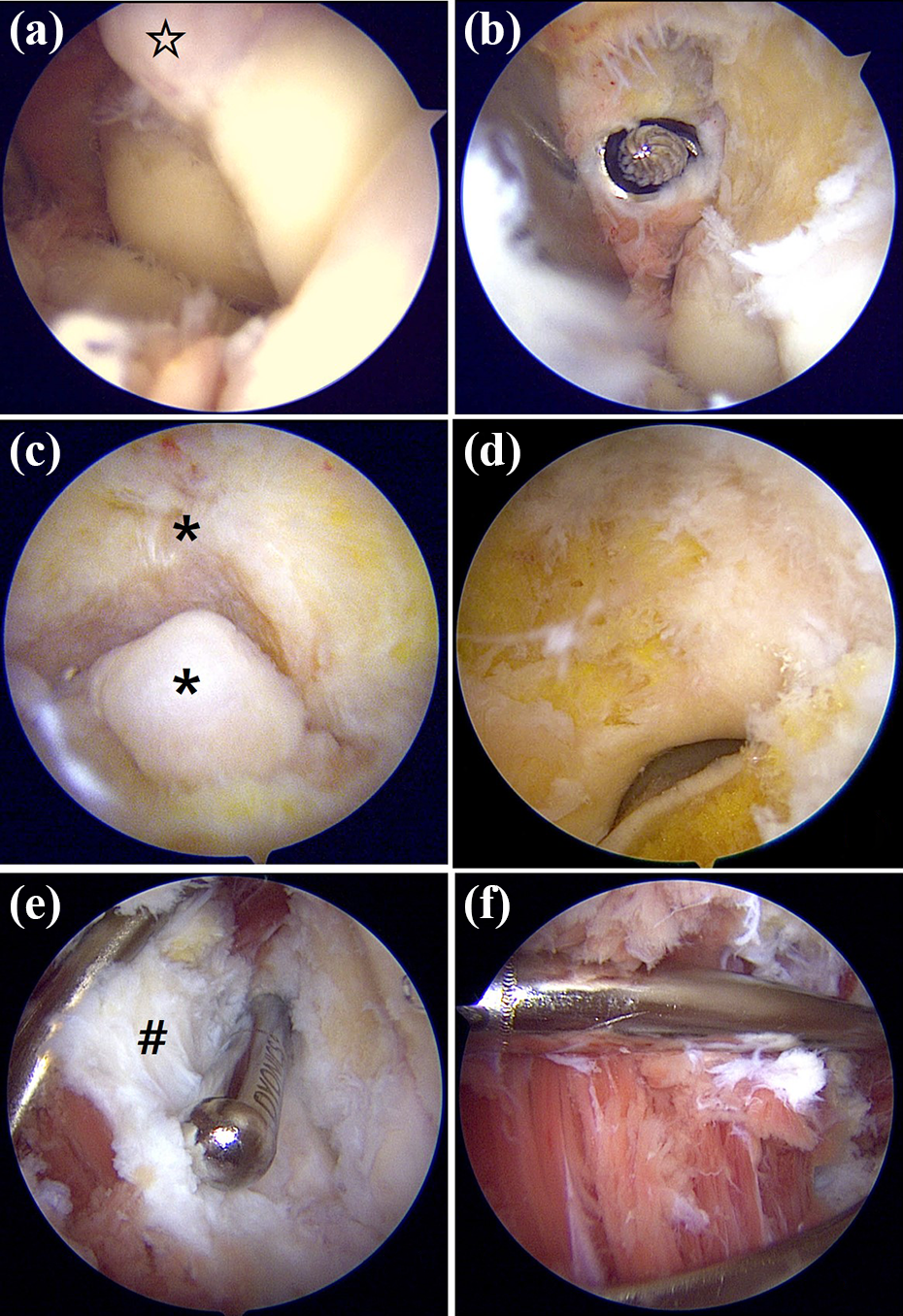
Arthroscopic osteocapsular arthroplasty. (a and b) Clearance in the coronoid fossa; ☆osteophyte in the coronoid fossa. (c and d) Clearance in the olecranon fossa and process; *osteophyte in the olecranon fossa and process. (e and f) Anterior capsulectomy; #contracted anterior capsule.
Postoperative management
The goal of ROM recovery, intraoperatively, is a functional ROM of at least 30–130 degrees extension–flexion and 50 degrees pronation–supination. After surgery, a soft compressive dressing and an anterior splint are applied. Neurologic examination is performed by the surgeon after recovery from anesthesia. After the surgeon confirms an intact neurologic function, the elbow is placed in extension and supination for 24 hours. From postoperative day 1, an immediate motion is encouraged under the guidance of the clinic physician. With assistance from the contralateral hand, the patient gradually increases the ROM in both extension and flexion, with nighttime splinting for the first 3–4 weeks.
(3) Clinical outcomes (open surgery versus arthroscopy)
Open debridement has been widely performed and supported by many experienced surgeons with favorable clinical outcomes for pain relief and ROM recovery. It has been suggested that any functional restoration or symptom relief that can be achieved by open surgery can be fully accomplished by arthroscopy. 34,45,46 A recent study also reported the comparable clinical outcomes associated with arthroscopic OCA with the important finding that neither procedure can guarantee excellent outcomes in patients with advanced osteoarthritis. 47 In a systematic review, Kim et al. reported that both open and arthroscopic OCA improve ROM and clinical scores and that open debridement is associated with a relatively higher complication and reoperation rates than arthroscopic OCA. 48 However, arthroscopic OCA is more technically demanding than open surgery, and the surgeon’s experience and familiarity with the technique are essential to avoid neurovascular injury.
(4) Complication that requires special attention
Delayed-onset ulnar neuritis (DOUN) may occur after the restoration of elbow motion. 23,49 The incidence of DOUN has been reported to be 11% after the arthroscopic contracture release of the elbow. There are three distinct clinical presentation patterns: rapidly progressive, non-progressive, and slowly progressive. The rapidly progressive pattern—characterized by increasing pain in the cubital tunnel, progressive loss of elbow motion, and neuropathy—is the most common pattern that requires an urgent reoperation for nerve management. If ulnar nerve transposition is delayed beyond 2 weeks after surgery, then a complete recovery of neurological function does not occur. Three factors are significantly associated with an increased DOUN risk: preoperative hypertrophic ossification, preoperative neurological symptoms, and preoperative arc of motion. We recommend a limited open ulnar nerve decompression before the procedure while maintaining a high index of suspicion and avoiding end-range stretching if it causes symptoms such as ulnar neuritis or pain near the cubital tunnel.
TEA
TEA was originally developed to manage end-stage rheumatoid arthritis, but indications have been expanded to include unfixable comminuted fractures, post-traumatic arthritis, and primary osteoarthritis. Because TEA is rarely performed, most surgeons have minimal experience with the procedure as compared with hip and knee arthroplasty, and few long-term outcome data are available. Therefore, surgeons must learn about this procedure by carefully reviewing the previous literature to avoid making unnecessary mistakes.
(1) Indications with different implant designs
End-stage elbow osteoarthritis with uncontrolled resting pain or mid-arc pain and without any infection sign is an indication for TEA. However, there is still no consensus for young or active patients due to the concern surrounding implant longevity.
A recent systematic review has reported 19 specific implant designs. 8 The implants can be classified into four different general categories: unlinked, linked, semiconstrained, and convertible (unlinked or linked) (Figure 4). An absolute prerequisite for applying the unlinked design is an intact, repairable, or reconstructable collateral ligament. However, even after an unlinked TEA is inserted with an intact collateral ligament, collateral ligament insufficiency could pose an issue that possibly causes implant failure and sometimes necessitates a revision surgery. More recently, convertible TEAs (Latitude Tornier implant system, Tornier, Montbonnot–Saint-Ismier Cedex, France) have allowed surgeons to choose between implanting a nonconstrained or semiconstrained prosthesis. If the surgeon has concerns regarding collateral ligament insufficiency or implant stability, then a semiconstrained hinge can be created by applying a modular component to the ulnar prosthesis. Two-year follow-up outcomes associated with convertible TEA are comparable with those of historical controls; however, no long-term survival data have been reported. 50

Hinge designs in four different total elbow prosthesis. (a) Kudo type-5 total elbow prosthesis (unlinked hinge). (b) Nexel total elbow prosthesis (linked hinge). (c) Discovery total elbow prosthesis (semiconstrained hinge). (d) Latitude total elbow prosthesis (convertible hinge).
(2) Surgical approach for TEA
There have been emerging concerns for triceps insufficiency in TEA with the reported failure rates of triceps up to 11%. 51,52 The complication of triceps is avoided by the meticulous surgical approach to maintain the maximized extensor mechanism. Therefore, the handling of the triceps tendon during the approach continues to evolve as well. 53 Triceps turndown, 54,55 triceps splitting, 56 triceps reflecting, and triceps-sparing 53,57 –60 approaches have also been introduced in the literature. The selection of the surgical exposure practically relies on the surgeon’s preference and experience. Increasing the importance of extensor mechanism of elbow, the triceps-sparing approach theoretically has been considered as the best option for preserving the extension mechanism. However, leaving the triceps attached is technically challenging, especially for those less familiar with elbow arthroplasty, and specifically for exposing the ulna. 61 Considering that the sufficient exposure would allow the correct implant positioning, the critical disadvantage of a triceps-sparing approach is the limited visualization for surgical exposure. The previous cadaveric studies reported that the visualization of articular surface using a triceps turndown, a triceps splitting, a triceps elevating approach, and an olecranon osteotomy allowed 75%, 35%, 37%, and 51% of visualization, respectively. 62 –64 Unlike a triceps reflecting approach, the ulna cannot be fully accessed with hyperflexion as the tension of the triceps inhibits this maneuver. However, there are no studies dealing with the exposure of the ulna-articular surface with different approaches. 65 It is important for the treating surgeon to be able to perform many of these various exposures depending on a patient’s presentation with various types of implants to have the greatest chance of success.
(3) Clinical outcomes of primary elbow osteoarthritis
Patients with primary osteoarthritis typically have higher functional demands and capabilities than those with inflammatory arthritis because osteoarthritis is more commonly associated with overused upper extremities, for example, by manual laborers, throwing athletes, and individuals requiring wheelchair assistance. Hence, it is critical to communicate with patients regarding postoperative management. The surgeon should emphasize that complications are more likely to arise or worsen if the patient continues with the same pattern of habitual elbow use. Schoch et al. reported that TEA represents a reliable surgical option for pain relief in patients with primary osteoarthritis. However, the restoration of extension is not always obtained, thereby indicating that more aggressive soft tissue releases or bony resection should be considered. A study’s result showed that the mean Mayo Elbow Performance score for 13 elbows without mechanical failure was 81.5 (range: 60–100 points). 58
(4) Complications
Due to the popularity of TEA, an increase in complications resulting in revision TEA parallels an increased uptake of primary TEA. It is well known that survival after TEA is substantially longer among patients with inflammatory arthritis than among those with trauma-related indications. 66 –68 However, the clinical outcomes and complications have not been well assessed with large sample sizes because of the low incidence of primary arthritis of the elbow. Linked prostheses tend to require more revisions due to polyethylene wear, whereas more revisions are performed on patients with unlinked prostheses because of instability and dislocations. A recent retrospective study found that 3 of 18 elbows sustained mechanical failure. Complications included intraoperative fracture in two, bony ankylosis in one, humeral loosening in one, humeral component fracture in one, and mechanical failure of a radial head component in one elbow. 58
Radiocapitellar arthroplasty
Radiocapitellar arthroplasty is based on the concept that the advanced degeneration in the radiocapitellar joint relative to the ulnohumeral joint has been associated with progressive changes from the radiocapitellar joint to the ulnohumeral joint. 19,20 A previous biomechanical study supported the procedure with the result that the radiocapitellar arthroplasty showed no difference in kinematics under the condition with the intact MCL as compared with the control. 69 With the theoretical benefit of the procedure, it has been proposed and indicated as a reconstructive option for a combined radial head and capitellar arthritis to eliminate the pain source and to reconstruct the lateral column that shares an axial load to probably decelerate the process of arthritis in the ulnohumeral joint. 17,18 The surgical approach is basically similar with that of the radial head replacement; however, a sufficient exposure of capitellum needs to be addressed for an accurate measurement of implant size. The conventional Kocher approach 70 or extensor tendon split approach 71 can be used to expose the radiocapitellar joint. The humeral LCL insertion is detached for a better exposure. After the radial head osteotomy, the shaft reaming is performed until a firm press fit is obtained. The height of the radial head is measured with the reference of the sigmoid notch. 72 The size of the capitellar component is decided by measuring the lateral side of the capitellum. Osteotomy is performed with the capitellar cutting guide. The resected radial head and capitellar surface are then used to reassess the size of the prosthetic components. After preparing the humeral canal, the definitive capitellar component is inserted. As a final step, the LCL complex is reattached at its humeral insertion. Although recent studies have reported favorable outcomes either in early or mid-term period, the procedure was not popularized with due to limited indications. 71,73 –75 Hence, there is a need for further clinical studies with long-term outcomes.
Distraction interposition arthroplasty
Distraction interposition arthroplasty is rarely indicated. It was proposed with the concept of sparing resection of the destroyed joint surface and creating a new congruent ulnohumeral joint with a graft, such as fascia lata or Achilles allograft. 5,76 A stable elbow with an intact collateral ligament is a prerequisite for preventing instability after interpositional arthroplasty. The collateral ligaments are reconstructed with the graft when they cannot be repaired primarily. A unilateral hinged external fixator is placed to hold the elbow in slight distraction while permitting an active motion immediately postoperatively. Typically, the fixator is left in place for 4 weeks. A recent study introduced the arthroscopic-assisted technique without hinged external fixation with satisfactory mid-term outcomes. 77 Indications for this surgery include painful inflammatory and arthritic elbows that have failed to respond to conservative and operative management, including OCA, radial head excision, and contracture releases. Interposition arthroplasty may be an option for young, active patients with end-stage arthritis, particularly those with severe joint destruction.
No published study has reported on the outcomes of this procedure for the specific indication of primary osteoarthritis. Larson and Morrey 76 reported their outcomes of interposition arthroplasty performed with an Achilles tendon allograft on 45 patients (elbow arthritis was inflammatory in 11 patients and post-traumatic in 34). At a mean follow-up of 6 years, the mean flexion–extension arc improved by 46 degrees in the group of 38 patients with surviving allografts. However, elbow instability was the major complication despite efforts to reconstruct the collateral ligaments.
Surgical considerations for an advanced disease
Although most studies have reported reliable clinical outcomes with surgical management, 29,47,58,78 –83 it is not easy to simply judge the overall outcomes because elbow osteoarthritis has a large spectrum of disease severity. 1,3,5 Therefore, it is an important initial step to assess severity according to symptoms and radiologic evidence. 4 The surgeon is required to understand the limitations of each surgical option. Cartilage-preserving procedures, such as OCA and the O-K procedure, aim to relieve the endpoint impingement pain and limited ROM, not the mid-arc or resting pain and limited ROM arising from cartilage erosion. Because osteophytes and loose bodies represent the principal pathologic mechanism causing impingement pain or terminal pain, the main target of the procedure is the proper removal of osteophytes and loose bodies. However, even after surgery, symptoms of resting pain due to cartilage destruction remain because surgery may not stop the progression of cartilage destruction. In previous retrospective studies, patients with the radiologic evidence of ulnohumeral joint space narrowing had worse clinical outcomes after OCA than those with intact joint spaces. 27,34,47 TEA has been considered as the last option for end-stage osteoarthritis when the symptoms mainly caused by joint destruction are expected to have poor outcomes after cartilage-preserving surgery. However, the exact cut-off point for choosing TEA instead of cartilage-preserving surgery remains undefined. Further comparative studies are warranted, particularly considering the spectrum of disease severity.
Summary
The surgical management of primary elbow arthritis has evolved alongside an improved understanding of pathologic aspects and the development of surgical techniques and devices. OCA, elbow debridement, distraction arthroplasty, and TEA have been used to manage elbow osteoarthritis. Because arthritis is a progressive disease, the elbow eventually progresses to advanced or end-stage arthritis requiring TEA. OCA and elbow debridement surgery still seem to play important roles in the maintenance or restoration of elbow function and amelioration of pain, as well as the deferment of TEA. Radiocapitellar replacement can be considered for isolated advanced osteoarthritis in the radiocapitellar joint. Distraction arthroplasty also might have a place in the treatment of younger, active patients with end-stage arthritis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.