
Abstract
Introduction
Failure after operative treatment of complex proximal humeral fractures (PHF) can prove challenging even for experienced surgeons. Reverse shoulder arthroplasty (RSA) seems to offer a satisfactory revision procedure with good clinical outcomes.
Materials and Methods
We present a case series of 14 patients, who were treated during a 3.5 years period (from 01/2016 until 06/2019). They all underwent revision surgery with RSA for failed operative treatment of PHF. Their mean age was 68 years (range, 51-84 years). 2 patients (14.3%) had been primarily treated with open reduction and internal fixation (ORIF), 5 patients (35.7%) with hemiarthroplasty, 3 patients (21.4%) with closed reduction and percutaneous fixation and 4 patients (28.6%) with transosseous suture fixation (TSF). We evaluated their absolute Constant score (CS), Visual Analogue Scale (VAS) score, and Range of Motion at their final follow-up, and we made a full clinical and radiological assessment to detect any postoperative complications.
Results
The mean absolute CS, VAS score, active anterior elevation, active abduction significantly improved compared with the preoperative status. Less significant difference was found in external rotation when comparing with the preoperative status (P = .0304). No significant differences were found when comparing RSA for different failed primary techniques (P > .05). No complications were detected following the revision surgeries of all patients.
Conclusion
RSA is an appropriate treatment as a revision technique for failed primary surgical treatment of PHFs. Though challenging it can offer good clinical results and pain relief.
Keywords
Introduction
Proximal humeral fractures (PHF) are the third most common fracture in people over 65 years old, behind hip and distal radius fractures, 1 and their rate is expected to rise over the following decades, due to the aging of the population. Their treatment can be challenging even for an experienced surgeon and the methods of treatment used during the past decades are numerous, ranging from nonoperative treatment or minimally invasive techniques such as closed reduction and percutaneous pinning (CRPP), intramedullary nailing (IMN) and transosseous suture fixation (TSF), to more invasive ones such as open reduction and internal fixation (ORIF) and hemiarthoplasty (HA) to even total shoulder arthroplasty (TSA) or reverse shoulder arthroplasty (RSA). However, even the most used primary techniques of ORIF and HA, have been characterized by high rates of complications and reoperation rate ranging from 13% to 34%,2–8 especially when combined with poor surgical technique, comminuted fractures and osteoporosis. 9
ORIF with the use of locking plates has been implicated in complications such as malreduction, screw cutout, malunion, nonunion, avascular necrosis, and infection,5,10 whereas HA is often associated with tuberosity malunion or resorption, impingement, periprosthetic fractures, loosening, infection, glenoid arthritis and chronic rotator cuff tears.2,11–13
All these complications can prove challenging to treat, especially when combined with poor quality of remaining tissues. For most of them RSA seems to be the only solution that can offer an opportunity for improvement in pain and function.13–26
Grammont and Baulot described the “delta” RSA as a nonanatomic approach to compensate for irreparable rotator cuff deficiencies. They medialized and lowered the glenohumeral center of rotation and this increased the lever arm of the deltoid muscle. As a result, this semi-constrained device relies on the tension of the deltoid for stability and enables elevation even with an absent rotator cuff.25,27,28 Although the initial indication of RSA was cuff deficiency, multiple indications have been suggested during the past decades, due to its increasing use and the advancements of the initial device. RSA is now widely used for cuff tear arthropathy, irreparable massive cuff tears without osteoarthritis, rheumatoid arthritis with cuff tears, acute PHFs and their sequelae and with satisfying results for revision surgery after failed fixation of PHFs or failed arthroplasties. 29
The purpose of this study was to present a case series of patients who underwent revision surgery with RSA after having a primary operative treatment for PHFs, and their clinical outcomes, in order to evaluate whether RSA can provide a satisfactory solution to this kind of devastating complications.
Materials and Methods
Patients
We present a case series of 14 patients, who were treated in the Orthopaedic Department of the University Hospital of Patras, Greece by two senior surgeons (Z.T.K. and A.P.), during a 3.5 years period (from 01/2016 until 06/2019). They were all treated for failed operative treatment of PHFs with revision surgery with RSA. Their mean age was 68 years (range, 51-84 years) and there were 8 female and 6 male patients. All patients gave written consent.
Only patients initially treated operatively, who were managed by a single-stage revision to a RTSA, and had a minimum of 12 months clinical and radiological follow-up were included. Of the patients, 6 had a PHF of the right and 8 had a PHF of the left arm. Eight patients had a 4-part PHF according to Neer classification, 4 patients had a 3-part fracture, 1 patient had a fracture-dislocation of the proximal humerus and 1 patient had suffered a head-split fracture (Table 1). 2 patients (14.3%) had been primarily treated with ORIF (1 patient with 4- and 1 patient with 3-part fracture), 5 patients (35.7%) with HA (3 patients with 4-part fracture, 1 patient with fracture-dislocation and 1 patient with head-split fracture), 3 patients (21.4%) with CRPP (2 patients with 4- and 1 patient with 3-part fracture) and 4 patients (28.6%) with TSF as described by Dimakopoulos et al. 8 (2 patients with 4- and 2 patients with 3-part fracture) (Table 2). The mean time from failed operative treatment to revision was 25.6 months (range, 5-168 months) and the complications that leaded to revision surgery were avascular necrosis (14.3%) in 1 ORIF patient and 1 CRPP patient, malunion (35.7%) in 3 TSF patients and 2 CRPP patients, nonunion (7.1%) in 1 TSF patient, screw cut-out (7.1%) in 1 ORIF patient and superior migration of the humeral head with glenoid osteoarthritis (35.7%) in 5 HA patients (Table 3).
Preoperative Characteristics of Patients Included.
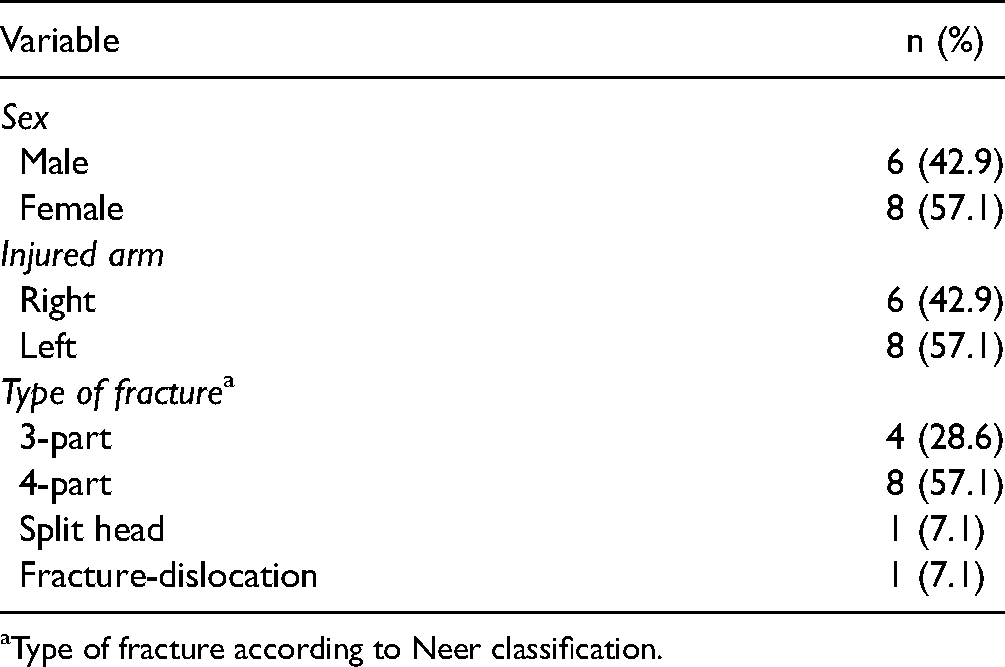
Type of fracture according to Neer classification.
Type of Primary Failed Operations.

Abbreviations: CRPP, Closed reduction and percutaneous fixation; TSF, Transosseous suture fixation; HA, Hemiarthroplasty; ORIF, Open reduction and internal fixation.
Complications Leading to Revision Surgery.

Abbreviations: AVN, Avascular necrosis; SM-OA, superior migration of the humeral head and glenoid osteoarthritis.
No patient had undergone more than 1 previous surgery.
Clinical and Radiographic Assessment
Functional results were evaluated with the Visual Analogue Scale (VAS), 30 the absolute Constant score (CS) 31 and assessment of active range of motion at the final follow-up. The mean follow-up time was 27.8 months, with a range from 24 to 36 months. Examiners different from the operating surgeons assessed the outcome in a standardized manner. Overall postoperative results were subjectively rated by the patients as poor, fair, good and excellent.
All patients were subjected to radiological assessment with the use of true anteroposterior, axillary lateral and scapular lateral radiographs.
Surgical Technique
All patients were placed in a beach-chair position, with the surgical extremity prepared in the field. The previous approach (standard deltopectoral in most cases) was used, and was extended distally when thought necessary. The axillary nerve was palpated and protected in all cases. The subscapularis and the rotator cuff—if they were in good condition—were tagged with heavy non-absorbable sutures (Orthocord sutures, DePuy Mitek Inc., Raynham MA) and mobilized in order to be reattached, after the implantation, at the humerus.
The Delta III RSA (DePuy Inc., Warsaw, IN, USA) was implanted in 3 shoulders (21.4%), the Anatomical Shoulder Reverse system (Zimmer Inc., Warsaw, IN, USA) in 4 shoulders (28.6%), the Arrow Prime RSA (FH Ortho Inc., USA) in 6 shoulders (42.9%) and the Duocentric Reversed shoulder prosthesis (Aston Medical, France) in 1 patient (7.1%). The contralateral humerus was used as template in order to define the height of the prosthetic stem.
The humeral stem had to be removed in all 5 patients (35.7%) who underwent conversion from hemiarthroplasty to RSA. In two cases of HA the humeral stem was found 40–60° retroverted. Of these 5 hemiarthroplasty cases, in two cases the humeral stem was loose and was easily removed with an impactor from below without the need for osteotomy, and then a long stem without cement was placed in one humerus (Figure 1), and a standard stem with cement in the other shoulder. In the other three HA cases the stem was well fixed and an L-type extended humeral osteotomy was performed. Three cerclage wires were passed around the humerus prior to opening the osteotomy with extreme caution not to damage the axillary and radial nerves; the distal cerclage wire was placed and directly tied, approximately 1 cm just below the end of the osteotomy, in order to prevent any periprosthetic fracture. The vertical osteotomy was performed with a narrow bladed oscillating saw, just lateral to the bicipital groove, to a point just distal to the stem or cement mantle. The transverse osteotomy was performed in the lateral direction since opening the humerus laterally is generally easier. After the L-shaped osteotomy was created into the anterior humerus, the vertical split was widened carefully using two wide osteotomes at the same time to open the humerus and to expose the intramedullary canal. The humeral implant was removed and the most of the cement mantle was carefully removed with the cement removal set (Chisels for cement removal, Aesculap Inc., Center Valley, PA). A trial stem was selected and the osteotomy was closed using the pre-placed cerclage cables. Once the glenoid was implanted, the final implant was placed into the humerus and the cables were fully tightened, securing the humerus to the implant (Figure 2).

(A, B) radiological assessment of a 53-year old male after failed primary operative treatment of slpit-humeral head fracture with hemiarthroplasty, presenting with superior migration and glenoid osteoarthritis and retroverted humeral stem. (C) Postoperative anteroposterior x-Ray of the same patient after revision surgery with uncemented—with long humeral stem—reverse shoulder arthroplasty.
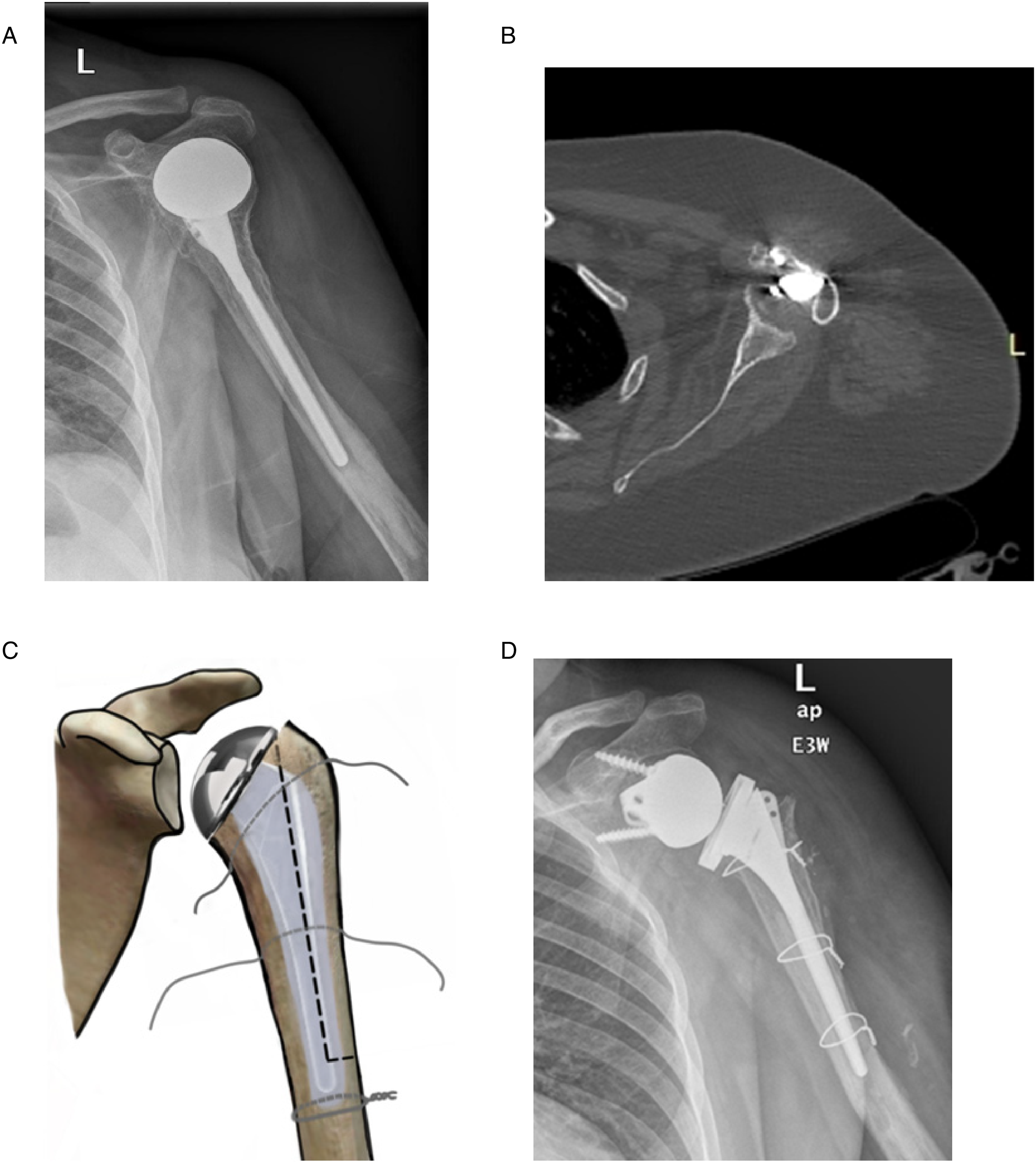
(A, B) radiological assessment of a 59-year old female patient after failed operative treatment of a 4-part proximal humeral fracture with hemiarthroplasty, presenting with superior migration and glenoid osteoarthritis and retroverted humeral stem. (C) Schematic illustration of the extended L-ytpe osteotomy of the proximal humerus that was necessary to remove the previous cemented humeral stem. Three cerclage wires were passed around the humerus prior to opening the osteotomy; the distal cerclage wire was placed and directly tied, approximately 1 cm just below the end of the osteotomy, in order to prevent any periprosthetic fracture. (2D) Postoperative anteroposterior x-Ray of the same patient after revision surgery with cemented reverse shoulder arthroplasty.
The humeral component was cemented in place in 8 cases (57.1%), while left uncemented in the remaining cases. The stem was placed with 10° retroversion in all cases. In the cases where there was malunion or nonunion of the tuberosities, the greater tuberosity was osteotomized and reattached to the implant and humeral shaft as closely as possible to its anatomic side. In 6 cases where the humeral stem was implanted uncemented, we used cancellous bone graft from the removed humeral head (Figure 3), or allograft when this was not possible.

(A, B) radiological assessment of a 51-year old female patient after failed operative treatment of a 3-part proximal humeral fracture of the left shoulder with open reduction and internal fixation, presenting with screw cut-out and postoperative glenohumeral osteoarthritis. (C) Intraoperative photograph of the glenoid, showing severe osteoarthritis. (D) Postoperative anteroposterior x-Ray of the same patient after revision surgery with uncemented reverse shoulder arthroplasty. (E, F) Clinical assessment at the final follow-up, 24 months postoperatively, during active anterior elevation and external rotation.
Statistical Analysis
Comparisons between preoperative and postoperative values of active range of motion and the absolute CS were performed with paired t test; and for pain (VAS) data, Wilcoxon signed rank test was used. The small sample size limited the power of our study to detect differences among the postoperative groups. All the analysis was performed by using GraphPad InStat (GraphPad Software Inc., San Diego, CA). The significance level was set as .05.
Results
Clinical Outcomes
The mean CS, VAS score, active anterior elevation, active abduction significantly improved compared with the preoperative status (Table 4). Whereas the difference in the above mentioned assessments was found extremely significant (P < .0001), the difference between preoperatively and postoperatively measured external rotation was found significant (P = .0304).
Clinical Assessment Preoperatively and at Final Follow-up.

Abbreviations: CS, Constant score; VAS, Visual analogue scale; ROM, range of motion; AAE, active anterior elevation; ABD, abduction; ER, external rotation.
In 3 patients (21.4%) the subjective outcome was rated as excellent, in 9 (64.3%) patients as good, in 1 (7.1%) patient as fair and 1 (7.1%) patient as poor.
No significant differences in CS, active anterior elevation and active abduction were found when comparing RSA for different failed primary techniques (P > .05).
Complications
One out of 14 patients suffered axillary nerve palsy which resulted from the primary operation and 1 patient suffered partial axillary nerve palsy, which resulted from his primary injury and remained after the 2 operations. Both of these patients underwent revision RSA due to superior migration of the humeral head and glenoid osteoarthritis after primary HA for PHF. No patient underwent further operation. There were no known infections.
Discussion
RSA has been used by many surgeons as the most appropriate method of treatment for failed primary operations after complex fractures of the proximal humerus.14–17,19,20,23–26 Cox et al. 16 studied 73 patients treated with reverse shoulder allograft-prosthetic composite after prior failed shoulder arthroplasty with associated bone loss and reported reliable pain relief and improved range of motion, with acceptable rate of complications and high patient satisfaction. Dezfuli et al. 17 categorized patients into four groups, including primary RSA and revision RSA for failed ORIF and HA and concluded that RSA is an effective treatment as both a primary and a revision procedure. However, they reported that primary RSA outperformed RSA done as a revision procedure. García-Fernández et al. 19 presented a retrospective study of patients initially treated with either ORIF or IMN, who were managed with revision to RSA and had a mean follow-up of 89 months. They concluded that although RSA is an appropriate treatment as a revision surgery for failed fixation of PHFs and patients will have improved shoulder function postoperatively, they should also be warned about the significant rate of complications following this salvage procedure (20% in their study). Another study by Grubhofer et al. 20 reviewed 43 patients with a minimum follow-up of 24 months, who underwent revision RSA due to failed ORIF after complex PHFs. They reported that RSA is a valuable salvage procedure that can offer improvement of shoulder function, patient satisfaction and pain levels, with relatively low revision rates. Hattrup et al. 22 reported results of 26 patients who had undergone RSA for the sequelae of PHFs with 15 of them having at least 1 attempt at internal fixation prior to RSA. Complications included 1 deep infection, 2 transient brachial plexopathies and 2 cases of dislocation, one of which led to revision surgery. Although complications were not infrequent, the results proved to be satisfactory in most patients. Other studies also report considerable complication rates that need to be discussed thoroughly with the patients, prior to the operation. For example, Holschen et al., 23 who studied 60 failed shoulder arthroplasties which were converted to reverse TSA, reported a complication rate of 15.9% with a revision rate of 13.6%. Another study by Hussey et al. 24 reported a complication rate of 26% with 16% revision rate among 19 patients who underwent RSA after failed internal fixation of PHFs. The complications included periprosthetic fractures in patients previously managed with IMN. Similar complication rates appear in other studies too,15,32 with the most common complication being postoperative infection. Other complications reported are persistent postoperative stiffness, dislocation, intraoperative fractures and axillary nerve palsy.
In our study, the complication rate does not agree with the previous mentioned studies, mainly because of the relatively short mean follow-up (27.8 months, range: 24-36 months) and the small sample of patients (n = 14). However 2 patients presented with axillary nerve palsy due to complications from their primary operations, a complication reported in numerous studies either as posttraumatic or postoperative complication of PHFs.14,33 We also found less statistical difference in external rotation when comparing the postoperative to the preoperative status (P = .0304), as opposed to the extremely significant difference (P < .0001) found for mean CS, VAS score, active anterior elevation and active abduction. This particular fact is also described in bibliography, as it is supported that little or no improvement in external rotation can be succeeded with RSA, because the prosthesis cannot substitute for the external rotation function of the posterior part of the rotator cuff. The center of rotation is also medialized, decreasing the effectiveness of the posterior deltoid as secondary external rotator when combined with abduction. 34
There are limitations associated with this study, including the retrospective design, the number of patients (n = 14), the relatively short follow-up (mean: 27.8 months), the various primary procedures and reasons for failure, the use of different implants for the revision surgery and the single point of follow-up. However, the advantage of our study is that it was performed at a single university hospital by two senior surgeons using a similar technique.
Conclusion
RSA is an appropriate treatment as a revision technique for failed primary surgical treatment of PHFs, that can offer improved shoulder function and pain relief. It is a technically demanding procedure, which should be performed by experienced surgeons and after a thorough discussion with the patient regarding the expected outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.